Background
Difficulty breathing through the nose after rhinoplasty is a serious problem. Patient dissatisfaction can be significant, even when cosmetic results are excellent. Long-term impacts on the quality of life and contributions to the pathophysiology of sleep-related breathing disorders have both been documented. This article focuses on the etiology, diagnosis, and treatment of postrhinoplasty nasal obstruction, with particular attention to the nasal valve area.
An image depicting internal nasal valve anatomy can be seen below.
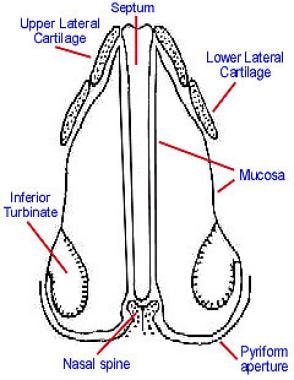 Rhinoplasty, postrhinoplasty nasal obstruction. Normal internal nasal valve anatomy. Notice the relationship between the septum, upper lateral cartilage, pyriform aperture, and inferior turbinate.
Rhinoplasty, postrhinoplasty nasal obstruction. Normal internal nasal valve anatomy. Notice the relationship between the septum, upper lateral cartilage, pyriform aperture, and inferior turbinate.
Problem
The etiology of postrhinoplasty nasal obstruction can be multifactorial but is primarily the result of the interplay between 2 factors. Unrecognized preexisting nasal conditions (eg, deviated nasal septum, turbinate hypertrophy, mucosal disease) in conjunction with the overresection of cartilages and a subsequent decrease in the nasal valve area after rhinoplasty are responsible for most cases of postrhinoplasty nasal obstruction.
Epidemiology
Frequency
Some investigators (ie, Courtiss and Goldwyn, Beekhuis) report that the prevalence of airway impairment after aesthetic rhinoplasty may be as high as 10%. [1, 2]
Etiology
The cause of postrhinoplasty nasal obstruction is often the interplay between a preexisting but unrecognized nasal abnormality and a reduction in nasal valve area secondary to the aesthetic rhinoplasty. [3]
During the evaluation and assessment of patients with postrhinoplasty breathing problems, Courtiss and Goldwyn and Beekhuis found that uncorrected septal pathology and overzealous resection of lower or upper lateral cartilage were significant causes of nasal airway obstruction after rhinoplasty. [1, 2] When preexisting pathologies (eg, nasal septal deviation, inferior turbinate hypertrophy, allergic rhinitis) are not recognized and addressed, a nasal valve area that is borderline-narrowed but asymptomatic preoperatively can become symptomatic postoperatively because of a further decrease in the nasal valve cross-sectional area.
Grymer used acoustic rhinometry to evaluate the internal dimensions of the nasal cavity in 37 patients before reduction rhinoplasty and again 6 months after surgery. [4] He demonstrated that rhinoplasty decreases the cross-sectional area of the nasal valve by 25% and the piriform aperture by 13%. Cole et al also used rhinomanometry to reveal that changes of as small as 1 mm to the nasal valve size can dramatically increase nasal resistance. [5]
Therefore, the nasal valve, as a regulator of nasal airflow and resistance, has been demonstrated to play a critical role in the function of the nose. Disturbance of the nasal valve area can produce limitations to normal nasal breathing. Multiple schemes can be used to classify the types of nasal valvular dysfunction. One convenient method is to group them according to either internal or external nasal obstruction (see Classification of nasal valve dysfunction).
Kern and Wang divide the etiologies of nasal valve dysfunction into mucocutaneous and skeletal/structural disorders. [6] The mucocutaneous component refers to the mucosal swelling (secondary to allergic, vasomotor, or infectious rhinitis) that can significantly decrease the cross-sectional area of the nasal valve and thus reduce nasal airway patency. The skeletal/structural component refers to any abnormalities in the structures that contribute to the nasal valve area. This includes the nasal septum, upper and lower lateral cartilage, fibroareolar lateral tissue, piriform aperture, head of the inferior turbinate, and floor of the nose.
The skeletal component can be further divided into static and dynamic nasal dysfunction. Static dysfunction is secondary to continuous obstruction at the level of the nasal valve due to deformities such as deviated septum, inferior turbinate hypertrophy, or inferomedially displaced upper lateral cartilage. Dynamic dysfunction is obstruction that varies in severity with respiratory effort and is usually related to deficiencies in the structural support of the lateral nasal wall, including the cartilaginous, fibroareolar, and muscular components. The lateral nasal wall caudal to the bony arch is mobile and responds variably to pressure changes.
The degree to which lateral wall movement occurs depends on the intrinsic stability of its skeletal and soft tissue support and on the pressure changes it is subjected to during quiet and forced inspiration. According to the Bernoulli principle, as the flow velocity of inspired or expired air increases, the pressure inside the nasal vault decreases relative to atmospheric pressure. At a threshold flow velocity, the disparity between pressures inside and outside the nasal vault overcomes the stability of the lateral nasal wall, and collapse occurs. This intrinsic stability derives from the rigidity of the unaltered nasal anatomy or from the support provided by the skeletal and soft tissue elements that remain after rhinoplasty.
Because ventilation involves pressure changes, the nasal airways must be stable both at rest and under the negative pressures created during quiet and forced inspiration. The internal and external nasal valves depend on satisfactory skeletal stability of the upper and lower lateral cartilages, respectively. When either the skeletal or the soft tissue component is congenitally deficient or has been compromised by surgery or trauma, the patient experiences a dynamic collapse of the valve during inspiration, with resultant airway obstruction. Normally, the upper lateral cartilages partially collapse at a ventilatory flow rate of 30 L/min. Thus, even normal nasal valves collapse with vigorous respiratory effort; however, a patient with dynamic nasal valve dysfunction may have a lateral nasal wall that is so weakened that it collapses even during normal nasal breathing.
In summary, nasal valve dysfunction can be secondary to either mucocutaneous problems or skeletal deformities (affecting either the internal or the external nasal valve), which can be dynamic or static. However, the cause is rarely so straightforward. In most instances, the mucocutaneous and skeletal components and the static and dynamic components contribute in varying degrees to the overall nasal valvular dysfunction.
Classification of Nasal Valve Dysfunction
Nasal valve dysfunction is classified below.
Mucocutaneous disease
See the list below:
-
Allergic rhinitis
-
Vasomotor rhinitis
-
Infectious rhinitis
-
Rhinitis medicamentosa
-
Sinusitis
Skeletal deformity
Deformities that affect the internal nasal valve area
-
Static deformity
Inferomedially displaced upper lateral cartilage
Narrowing of pyriform aperture
Scarring at intercartilaginous junction
Turbinate hypertrophy
Deviated nasal septum
-
Dynamic deformity - Collapsed upper lateral cartilage secondary to disruption of support from the nasal bone, septum, and lower lateral cartilage
Deformities that affect the external nasal valve
-
Static deformity
Tip ptosis
Cicatricial stenosis
-
Dynamic deformity
Collapsed lower lateral cartilage secondary to excessive excision
Nasal muscle deficiency
Pathophysiology
Internal nasal valve obstruction
Static dysfunction includes (1) inferomedial displacement of the upper lateral cartilage, (2) narrowing of the piriform aperture secondary to osteotomy, (3) scarring at the intercartilaginous junction, (4) turbinate hypertrophy, and (5) deviated nasal septum, described as follows:
-
Inferomedial displacement of the upper lateral cartilage
The middle nasal vault is composed of the paired upper lateral cartilages and the dorsal cartilaginous septum. Understanding that the upper lateral cartilages are joined to the dorsal septum as a single cartilaginous unit in the cephalic two thirds of the vault is important.
Sheen recognized that resection of the cartilaginous middle vault roof during hump removal disrupts this important connection between the upper lateral cartilage and the dorsal septum. [7] This allows the upper lateral cartilages, which now lack support medially, to fall toward the narrowed dorsal septal edge. This results in internal valve collapse and a characteristic inverted-V deformity. Thus, nasal valve dysfunction is common in patients after excessive and uncompensated narrowing of the middle nasal vault in rhinoplasty.
The amount of inferomedial displacement of the upper lateral cartilages also depends on whether the superior support with the nasal bone or its inferior connection with the lower lateral cartilage has been disrupted. Thus, if the caudal trim of the upper lateral cartilage or the cephalic trim of the lower lateral cartilage is aggressive, the scroll area weakens, which results in further medial displacement of the upper and lower lateral cartilages.
-
Narrowing of the piriform aperture secondary to osteotomy
Overly aggressive lateral osteotomies and infracturing can lead to medial displacement of the nasal bone with corresponding displacement of the upper lateral cartilage.
This dramatically narrows the nasal valve angle and decreases the valve cross-sectional area, contributing significantly to nasal airway obstruction after rhinoplasty.
-
Scarring at the intercartilaginous junction
A basic principle of surgery is that incisions placed across a concave surface risk scarring and distortion. The nasal valve is such a concave area and is frequently involved when an intercartilaginous incision is used.
Improper placement and poor closure of intercartilaginous incisions may lead to scar formation and contracture at the nasal valve angle. Surgeons who primarily use internal incisions in rhinoplasty may be more likely to injure the scroll while they make standard intercartilaginous incisions.
When intercartilaginous incisions are extended anteriorly and joined to columellar full-transfixion incisions, the risk of mucosal scarring and synechiae is increased, which may lead to blunting of the apex of the internal valve. This is especially likely to occur if the incisions are not sutured well and heal poorly.
-
Turbinate hypertrophy
The head of the inferior turbinate contributes to the internal nasal valve area. Thus, inferior turbinate hypertrophy of any cause decreases the cross-sectional area of the nasal valve.
While rhinoplasty itself does not cause this deformity, failure to recognize and to correct inferior turbinate hypertrophy contributes to the problem of postrhinoplasty nasal obstruction.
-
Deviated nasal septum: Similar to inferior turbinate hypertrophy, a nasal septum deviated at the nasal valve area contributes to postrhinoplasty nasal obstruction if not recognized and corrected during the rhinoplasty.
Dynamic dysfunction includes collapsed upper lateral cartilage secondary to disruption of support to the nasal bone, septum, and lower lateral cartilage.
-
Collapsed upper lateral cartilage secondary to disruption of support to the nasal bone, septum, and lower lateral cartilage
The upper lateral cartilage is connected to and derives support from the nasal bone cephalically, dorsal septum medially, and lower lateral cartilage caudally.
After resection of the cartilaginous middle vault roof during hump removal and disruption of the scroll area secondary to cephalic trimming of the lower lateral cartilages, the upper lateral cartilages are prone to medial collapse. This collapse is not only static in that it continuously narrows the nasal valve angle, but it is also dynamic.
With the static reduction of the nasal valve angle, greater inspiratory force is needed to generate enough airflow through the narrowed nasal passageway. This increased pressure differential across the nasal valve area can cause dynamic collapse of the unsupported and frail upper lateral cartilage and cause a vicious cycle of further narrowing of the nasal valve angle.
External nasal valve obstruction
External nasal valve collapse is due to collapse of the nostril margin at the opening of the nose (alar collapse) with moderate-to-deep inspiration through the nose. This phenomenon is usually observed in patients with narrow slitlike nostrils, a projecting nasal tip, and thin alar sidewalls.
The cause of external valve collapse may be surgical, congenital (eg, hypoplasia, paradoxical lateral crura), or posttraumatic in nature. This article focuses on only postrhinoplasty-related external valvular collapse. Constantian and Clardy reviewed 160 patients treated for external nasal valve incompetence. Surgical reconstruction was performed with septal cartilage or with composite conchal cartilage-skin grafts. Using rhinomanometry, Constantian and Clardy found that correction of external valvular incompetence increased total nasal airflow during quiet ventilation by more than 2-fold over preoperative values. Thus, the external nasal valve may play a crucial role as the cause of nasal airway obstruction in some patients.
Static dysfunction includes tip ptosis and cicatricial stenosis, described as follows:
-
Tip ptosis
The etiology of tip ptosis can be divided into either structural deficiencies in the cartilaginous or ligamentous support of the tip or excess soft tissue bulk that creates a mass effect at the tip.
Structural ptosis can result from rhinoplasty as a consequence of weakened support from the medial crura or columella. Furthermore, performing rhinoplasty through the delivery approach and dividing the cephalic margin of the lower lateral cartilage from the caudal margin of the upper lateral cartilage disrupts one of the major tip support mechanisms and may cause caudal slippage of the lateral crura, which results in structural ptosis.
Ptosis from soft tissue bulk is usually idiopathic in nature and is the consequence of thick redundant skin and subcutaneous tissue in the tip and supratip regions. Ptosis may also be the consequence of conditions such as rhinophyma.
-
Cicatricial stenosis
Cicatricial stenosis is a less common cause of significant external nasal valve dysfunction and may be secondary to iatrogenic injury from poorly placed marginal incisions or may be a result of an inhalation injury.
Scar tissue may narrow the valve area through the formation of hypertrophic webs; however, more often, wound contracture causes a cicatricial narrowing.
Sheen conservatively estimated that 75-85% of postrhinoplasty patients have some reduction of the nasal vestibule.
Dynamic dysfunction includes (1) flaccid collapse of the lower lateral cartilage after the overresection of cartilage during tip-modeling procedures and (2) nasal musculature deficiency, described as follows:
-
Flaccid collapse of lower lateral cartilage after overresection of cartilage during tip-modeling procedures
The cutaneous and skeletal supports of the lower lateral cartilages comprise the structural support of the external nasal valves.
Overzealous resection of the cephalic margin of the lower lateral cartilages can lead to flaccid collapse of the cartilaginous framework of the lateral nasal wall. Because of this lack of support, the pressure differential across the nasal valve during inspiration can cause the lateral nasal wall to collapse.
-
Nasal musculature deficiency
The nasal musculature normally acts to pull the lateral nasal wall outward to prevent medial collapse during inspiration.
The importance of functional nasal musculature can be inferred from the nasal obstruction that occurs in patients with facial nerve paralysis.
Nasal muscular deficiency can be secondary to aging or can be due to rhinoplasty surgical damage such as devascularization, partial denervation, or fibrosis.
Presentation
History
Begin with an accurate diagnosis before considering the array of medical and surgical treatments. Focus the history on the relationship between the onset of nasal obstruction and the rhinoplastic procedure. Determine the patient's preoperative nasal function in order to evaluate preexisting nasal deformities (eg, deviated nasal septum, turbinate hypertrophy, allergic rhinitis, vasomotor rhinitis, sinusitis). Record the duration, side (ie, unilateral, bilateral, alternating), timing (ie, continuous vs intermittent), severity, and any associated symptoms. Elicit a history regarding prior medical and surgical treatments for nasal obstruction and their effectiveness. An operative report from the previous surgeon who performed the rhinoplasty may be helpful.
Disease-specific quality of life instruments can be useful to systematically assess symptoms before and after treatment. The Nasal Obstruction Symptom Evaluation (NOSE) scale is a validated instrument assessing the following 5 categories:
-
Nasal congestion or stuffiness
-
Nasal blockage or obstruction
-
Trouble breathing through the nose
-
Trouble sleeping
-
Inability to get enough air through nose during exercise or exertion
Physical examination
The typical postsurgical nose with nasal airway obstruction is overresected, with a narrowed but scooped-out dorsum and a narrow pinched tip. These patients commonly have nasal obstruction due to incompetent nasal valves. When examining a patient who reports nasal obstruction, evaluate the internal and external valves and the septum and turbinates.
The standard Cottle maneuver, which is used to assess nasal valve incompetence by judging improvement in nasal breathing with lateral distraction of the ipsilateral cheek, is a test with nonspecific results. Even the narrow airway produced by anterior septal deviation or turbinate hypertrophy is improved by traction on the cheek. Anterior rhinoscopy is also a poor means of accurately evaluating subtle changes in nasal valve anatomy; the dysfunctional nasal valve is frequently missed because of distortion from the nasal speculum.
A more precise diagnosis can be made based on direct inspection of valvular support during quiet and forced inspiration, without the distortion induced by a nasal speculum. Collapse at the internal nasal valve is usually diagnosed based on the identification of medialization of the caudal margin of the upper lateral cartilages due to negative pressure created upon inspiration through the nose. These patients typically have pinching or medial collapse of the supraalar region.
External nasal valve collapse can be diagnosed based on observation of the nostril margin to determine if the alae collapse with moderate-to-deep nasal inspiration. Next, a modified Cottle maneuver can be performed with a cerumen curette placed intranasally to support the internal or external nasal valve to determine specifically if improvement in nasal airflow results. Minimal distraction of a collapsed internal valve or stabilization of the external valve during inspiration can dramatically increase airflow on the affected side and confirm the diagnosis.
The patient can usually appreciate an immediate improvement in airflow when a flaccid or collapsible valve is supported during inspiration.
Because symptoms are commonly inconsistent with appearances, objective criteria are required for an accurate diagnosis, appropriate therapy, and assessment of results. Objective measurement of nasal airway resistance can be obtained with the use of rhinomanometry.
More recently, Hilberg et al introduced acoustic rhinometry as a noninvasive and reliable objective method for determining the cross-sectional area of the nasal cavity. [8] Acoustic rhinomanometry is based on the analysis of sound waves reflected from the nasal cavities. It provides an estimate of the cross-sectional areas of the nose as a function of the distance from the nostril. Thus, the site (anterior, mid, or posterior) and degree of nasal obstruction can be identified. Also, analysis can be done before and after topical decongestants are applied, allowing discrimination of mucocutaneous versus structural blockage. Standards for age, race, ethnicity and sex have been recently published.
Lam et al demonstrated that validated anatomic, physiological, and subjective nasal measures, while internally consistent, may not correlate with one another, suggesting that various measures may assess different aspects of nasal airway obstruction and provide complementary information. [9]
Indications
The treatment of postrhinoplasty nasal obstruction has no absolute indications. The extent of medical and surgical treatment depends on the severity of symptoms and the patient's desire to improve his or her ability to breathe through the nose.
Relevant Anatomy
Mink first coined the term nasal valve in 1903 to refer to the slitlike opening between the caudal end of the upper lateral cartilage and the nasal septum. This angle is normally 10-15° in the leptorrhine nose (typical nose in whites) and is more obtuse in the platyrrhine nose (typical nose in African Americans). The nasal valve is only a portion of the internal nasal valve area, which is bounded superiorly by the nasal valve, medially by the septum, laterally by the caudal end of upper lateral cartilage and the bony piriform aperture and its adjacent fibrofatty tissue, inferiorly by the floor of the nose, and inferolaterally by the head of the inferior turbinate.
The internal nasal valve area is the narrowest portion of the nasal passage and thus functions as the primary regulator of airflow and resistance. The cross-sectional area of the nasal valve area is 55-83 mm2. As described by the Poiseuille law, airflow through the nose is proportional to the radius of the narrowest portion of the nasal passageway, raised to the fourth power. Thus, changes as small as 1 mm in the size of the nasal valve exponentially affect airflow and resistance through the nasal cavity.
The external nasal valve is also described and is formed by the lateral crura of the lower lateral cartilage and its investing soft tissue cover. Many authors do not differentiate between the internal and external nasal valves. Although internal and external valve problems coexist in many cases, the distinction between these 2 types of valvular deformities is worth making because an accurate diagnosis affects optimal treatment results.
Contraindications
Contraindications to surgical correction of postrhinoplasty nasal obstruction are based on the patient's comorbidities and ability to tolerate surgery. Coexisting medical conditions may put the patient at risk during anesthesia. Additionally, patients with unrealistic expectations should probably not undergo surgical correction. Finally, patient refusal is an obvious contraindication.
-
Rhinoplasty, postrhinoplasty nasal obstruction. Normal internal nasal valve anatomy. Notice the relationship between the septum, upper lateral cartilage, pyriform aperture, and inferior turbinate.





