Practice Essentials
Middle ear and eustachian tube inflammation are common denominators in various clinical conditions, namely, acute otitis media (AOM), chronic otitis media with effusion (COME), and eustachian tube dysfunction (ETD). [1, 2, 3]
Symptoms related to middle ear/eustachian tube inflammation/infection
These include the following:
-
Eustachian tube dysfunction (ETD) - Symptoms usually follow the onset of an upper respiratory tract infection (URTI) or allergic rhinitis; [4] symptoms include aural fullness, difficulty popping ears, intermittent sharp ear pain, hearing loss, tinnitus, and disequilibrium
-
Otitis media (OM) - Acute otitis media (AOM) can also be observed following URTI or secondary to any cause of eustachian tube inflammation or blockage; symptoms include otalgia, hearing loss, fever, and disequilibrium
-
Chronic otitis media with effusion (COME) - Symptoms include hearing loss, tinnitus, and disequilibrium; COME is not associated with fever; children may have speech/language delay
Workup
The workup should include a complete exam of the upper respiratory tract, including the tympanic membrane, nasopharynx, and larynx (if the etiology is in question and the diagnostic tools are available). A pneumatic otoscope is essential for an accurate assessment of the middle ear.
An impedance measurement (tympanogram) is an indirect measurement of eustachian tube and middle ear function that suggests the presence or absence of effusion or pressure in the middle ear space.
Audiometry is critical in determining any temporary effects that middle ear fluid may have on hearing sensitivities.
The Eustachian Tube Dysfunction Questionnaire (ETDQ-7) is a validated symptom score utilized to quantify the severity of eustachian tube dysfunction. [5]
Rarely needed, a computed tomography (CT) scan of the temporal bone is useful to evaluate for extracranial complications of otitis media (OM). A magnetic resonance imaging (MRI) study is useful to evaluate for intracranial complications of otitis media (OM).
Management
In the United States, acute otitis media (AOM) is typically treated with antibiotics. [6] Treatment with amoxicillin for 10 days is the initial antibiotic therapy, or Bactrim is substituted if the patient is allergic to penicillin. In Europe, a more conservative approach to treating acute otitis media (AOM) is used. Given the alarming increase in antibiotic resistance, the routine usage of antibiotics in the United States should be reconsidered.
In the United States, otitis media with effusion (OME) can be treated with observation, antibiotics, or tympanostomy tube placement. However, a meta-analysis of controlled studies revealed only a 14% increase in the resolution rate when antibiotics are given. [7, 8] Antibiotic suppression is not indicated for OME, and multiple courses of antibiotics have no proven benefit. Consider surgical intervention after 3-4 months of effusion with a 20 dB or greater hearing loss. [9]
Eustachian tube dysfunction (ETD) can be treated primarily with a combination of time, autoinsufflation (eg, an Otovent), and oral and nasal steroids (budesonide, mometasone, prednisone, methylprednisolone).
Nasal and oral antihistamines can be beneficial in patients with allergic rhinitis. Leukotriene antagonists (eg, montelukast sodium [Singulair]) are helpful in some patients when oral steroids are not an option. Adequate control of laryngeal pharyngeal reflux helps to resolve eustachian tube dysfunction (ETD) in patients with an associated peritubal inflammation from reflux. Proton pump inhibitors (esomeprazole magnesium [Nexium], rabeprazole [Aciphex], omeprazole [Prilosec]) administered twice a day are often used.
The primary surgical treatment of all types of otitis media (OM) is myringotomy with tube placement. [10] The typical ventilation tube stays in place for a period of 8-12 months, with closure of the perforation occurring after tube extrusion. In a small percentage of patients with poor eustachian tube function or other complicating factors, the perforation may persist.
Adenoidectomy is indicated for refractory otitis media with effusion (OME) in children older than 4 years and in younger children when adenoid pathology is present (eg, chronic adenoiditis, adenoid hypertrophy).
A newer technique, endoscopic eustachian tube dilation, has been utilized in patients as young as age 4 years in Europe and in patients older than 18 years in the United States. [11]
Pathophysiology
Acute otitis media (AOM) can be described on the cellular and molecular level as a transudation of neutrophils, serum, and inflammatory mediators into the middle ear space. This transudation is associated with mucosal edema of the middle ear and bacterial or viral infection of the eustachian tube and middle ear space.
Chronic otitis media (COM) involves a transudation of serum with less cellularity of the effusion material. The inflammatory mediators are less destructive, and bacteria and viral antigens may be less prevalent. See the image below.
Epidemiology
Frequency
United States
Otitis media (OM) is the most common diagnosis made by office-based physicians of children younger than 15 years. Otitis media (OM) is the most common reason children are prescribed antibiotics and the most common indication for surgery in children.
A study by Hasegawa et al, using a cross-sectional analysis of the Nationwide Emergency Department Sample, found that otitis media was the second most common cause of infectious disease – related emergency department visits in the United States in 2011. The study found that otitis media was diagnosed in 18% of such cases, compared with upper respiratory infection in 41% of cases. [12]
International
Rates of otitis media (OM) equal to or higher than rates in the United States are noted internationally, especially in less developed countries. A delay is evident in the peak incidence of otitis media (OM) in European children, which may be attributable to the fact that European children enter childcare at a later age.
Mortality/Morbidity
In the era of modern medicine, middle ear infection rarely leads to mortality, except in rare cases of intracranial spread of infection.
Eustachian tube dysfunction (ETD) and chronic otitis media with effusion (COME) affect 70% of children by age 7 years and are common causes of childhood hearing loss. Morbidity from otitis media (OM) primarily stems from the effect on hearing. In most cases the conductive hearing loss is entirely reversible with medical or surgical treatment. Children may have a speech/language acquisition delay from recurrent acute otitis media (AOM) or chronic otitis media with effusion (COME).
Otitis media (OM) has not clearly been shown to affect the long-term acquisition of language skills in children; however, studies have predicted that early recurrent otitis media (OM) and chronic otitis media with effusion (COME) may be predictive of future decreases in hearing as measured by school screening tests and a decrease in overall school achievement. These findings suggest a possible long-term effect on the central auditory pathway.
Race
American Indian and Native Alaskan children, including the Inuit, have higher rates of chronic otitis media (COM) than whites. Hispanic children have higher rates of otitis media (OM) than either whites or African American children.
The prevalence of chronic suppurative otitis media (OM) is highest in Inuits of Alaska, Canada, and Greenland; Australian Aborigines; and in American Indians. High prevalence is also found in Pacific Islanders and Africans. Low prevalence is found in residents of Korea, India, and Saudi Arabia. The lowest prevalence is found in residents of the United States, United Kingdom, Denmark, and Finland.
Sex
Males have a higher prevalence of acute otitis media (AOM) and undergo myringotomies and tympanoplasties more frequently than females do.
Age
Middle ear dysfunction and eustachian tube dysfunction (ETD) are more common in the pediatric age group. Peak incidence of otitis media (OM) is in the first 2 years of life. [13]
-
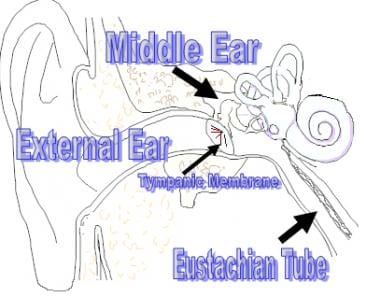
Anatomy of the external and middle ear.
-
Eustachian tube dilation procedure, prior to insertion of balloon.
-
Insertion of balloon in eustachian tube dilation.









