Practice Essentials
Patients with cleft deformity have cosmetic problems and impaired nasal airflow as a result of distorted anatomy. [1] These patients have septal deflections, atretic nostrils, turbinate hypertrophy, and cleft lips and palates. Nasal rhinometry has demonstrated statistically significant findings of smaller airways in patients with cleft deformity when compared with patients without cleft deformity. Warren et al showed that children with unilateral cleft deformity have smaller airways than children with bilateral cleft deformity. [2] However, these differences do not persist over time. Although the cleft nose grows as the patient ages, it remains 30% smaller than that of patients without cleft lip deformity.
Cleft lip nasal deformity offers a unique challenge to the reconstructive surgeon for many reasons. First, clinical presentation of cleft lip varies widely, requiring a host of surgical techniques. Second, deformity may be quite severely asymmetric, making surgical correction difficult. Third, patients with cleft lip may have been previously subjected to numerous surgical interventions, leading to significant scar tissue in the operative site. Fourth, timing of rhinoplasty, whether synchronous or staged with cleft lip repair, is controversial. Fifth, this nasal anomaly affects the pediatric population, and the patient's growth affects surgical results. Conversely, the surgery may adversely compromise nose growth.
This article is intended as an introduction to basic clinical features of the deformity, shown below, and to some surgical options for correction.
Surgery
Surgical management of cleft lip nasal deformity includes the following:
-
Nasal airway - Adult studies have corroborated that postsurgically corrected noses maintain significantly smaller airways than noncleft noses; hence, parallel goals of cosmetic and functional improvement must be served
-
Septal deformity - Surgical correction aims at establishing a patent nasal airway while creating a more favorable external nasal appearance
-
Columellar deformity - The columella is viewed as foreshortened in cleft lip nasal deformity; two views on the best surgical management exist, with some surgeons arguing that the columella requires primary correction and others maintaining that reshaping the nasal ala is sufficient to affect columellar length [3, 4]
-
Alar deformity - Surgical techniques may be categorized into external and internal approaches; in mild defects, the nostril may be repositioned by excising a wedge of skin anterior to the rim margin and advancing the rim forward
-
Dorsal deformity - Correction of septal deflection may be sufficient to reestablish normal dorsal symmetry
-
Bilateral cleft lip nasal deformity - The hallmark of bilateral cleft lip nose is a short columella, with surgical techniques focusing on achieving proper columellar length
History of the Procedure
Historically, cleft lip nasal deformity has received less attention than primary lip repair or has been ignored altogether. In pre-Columbian figurines, cleft lip was sculpted accurately, but nasal appearance was depicted incorrectly as normal. Rhinoplasty for cleft lip was not introduced until the turn of the 20th century. Most modern techniques had already been described by the 1920s-1940s, albeit with less refinement (eg, open rhinoplasty incisions were placed along the alar rim, leaving a conspicuous scar). It was not uncommon for patients to have undergone as many as 20 procedures for cleft lip/palate/nose. Currently, the literature offers numerous opinions regarding the best surgical approach and timing of intervention.
Etiology
Embryologic origin of cleft lip nasal deformity is not well understood. Curiously, classic nasal anomaly of patients with cleft lip may exist in absence of any cleft lip deformity owing to fetal derangements affecting only the nose. The nose is derived from two distinct tissue masses, the frontonasal and lateral facial complexes. Frontonasal processes that migrate over the forehead constitute the nasal placodes. In turn, nasal placodes develop into the medial and lateral processes, forming the columella and alae, respectively. Theory holds that mesodermal growth of the alae may follow growth of the central portion of the nose. Any disruption of this process may result in unilateral nasal deformity. Furthermore, incomplete union of the frontonasal and lateral facial complexes may contribute to clefting.
Presentation
Clinical presentation of cleft lip varies widely.
-
Deformity may be quite severely asymmetric.
-
Septal deflections, atretic nostrils, turbinate hypertrophy, and cleft lips and palates are presenting features.
-
Patients with cleft lip may have significant scar tissue from previous surgical interventions.
Indications
See Surgical therapy.
Relevant Anatomy
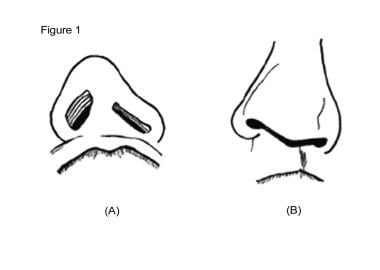
The major defect of cleft lip nasal deformity concerns the position of the ala. The ala lies inferior and lateral to the contralateral side; its relative position falsely lengthens the nose on that side. The ala rests on an underdeveloped premaxilla, which partly accounts for alar base lowering and horizontal nostril seating, as depicted in the image below. The ala is often underdeveloped and weak, exhibiting a convoluted shape. This contributes further to dome lowering on the cleft side. Because of the abnormal ala, the columella is foreshortened and lies obliquely, with its base directed away from the cleft side. Bone growth is retarded on the cleft side; nasal bones and the nasal process of the maxilla are underdeveloped, causing the nasal dorsum to tilt to the cleft side. The septum may lie outside of the maxillary crest seat, and the cartilaginous portion may be buckled, both of which may cause nasal tip deviation.
The nasal septum exhibits a wide range of abnormalities in addition to obvious external cosmetic deformities. When cleft palate coexists with cleft lip, significant bony abnormalities may occur along the nasal floor, including nasal-oral fistula. Bilateral cleft lips may also reveal a duplicated thickened septum, which is postulated to represent failed growth of 2 septa. Studies have confirmed the presence of significant septal deviation in patients with bilateral cleft lip when compared to patients without bilateral cleft lip. The septum tends to deviate toward the cleft side, with the cartilaginous base displaced off of the maxillary crest toward the cleft side. This septum malposition contributes to nasal tip tilt toward the noncleft side, as depicted in the image below.
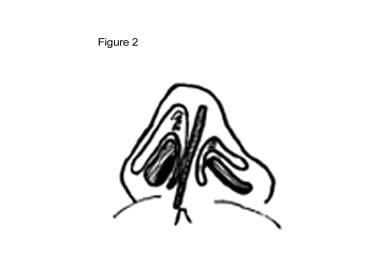 Cleft lip nasal deformity. Septum deviated toward cleft side and lying outside of maxillary crest.
Cleft lip nasal deformity. Septum deviated toward cleft side and lying outside of maxillary crest.
Contraindications
Surgical intervention for cleft lip nasal deformity may be contraindicated in certain conditions. No absolute age minimum exists for nasal reconstruction. However, nasal surgery should be elected after age 5 years to permit sufficient physical and psychological maturity to develop before surgery is undertaken. Major septal surgery may be performed later in combination with or independent of external nasal surgery to allow for maximal time for development in this important facial growth center. (However, a study by Seo et al suggested that in patients who, during infancy, undergo primary rhinoplasty to correct nasal deformity at the same time as bilateral cleft lip surgery is performed, nasal dimensions at skeletal maturity are not deficient compared with those of controls. [5] ) As alluded to, psychological maturity is a critical consideration so that realistic and mutual goals may be set by the surgeon and patient before rhinoplasty surgery is undertaken. Such discussion may be undertaken only once the patient is older and able to understand the ramifications of surgery.
-
Cleft lip nasal deformity. A: Basal view. B: Frontal view.
-
Cleft lip nasal deformity. Septum deviated toward cleft side and lying outside of maxillary crest.
-
Cleft lip nasal deformity. Ivy modification of the Blair procedure. Laterally based nostril rim flap rotated medially inward.
-
Cleft lip nasal deformity. Dingman technique. Nostril rotated via columellar and alar-based flap.
-
Cleft lip nasal deformity. V-Y advancement for columellar lengthening.
-
Cleft lip nasal deformity. Rectangular flap for columellar lengthening.
-
Cleft lip nasal deformity. Brauer-Foerster procedure for columellar lengthening via medial rotation of bilobed flaps.
-
Cleft lip nasal deformity. Cronin procedure for columellar lengthening. Anteriorly based bilobed flap is advanced anteriorly, and posteriorly based columellar flap is advanced posteriorly.
-
Cleft lip nasal deformity. Ferris-Smith procedure. Repair of total columellar loss; full-thickness skin graft (FTSG) is buried beneath upper lip skin and later rotated into place.
-
Cleft lip nasal deformity. Serre method. Repair of total columellar loss; doubled full-thickness skin graft (FTSG) is buried beneath upper lip skin and later rotated into place.
-
Cleft lip nasal deformity. Elevation of nostril apex by excision of skin wedge.
-
Cleft lip nasal deformity. Thomas Rees technique. Lateral crus of lower lateral cartilage is severed from lateral attachment and advanced medially to be sutured to contralateral ala.
-
Cleft lip nasal deformity. Tajima reverse-U technique. A: Intranasal incision. B: Suture ala on the cleft side to (1) ipsilateral upper lateral cartilage, (2) contralateral cartilage, and (3) contralateral ala.
-
Cleft lip nasal deformity. Cartilage grafts. A: Onlay alar graft. B and C: Turnover alar graft.
-
Cleft lip nasal deformity. Bilateral cleft lip nasal deformity. Broad, flat, bifid tip; wide alar bases; and short columella. A: Frontal view. B: Profile view.
-
Cleft lip nasal deformity. Millard classic forked flaps. One taken from each side of prolabium and banked within nasal sills during primary lip repair until secondary rhinoplasty.





