Practice Essentials
Patulous tube is a troublesome but benign condition in which the eustachian tube remains abnormally patent. Schwartze first described patulous eustachian tube in 1864 when he noted a scarred atrophic eardrum moving synchronously with respiration. This condition was first fully described in 1867 by Jago, who had a patulous eustachian tube. [1]
Workup in patulous eustachian tube
Computed tomography (CT) scanning in an axial plane has been used to show the presence of a patulous eustachian tube.
Tympanometry may detect movements of the tympanic membrane with nasal respiration, especially with the patient in an erect position. [2]
Distorted sounds of nasal respiration and speech may be heard with a microphone placed in the external meatus.
In some patients with patulous tube, direct nasopharyngoscopy may show the continuous presence of a triangular opening of the eustachian tube orifice.
Management of patulous eustachian tube
The following methods may be used for treatment of a narrow lumen caused by an inflammatory response or scar tissue:
-
Bezold's remedy of insufflation of a solution of salicylic acid and boric acid (1:4 ratio) - Repeat treatments are always necessary
-
Eustachian tube diathermy with sequential application of ureteric diathermy probe
-
Cautery with 20% silver nitrate
The following methods may be used for treatment of a narrow lumen caused by extrinsic compression:
-
Paraffin injection
-
Teflon injection anterior to the eustachian tube orifice
-
Gelfoam injection
-
Alter function of palatal muscles, with or without pterygoid hamulotomy
-
Occlusion of the eustachian tube
-
Myringotomy and insertion of a ventilating tube
-
Surgical scar tissue removal in nasopharynx
Epidemiology
Frequency
Incidence of patulous eustachian tube is 0.3-6.6%, and 10-20% of persons who have it are bothered enough by symptoms to seek medical attention. This condition is more common in females than in males and is usually present in adolescents and adults; it is rarely found in young children.
See the image below.
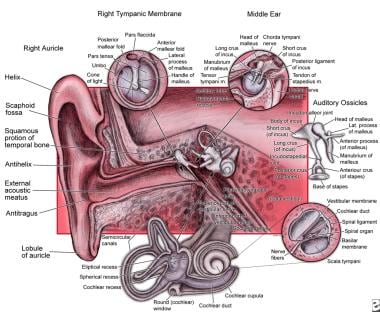 Anatomy of the ear.
Anatomy of the ear.
Etiology
In most instances, patulous eustachian tube is idiopathic. Weight loss (sometimes caused by chronic illness) and pregnancy are identified as important predisposing factors. Neurologic disorders that may cause muscle atrophy (eg, stroke, multiple sclerosis, motor neuron disease) have been implicated. Adhesion formation in the nasopharynx following adenoidectomy or radiotherapy may also predispose individuals to a patulous tube. The condition is sometimes associated with medications (eg, oral contraceptives, diuretics). Other predisposing factors include fatigue, stress, anxiety, exercise, and temporomandibular joint syndrome.
On the other hand, in a study using computed tomography (CT) scanning to compare the bony portion of the eustachian tube of patients with patulous eustachian tube with that of controls, Ikeda et al found the shape to be almost identical, indicating that this part of the structure exercises no pathologic influence on patulous eustachian tube. [3]
Pathophysiology
Under normal resting conditions, the eustachian tube is closed and only opens with swallowing or autoinflation. In unaffected individuals, closure of the eustachian tube is maintained by luminal and extraluminal factors, which include intrinsic elasticity of the tube, surface tension of moist luminal surface, and extraluminal tissue pressure. Muscle tone of tensor veli palatini dilates the lumen; damage to tensor veli palatini following cleft palate surgery may produce a patulous tube. Weight loss can also lead to abnormal patency caused by reduced tissue pressure and loss of fat deposits in the eustachian tube region. Pregnancy alters opening pressures of the eustachian tube because of the change in surface tension; estrogens acting on prostaglandin E affect surfactant production. Scarring in the postnasal space following adenoidectomy may result in traction of the tube in a patent position.
Presentation
History
Major symptoms of patulous eustachian tube include fluctuating aural fullness, roaring tinnitus synchronous with nasal respiration, audible respiratory sounds, distorted autophony (ie, the abnormal perception of one's own breath and voice sounds) with echoing occasionally severe enough to interfere with speech production, and sensation of plugged ear. Autophony is the most frequent symptom associated with patulous tube. [4]
Vertigo and hearing loss can also occur because patulous eustachian tube allows excessive pressure changes to occur in the middle ear; these pressure changes are then transmitted to the inner ear through ossicular movement. Some patients may have difficulty eating because the noise of chewing is transmitted to the ear. Patulous eustachian tube is often misdiagnosed because symptoms mimic those of middle ear effusion. Symptoms may relate to cyclical changes occurring in the mucosa of the eustachian tube. Some patients find relief from the associated increased mucosal congestion by lying down, by putting the head between the knees, or during upper respiratory tract infection.
Compression of the jugular veins produces peritubular venous congestion and may relieve symptoms. Patients sometimes sniff repetitively to close the eustachian tube, and this may lead to long-term negative middle ear pressure. Decongestants or a ventilation tube in the drum can worsen symptoms.
Diagnosis can often be made based on history alone.
Physical examination
Examination findings are usually unremarkable; canals and eardrums appear normal. The eardrum can be atrophic secondary to the constant drum motion from breathing or sniffling. Synchronous movement of the tympanic membrane with respiration is exaggerated with forced respiration or with the patient breathing in and out through the nose with one nostril occluded; the tympanic membrane moves medially on inspiration and laterally on expiration. With the patient sitting upright, small movements of pars flaccida occur, which disappear when the patient is supine. Examine the ear with an operating microscope to detect subtle movements.
Indications
Surgery is indicated if the patient continues to have significant otologic symptoms despite medical therapy.
Contraindications
Surgical therapy for a patulous eustachian tube is contraindicated in patients who are pregnant or have mild symptoms. These patients need informative reassurance alone (see Medical Therapy).
-
Anatomy of the ear.





