Practice Essentials
Preauricular cysts, pits (as shown below), fissures, and sinuses are benign congenital malformations of the preauricular soft tissues first described by Van Heusinger in 1864. Preauricular pits or fissures are located near the front of the ear and mark the entrance to a sinus tract that may travel under the skin near the ear cartilage. These tracts are lined with squamous epithelium and may sequester to produce epithelial-lined subcutaneous cysts or may become infected, leading to cellulitis or abscess. Complete surgical excision of a preauricular sinus tract or cyst is indicated in the setting of recurrent or persistent infection.

Preauricular tags, as shown below, are epithelial mounds or pedunculated skin that arise near the front of the ear around the tragus. They have no bony, cartilaginous, or cystic components and do not communicate to the ear canal or middle ear.

Simple preauricular cysts should not be confused with first branchial cleft cysts. Branchial cleft anomalies are closely associated with the external auditory canal, tympanic membrane, angle of the mandible, and/or facial nerve. Misinterpreting a first brachial abnormality for a simple sinus tract may place the unsuspecting physician at risk for damaging the facial nerve, incompletely excising the lesion, or both.
Patients identified with preauricular pits or cysts should be examined for other congenital anomalies.
Workup in preauricular cysts, pits, and fissures
With regard to laboratory studies, culture samples may be obtained during drainage procedures.
Imaging is not indicated for routine preauricular cysts and sinuses. However, it is indicated in patients who present with pits or fistulas located in atypical regions, those with cartilage duplication around the external auditory canal that extends into the parotid, and those with recurrent parotid swelling. Patients who have preauricular cysts or pits and a branchial cleft cyst should undergo renal ultrasonography to rule out branchio-oto-renal syndrome.
Management of preauricular cysts, pits, and fissures
Antibiotics (eg, cephalexin [Keflex], amoxicillin and clavulanate potassium [Augmentin], erythromycin) are indicated in patients with cellulitis from infected preauricular pits.
Incision and drainage procedures may be required for patients with abscess formation. Staphylococcus aureus is the most common bacteria found in these infections, followed by Proteus, Streptococcus, and Peptococcus species.
The authors discourage standard incision and drainage in the setting of abscess formation within a preauricular sinus tract or cyst. A potential alternative to incision and drainage is the use of a blunt-ended lacrimal probe inserted into the preauricular pit in order to open the abscess cavity. However, acute inflammation usually makes this option technically difficult and painful. Aspiration with a 21-gauge needle reliably provides at least temporary relief, eases pain, and provides purulent material for culture and sensitivity. Needle aspiration may need to be repeated if an abscess reaccumulates, but this procedure reliably leads to a better cosmetic result than incision and drainage.
Complete surgical excision of a preauricular sinus tract or cyst is indicated in the setting of recurrent or persistent infection. The operation is typically performed when the acute infection has subsided. Recurrence rates following excision range from 0-42%. Factors that reportedly reduce the risk of recurrence include complete excision of the sinus and tract with associated perichondrium, dissection down to temporalis fascia, closure of dead space, and avoidance of sinus rupture.
Epidemiology
Frequency
Malformations of the external ear are not uncommon. Generally, they occur in 1 of every 12,500 births. Incidence of spontaneous formation of ear pits in the nonsyndromic population ranges from 0.3-0.9%. (These conditions affect males and females equally and have no race predilection.)
A Korean study that assessed data from 23,533 individuals found the incidence of unilateral and bilateral preauricular sinuses to be 1.3% and 0.3%, respectively. The adjusted odds ratio for having bilateral sinuses was higher in children of a parent with bilateral sinuses, but the same was not true for unilateral sinuses. No association was found between preauricular sinuses and hearing impairment. [1]
Another Korean study, by Lee et al, estimated the overall prevalence of preauricular sinuses in South Korea to be 1.91%, with these occurring unilaterally in 79.08% of cases. The study, which involved a survey of 56,592 individuals, found the prevalence to be highest in females. [2]
Etiology
Embryology and branchial arch development
The auricle forms during the sixth week of gestation. The first and second branchial arches give rise to a series of 6 mesenchymal proliferations known as the hillocks of His, which fuse to form the definitive auricle. The first arch gives rise to the first 3 hillocks, which form the tragus, helical crus, and the helix. The second arch gives rise to the second 3 hillocks, which form the antihelix, scapha, and the lobule.
Defective or incomplete hillock fusion during auricular development is postulated as the source of the preauricular sinus. Another theory suggests that localized folding of ectoderm during auricular development is the cause of preauricular sinus formation. The first 3 hillocks are most often linked to supernumerary hillocks, leading to preauricular tag formation.
Genetics
Correct sequential gene activation is required for normal ear and facial development. Interrupting the gene activation sequence in laboratory animals disrupts ear development.
Genetic linkage analysis studies have suggested that congenital preauricular sinus localizes to chromosome 8q11.1-q13.3. [3]
The inner neurological hearing apparatus, cochlea, and auditory nerve form in conjunction with the outer ear structures during the early developmental stages. External deformities may be associated with an inner neurological deformity and, hence, suggest a possible deafness.
Associated syndromes
Syndromic expression of pits, tags, and fissures occurs at much higher frequencies in certain craniofacial dysmorphisms. Minor anomalies of the head and neck may aid the clinician in developing a presumptive diagnosis during the initial examination. Additional ear anomalies include helical fold abnormalities, asymmetry, posterior angulation, small size, absent tragus, and narrow external auditory meatus. Some syndromes with characteristic ear anomalies are as follows:
-
Branchiootorenal syndrome (BOR) - Preauricular sinus
-
Beckwith-Wiedemann syndrome - Preauricular sinus with asymmetric earlobes
-
Mandibulofacial dysostosis - Auricular pits/fistulas
-
Oculoauriculovertebral dysplasia - Preauricular tags (see the image below)
 Multiple tags in a child with oculoauriculovertebral dysplasia. Note the hemifacial atrophy, retrognathia, and lower set ear. Image courtesy of Jack Yu, MD.
Multiple tags in a child with oculoauriculovertebral dysplasia. Note the hemifacial atrophy, retrognathia, and lower set ear. Image courtesy of Jack Yu, MD.
-
Chromosome arm 11q duplication syndrome - Preauricular tags or pits
-
Chromosome arm 4p deletion syndrome - Preauricular dimples or skin tags
-
Chromosome arm 5p deletion syndrome - Preauricular tags

A study by Beleza-Meireles et al of clinical phenotypes in 51 patients with oculoauriculovertebral dysplasia found ear abnormalities in 47 (92%) of them (unilateral: 24 patients; bilateral: 23 patients). [4]
Medication
A study by Andersen et al suggested that the occurrence of birth defects in the face and neck region, including preauricular cysts, may be linked to the use of propylthiouracil in early pregnancy to treat maternal hyperthyroidism. In a review of records from more than 1.6 million children born in Denmark between 1996 and 2008, the investigators concluded that in terms of having a birth defect in the head or neck region—specifically, a preauricular or branchial sinus, fistula, or cyst—children exposed to propylthiouracil had a hazard ratio (HR) of 4.92. These same children also had an HR of 2.73 for a urinary system birth defect (single renal cyst, hydronephrosis). Possible propylthiouracil-related birth defects were found in a total of 14 children, including three whose mothers were initially given methimazole/carbimazole but were switched to propylthiouracil in early pregnancy. [5]
Pathophysiology
Preauricular sinuses may be asymptomatic for life. An infection arises in cases of preauricular sinus when the opening of the pit seals bacteria within the sinus tract along with desquamated skin. Early signs and symptoms of swelling, pain, and erythema should prompt the practitioner to begin antibiotic therapy directed at common skin bacterial organisms. Surgical drainage may be indicated if there is recurrent drainage from a preauricular pit, [6] obvious abscess formation occurs or swelling progresses despite antibiotic therapy. Toxic-appearing and immunocompromised patients may require observation, intravenous antibiotic therapy, and surgical drainage. Complete surgical removal is the treatment of choice for recurrent infection and drainage problems. The aforementioned Korean study did not find preauricular sinuses to be associated with hearing impairment. [1]
Ear tags alone pose no threat to any structure and are usually merely a cosmetic deformity. They are usually excised in young patients by qualified surgeons who treat head and neck abnormalities. General anesthesia is typically required. Recurrence rates are low.
Smaller, narrowly based tags are tied at their bases with thread or suture in infants during office visits. Simple excision at the base may be performed using topical EMLA cream. Larger, broad-based, multiple, or complex tags may require elliptical excision and plastic closure, which requires general anesthesia.
Presentation
Clinical presentation of various ear anomalies may be summarized as follows:
-
Noninfected pits - Pinpoint hole in front of the ear or above tragus, as shown below
Nondraining
Lacks swelling
-
Infected pits - Cellulitis and abscess
Red, swollen
Draining purulent material
Granulation around pit
Tender
Previous surgical scar with underlying swelling
-
Cysts - Slowly enlarging preauricular mass
Usually nontender if uninfected
Associated pit usually adjacent to cyst, as shown below
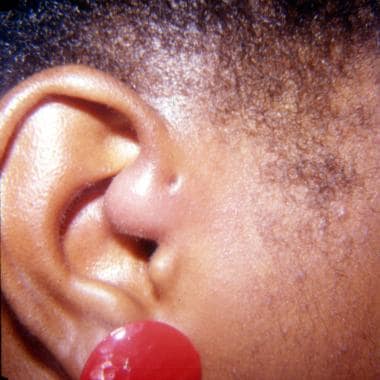 Infected preauricular cyst with swelling and erythema toward the cartilage of the ear.
Infected preauricular cyst with swelling and erythema toward the cartilage of the ear.
-
Tags - Fleshy knobs of skin in front of the ear
Nontender
Nondraining
Color similar to surrounding skin
Appears to be attached on the surface of the cheek, pinna, tragus, or lobe
No rapid growth


Differential diagnoses
See the list below:
-
Preauricular swelling/infection
-
Parotid swelling/mass/tumor
-
First branchial cleft cyst
-
Duplication of ear canal
-
Trauma
-
Cellulitis from otitis externa
-
Trauma
-
Body piercing
-
Previous surgical site
Indications
Most patients with preauricular pits in the typical location are asymptomatic and require no surgical intervention. Needle aspiration is indicated for abscess that fails to respond to antibiotics. Incision and drainage complicates later excision and should be reserved for abscess that recurs after needle aspiration.
Complete excision of the cyst or sinus tract may be undertaken in cases of recurrent infection.
Ear tags are removed for cosmetic reasons.
Relevant Anatomy
A preauricular pit may mark the entrance to a sinus tract, which can vary in length, follow a tortuous course, and branch extensively. Preauricular sinuses and cysts have a component of close association with the auricular perichondrium. For this reason, some argue that complete removal of a sinus tract or cyst should also include a portion of the auricular perichondrium at the base of the lesion.
Preauricular sinuses or cysts are found lateral and superior to the facial nerve and parotid gland, whereas first branchial cleft malformations are found in close association with these structures, as well as with the external auditory canal.
Excision of complex or broad-based tags requires the knowledge of relaxed skin lines and wound tension in the region of the face and ear.
Contraindications
An infected cyst or tract may be considered a relative contraindication to excision of a sinus tract or cyst. Antibiotics and, occasionally, steroids should be considered to control any residual inflammation prior to surgery.
-
Preauricular ear tag. Image courtesy of Jack Yu, MD.
-
Multiple tags in a child with oculoauriculovertebral dysplasia. Note the hemifacial atrophy, retrognathia, and lower set ear. Image courtesy of Jack Yu, MD.
-
Uninfected preauricular pit. Image courtesy of Ed Porubsky, MD.
-
Close-up image of preauricular pit. Image courtesy of Ed Porubsky, MD.
-
Infected preauricular cyst with swelling and erythema toward the cartilage of the ear.
-
A preauricular sinus tract is probed with a blunt needle, and methylene blue dye is injected. Note the region in front of the pit, where previous abscess formation, spontaneous drainage, and residual scarring and granulation have occurred. This circumstance requires a more complex procedure. Removal of the entire sinus tract and the granulation disease is essential. Image courtesy of Ed Porubsky, MD.
-
Preauricular sinus tract, cyst, and granulation removed. The skin was closed with slight undermining and no tension. Sutures are removed 7-10 days later.
-
Keloid scar formed several months after removal of preauricular sinus tract. Intralesional steroids and close observation are indicated.





