Background
Premaxillary augmentation addresses the nasal base, upper lip, and nasolabial angle. Augmentation is typically achieved with implanted autogenous grafts, homografts, or alloplasts. However, rotational flaps have also been described in the literature. Insertion of an implant anterior to the nasal spine may address several aesthetic shortcomings. A premaxillary implant can increase tip projection, improve the nasolabial angle, and lengthen the upper lip. Implants may also be inserted over the central upper lip anterior to the maxilla to achieve maxillary augmentation in combination with the aforementioned changes to nasal appearance. Alternatively, when malocclusion exists, orthognathic work addresses the malocclusion while simultaneously correcting premaxillary retrusion.
This article reviews basic anatomy and aesthetic considerations of the nasal base/tip-lip complex, discusses the advantages and disadvantages of implants used for premaxillary augmentation, and offers surgical techniques to achieve the desired cosmetic result.
See the image below.
Problem
The premaxilla (also known as the incisive bone, intermaxillary bone, or Goethe bone) is the bony segment of the maxilla that lies between the lateral borders of the lateral maxillary incisors. It exists as a separate bone in the fetus and sometimes in the adult. If anatomic growth of this area is hindered by congenital anomalies (eg, cleft lip and palate, Binder syndrome), premaxillary retrusion is observed. The retruded maxillary segment is identified by a constellation of defects, including an acute nasolabial angle, nasal tip ptosis, and labial incompetence at rest. Part of this retrusion may be manifested by class III malocclusion, which orthognathic surgery should correct.
Pronounced ethnic differences of the premaxilla have been observed. The premaxilla is commonly in need of augmentation in the classic mesorrhine and platyrrhine noses. Of course, detailed anatomic evaluation of each patient helps identify the presence or absence of this finding.
Epidemiology
Frequency
A cadaver study by Cohn et al found that in 10 tip rhinoplasties, using the sublabial approach, premaxillary augmentation was indicated in three procedures (30%) to help improve an acute, retrodisplaced nasolabial angle. [1]
The Aesthetic Society reported that in 2021, rhinoplasty was the fourth most commonly performed aesthetic plastic surgery procedure in men. [2]
Pathophysiology
Besides congenital malformations and various individual differences that account for premaxillary retrusion, 2 types of noses exhibit a higher prevalence of this deformity: noses of aging individuals and noses of individuals of Asian or African descent.
As an individual ages, the nose undergoes several predictable changes, including nasal tip ptosis, maxillary bone resorption (with or without loss of maxillary dentition), and decrease in the vertical height of the upper lip vermilion. The overall appearance is an unpleasant acute nasolabial angle, loss of nasal projection, and lengthening of the upper lip. The first 2 unaesthetic features may be addressed by premaxillary augmentation. However, the lengthening of the upper lip may be exacerbated with a premaxillary implant. Flowers and Smith have described a method to correct this latter problem with a rotational flap (see Treatment). [3] Also, be particularly wary of inserting an alloplastic premaxillary implant into an edentulous patient who wears dentures because of eventual erosion into the implanted pocket.
The classic mesorrhine and platyrrhine noses are characterized by an acute nasolabial angle and underprojection of the nose, both of which may benefit from premaxillary augmentation. An analysis of the nasal/maxillary skeleton reveals these findings. The leptorrhine nose is characterized by a prominent anterior nasal spine and prognathic premaxilla. In contrast, the mesorrhine, or Asian, nose displays a more retruded premaxillary component and shorter nasal spine. The platyrrhine structure of the typical African nose exhibits retrusion of the premaxilla with an almost absent nasal spine. Premaxillary augmentation has served as a fundamental part of rhinoplasty in mesorrhine and platyrrhine noses. Of course, these generalizations may not apply to a specific patient; an exacting anatomic analysis is essential in every case.
Presentation
Facial analysis
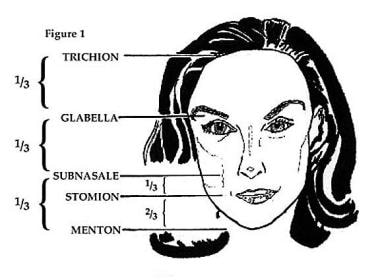
Ideally, the lower third of the face, from the subnasale to the menton, should occupy one third of the vertical dimension of the face. In aesthetic analysis, the remaining two thirds of the face may be equally divided from the trichion to the glabella and from the glabella to the subnasale. The lower third of the face may be further subdivided into an upper one third (subnasale to stomion) and lower two thirds (stomion to menton; see the image below). These ideal lengths should be kept in mind when performing premaxillary augmentation because the upper lip length is affected by this procedure.
When evaluating a patient for possible premaxillary augmentation, assessing the upper lip position both in repose and in animation, particularly smiling, is important. As premaxillary deficiency can lead to excessive and unaesthetic gum exposure (so-called gummy smile), the patient should be asked to smile to determine whether such a condition exists. If the patient has very little upper gingival showing or even partial overhang of the upper lip onto the incisors, the surgeon should be wary about pursuing premaxillary augmentation as dental show may be further lessened. This preoperative assessment and related patient counseling cannot be overemphasized.
Relevant Anatomy
Nasal base
A fundamental focus of aesthetic analysis of the nose is the nasal base. Often, terms used to describe this area are used imprecisely; for example, the term lobule may apply only to the tip of the nose or to the entire inferior portion of the nose, including the alae laterally. In this article, the term lobule refers specifically to the region of the nose medial to the alae and anterior to the nostrils, ie, the tip of the nose.
Vagueness in definition also affects the nasal base. Some authors define the nasal base as the area of the paired lower lateral cartilages, whereas others use the term to describe an area that is limited to the point at which the columella meets the upper lip (see the image below).
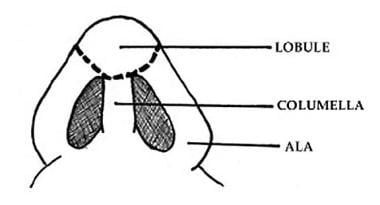 Premaxillary augmentation rhinoplasty. The nasal base: lobule, alae, and columella.
Premaxillary augmentation rhinoplasty. The nasal base: lobule, alae, and columella.
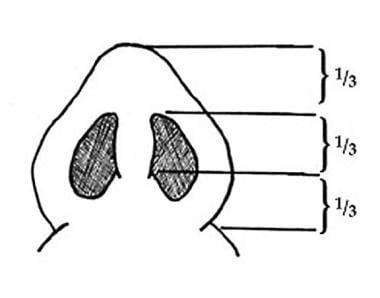
The nasal base is defined in this article as the entire triangular area from alar-facial crease to alar-facial crease and including the nasal tip. The anteroposterior dimension from nasal tip to base of the columella may be ideally subdivided into equal thirds: (1) from tip to anterior nostril rim, (2) from anterior nostril rim to anterior border of medial crural footplates, and (3) from anterior medial crural footplate to the base of the columella (see the image below). The width of the nasal base, from lateral alar margin to lateral alar margin, should equal the intercanthal distance and 70% of the length.
On lateral view, the nostril aperture should approximate an oval. The ideal width of the oval should be approximately 2-4 mm without excessive columellar/alar show or retraction. In addition, the columella should display a double break, with the break at the mid columella.
Nasolabial angle
The nasolabial angle, or, more precisely, the columellar-labial angle, is defined by the angle the columella makes with the upper lip. Ideally, the columellar-labial angle should be 95-115° for females and 90-100° for males. However, the individual face must be taken into account, and different facial configurations may benefit from a different columellar-labial angle. For example, a smaller or more acute columellar-labial angle is preferable in taller patients. However, a relatively more obtuse columellar-labial angle is aesthetically preferable in shorter patients. In general, the male nose may tolerate more variation in the columellar-labial angle than that of the female.
Contraindications
The lengthening of the upper lip produced by aging may be exacerbated with a premaxillary implant. Be particularly wary of inserting an alloplastic premaxillary implant into an edentulous patient who wears dentures because of eventual erosion into the implanted pocket.
As mentioned before, observation of the patient during forceful smiling is important in order to evaluate the safety of implant placement, as it concerns lengthening of the upper lip. For a patient with very little upper gum showing, a risk exists of pulling the lip so far down as to hood over the incisors. Another important consideration that concerns larger alloplastic implants involves the possibility for patients to feel the implant during smiling or animation, which can be quite troublesome. This possible outcome should be explained. Typically, smaller autogenous grafts do not cause this problem, but larger alloplasts can cause this problem. [4]
-
Premaxillary augmentation rhinoplasty. Ideal vertical dimensions of the face.
-
Premaxillary augmentation rhinoplasty. The nasal base: lobule, alae, and columella.
-
Premaxillary augmentation rhinoplasty. Ideal dimensions of the nasal base.
-
Premaxillary augmentation rhinoplasty. Ideal configurations of the alar-columellar relationship.
-
Premaxillary augmentation rhinoplasty. Rotational intracrural flap. Intracrural flap is pedicled posteriorly and bunched along the anterior maxillary spine.
-
Premaxillary augmentation rhinoplasty. Rotational subnasal flap. The de-epithelialized flap is tunneled anteriorly in a columellar soft pocket.
-
Premaxillary augmentation rhinoplasty. Example of a silicone premaxillary implant.





