Practice Essentials
Otalgia is defined as ear pain. Two separate and distinct types of otalgia exist. Pain that originates within the ear is primary otalgia; pain that originates outside the ear is referred otalgia. [1, 2]
Typical sources of primary otalgia are external otitis, otitis media, mastoiditis, and auricular infections. Most physicians are well trained in the diagnosis of these conditions. When an ear is draining and accompanied by tympanic membrane perforation, simply looking in the ear and noting the pathology can make the diagnosis. When the tympanic membrane appears normal, however, the diagnosis becomes more difficult.
Referred otalgia is a topic unto itself. Although many entities can cause referred otalgia, their relationship to ear pain must be identified. A categorical discussion of the workup, treatment, prognosis, demographics, and other issues is impossible because the various pathologies responsible for creating referred otalgia are so diverse.
Reports document that not all otalgia originates from the ear. Many remote anatomic sites share dual innervation with the ear, and noxious stimuli to these areas may be perceived as otogenic pain. By definition, referred otalgia is the sensation of ear pain originating from a source outside the ear.
To better understand referred otalgia, the physician first must understand the anatomic distribution of nerves associated with the ear. Irritation of these nerves, as well as irritation of distant branches of these nerves, can cause the perception of pain within the ear.
The picture below demonstrates the diversity of pathologies that can be the source of referred otalgia.
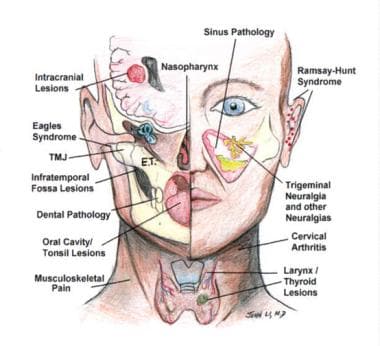 This picture demonstrates the diversity of pathologies that can be the source of referred otalgia.
This picture demonstrates the diversity of pathologies that can be the source of referred otalgia.
Workup in otalgia
Frequently, the workup suggests that otalgia may be a problem of dental origin.
A complete blood count may indicate an occult infection. Thyroid function and erythrocyte sedimentation rate (ESR) studies may reveal thyroiditis and temporal arteritis.
The perception of aural fullness may be described as ear pain and is observed in conditions associated with endolymphatic hydrops and Eustachian tube dysfunction. [3]
Ménière disease can be diagnosed by history, audiometrics, and a battery of laboratory tests.
In the absence of obvious fluid within the middle ear, aural fullness secondary to Eustachian tube dysfunction may manifest with a practically imperceptible bulging or retraction of the tympanic membrane. If autoinsufflation is not effective in relieving this pressure, consider a diagnostic myringotomy.
Imaging studies can include the following:
-
Dental radiography
-
Chest radiography
-
Computed tomography (CT) scanning
-
Magnetic resonance imaging (MRI)
-
Panorex imagery
-
Positron emission tomography (PET) scanning
Other tests include the following:
-
Audiography
-
Vestibulocochlear testing
-
Nasal endoscopy
-
Upper aerodigestive tract endoscopy, laryngoscopy
-
Blood tests
When the history and physical examination findings are inconclusive, use of local anesthesia may help localize the problem.
Management of otalgia
Identification of a causative etiology is often necessary to successfully treat referred otalgia. Once determined, most causes of referred otalgia can be readily treated.
Use antibiotics in treating various types of infections (eg, tonsillitis, pharyngitis, sinusitis). Use antivirals if the causative agent is suspected to be viral, such as in cases associated with herpes zoster or shingles. Antifungals are indicated if the source is caused by a fungus (eg, oral thrush/candidiasis). Antiulcer/antacid medications can be used for esophagitis and gastroesophageal reflux disease. Use nonsteroidal anti-inflammatory drugs (NSAIDs) when myalgias and neuralgias are suspected. Reexamine the patient after a 2-week trial of NSAIDs.
Strong narcotic analgesics are not indicated and should not be used to treat referred otalgia. Narcotics may mask symptoms, making the correct diagnosis difficult to reach.
Pathophysiology
The sensory innervation of the ear is served by the auriculotemporal branch of the fifth cranial nerve (CN V), the first and second cervical nerves, the Jacobson branch of the glossopharyngeal nerve, the Arnold branch of the vagus nerve, and the Ramsey Hunt branch of the facial nerve. Neuroanatomically, the sensation of otalgia is thought to center in the spinal tract nucleus of CN V. Not surprisingly, fibers from CNs V, VII, IX, and X and cervical nerves 1, 2, and 3 have been found to enter this spinal tract nucleus caudally near the medulla. Hence, noxious stimulation of any branch of the aforementioned nerves may be interpreted as otalgia.
Epidemiology
In a study of US emergency department (ED) patients with otologic complaints, Kozin et al found that the most commonly diagnosed conditions were otitis media not otherwise specified (NOS) (60.6%), infected otitis externa NOS (11.8%), and otalgia NOS (6.8%). The data was drawn from a weighted total of 8,611,282 ED visits for otologic problems between 2009 and 2011. [4]
In a Korean study of 294 patients with otalgia, the prevalence of primary otalgia was found to be higher in children than in adults and in men than in women, while referred otalgia was more likely to occur in adults in general and in women in particular. The study, by Kim et al, also found that neuralgia occurred more frequently in women than in men with referred otalgia. [5]
-
This picture demonstrates the diversity of pathologies that can be the source of referred otalgia.









