Practice Essentials
Nasal fractures are the most common types of facial fractures; however, they are often unrecognized and untreated at the time of injury. Its central position and anterior projection on the face predisposes the nose to traumatic injury. Studies have shown that most nasal fractures involve the septum, which can be an obstacle to successful reduction. [1]
Fractures can be classified as open or closed, depending on the integrity of the mucosa. Prompt identification and management of the injury in the early postinjury period is imperative to avoid the potential complications of nasal and septal fractures. Confirming that septal hematoma is not present is crucial to avoid further compressive damage to native tissue and dangerous infectious complications. Longer-term follow-up allows the surgeon to assess for both early and late sequelae of injuries to the nasal complex. Surgical intervention may be appropriate in the early postfracture period or much later, after the fracture has healed. [2]
An oblique view of nasal fractures is depicted below.
Signs of nasal fractures
Clinical findings in patients with a history of trauma to the nose or face may include the following [3] :
-
Epistaxis, which is common in nasal fractures due to mucosal disruption
-
Change in nasal appearance
-
Nasal airway obstruction
-
Infraorbital ecchymosis
Workup in nasal fractures
The use of radiography is controversial in the workup of nasal and septal fractures. Old fractures, vascular markings, and suture lines can lead to false-positive results.
Computed tomography (CT) scanning is useful to assess for associated injuries, as well as the extent of nasal injury. Septal fractures may be more obviously depicted on these films.
Photographs are useful and necessary for documentation and for comparison with preinjury photos.
Management of nasal fractures
Elevation of the head and use of cold compresses in the periorbital and nasal region can be helpful while waiting for edema to subside.
Regarding surgery, no clear recommendation exists regarding the type of operative approach or the timing of surgery in patients with nasal fractures.
Studies have shown that as the significance of the nasal deviation increases, successful reduction of the nasal fracture becomes more difficult. The literature indicates a significant dissatisfaction with closed reduction results, suggesting that open approaches may reduce the need for future revision procedures.
Dorsal nasal reconstruction with rib graft or calvarial bone grafts is necessary in patients with severe nasal injuries, significant saddle-nose deformity, loss of dorsal projection, and shortened nasal length.
Epidemiology
Frequency
Nasal fractures are the third most common types of fractures, behind fractures of the clavicle and wrist. Nasal fractures are often cited as the most common type of facial fracture, accounting for approximately half of all facial fractures in several studies. Zygomatic (22%), blowout (12%), mandibular bone (8%), and maxillary bone (9%) fractures follow in frequency.
A British study, by Gupta et al, found at a major trauma center that the coronavirus disease 2019 (COVID-19) pandemic may have reduced the number of patients coming to the emergency department for treatment of nasal fractures. The investigators reported that the number of patients presenting with suspected or confirmed nasal fractures in 2020 was 51.4% less than in 2019. [4]
Etiology
Most commonly, nasal bone fractures are sustained in fights (34%), accidents (28%), and sports (23%). A 2009 study of 236 patients with facial fractures incurred while playing sports determined that fractures of the nasal bone were most common. [5]
With increasing use of air bags in automobiles, a shift in the mechanism of injury and the type of nasal fractures has occurred; therefore, the incidence of septal injury in nasal fractures, without concurrent nasal bone fracture, has increased.
In a study of 2023 adults with facial fracture, including 209 patients over age 64 years, Atisha et al determined that nasal fractures were more common in elderly persons than in nonelderly ones (54.1% vs 45.3%, respectively). [6]
In children, nasal fractures are most commonly due to falls. In a study of 100 children with traumatic nasal deformity, Liu et al determined that such injuries were most often the result of sports-related trauma (28%), with accidental trauma (21%), interpersonal violence (10%), motor vehicle collisions (6%), and alcohol-related trauma (2%) being the next most common reasons for injury. [7] The possibility of child abuse should be considered in every child presenting with a nasal fracture.
A Korean study, by Yu et al, found that among 2321 patients, nasal fractures were most commonly caused by violence (31%), but that in patients under age 12 years, only a small minority sustained nasal fractures in this manner, with, as also indicated in the above paragraph, slips/falls and sports-associated trauma being the most frequent causes in these children. No violence-related nasal fractures were found in patients under age 10 years. The investigators also reported that, while plane 2 fractures sustained via lateral force were more common than plane 1 or 2 fractures occurring by way of frontal impact (54.45% vs 36.84%), frontal impact was the more common culprit in patients under age 12 years. [8]
Pathophysiology
The direction of force to the nose during injury determines the pattern of the fracture.
-
Frontal force causes damage ranging from simple fracture of the nasal bones to flattening of the entire nose.
-
Lateral force may depress only one nasal bone; however, with sufficient force, both bones may be displaced. Lateral force can cause severe septal displacement, which can twist or buckle the nose. Septal fragments may interlock, creating further difficulty in reduction.
-
Superior-directed force (from below) rarely occurs. It may cause severe septal fractures and dislocation of the quadrangular cartilage.
Presentation
Clinical findings in patients with a history of trauma to the nose or face may include the following [3] :
-
Epistaxis, which is common in nasal fractures due to mucosal disruption
-
Change in nasal appearance
-
Nasal airway obstruction
-
Infraorbital ecchymosis
Indications
Indications for repair of nasal fractures include abnormal nasal function, abnormal appearance, and presence of early postinjury complications. Several methods of reduction and repair can be performed to achieve good cosmetic and functional results. [9]
-
Closed reduction may be performed under local anesthesia or local anesthesia with mild sedation. Indications include the following [10] :
Simple fracture of nasal bones
Simple fracture of nasal-septal complex
-
Open reduction requires deeper sedation or a general anesthetic. Indications include the following:
Extensive fracture-dislocation of nasal bones and septum
Fracture dislocation of caudal septum
Open septal fractures
Persistent deformity after closed reduction
Relative indications, eg, septal hematoma, inadequate bony reduction due to septal deformity, cartilaginous deformities, displaced nasal spine, and recent intranasal surgery
Relevant Anatomy
See the list below:
-
Nasal skin has an abundant blood supply and tends to be thinner over the rhinion and thicker over the nasion. Nasal skin thickness varies among individuals.
-
The nasal pyramid is composed of 2 nasal bones and the frontal process of the maxilla. The thickness of the bones decreases toward the tip of the nose; as a result, most fractures occur in the lower half.
-
Upper lateral cartilages form the middle nasal vault. Upper lateral cartilages are attached to the nasal bones superiorly, the quadrangular cartilage of the septum medially, and the lower lateral cartilages (ie, tip cartilages) inferiorly.
-
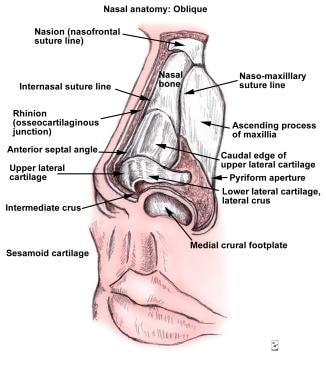
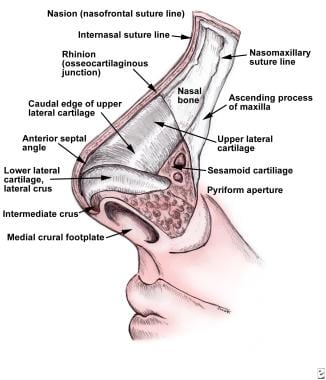
The images below depict the oblique and lateral view of the nasal anatomy.
-
Sesamoid cartilages are less important and lie in the fat pad between lower lateral cartilages and the piriform aperture.
-
The nasal septum (as seen in the image below) has a cartilaginous and bony component that is lined with mucoperichondrium and mucoperiosteum, from which the cartilage and bone receive their blood supply. Interruption of the opposition of perichondrium to cartilage (as with septal hematoma) may interrupt the blood supply and lead to resorption of septal cartilage and possibly subsequent saddle-nose deformity.

Contraindications
Some fractures do not need correction, providing the patient is satisfied with the appearance and function of the nose. In more severe injuries, one must entertain the option of deferring a nasal procedure until the patient has become stabilized.
-
Oblique view.
-
Lateral view.
-
Nasal septum.









