Practice Essentials
Contact granulomas are benign lesions usually located on the posterior third of the vocal fold, which corresponds to the vocal process of the arytenoid cartilage. Contact granulomas may occur unilaterally or bilaterally.
Granulomas of the larynx can be classified into 2 general groups: specific granulomas and nonspecific granulomas. Specific granulomas are rare and include granulomas caused by tuberculosis [1] and syphilis. Nonspecific granulomas are benign and are unilaterally or bilaterally located on the vocal processes of the vocal folds. Histologically, they resemble pyogenic granulomas.
See the image below.
Contact ulcers (or granulomas) historically were thought to be the result of voice abuse or misuse, and the granulomas of intubation or gastroesophageal reflux were separate subsets of these conditions. However, for all purposes, the appearance, symptomatology, and treatment of these nonspecific granulomas are identical; therefore, both subsets of nonspecific granulomas can be considered a single entity.
Chevalier Jackson first identified contact ulcers in 1928. [2] He collected 127 case reports dating to 1888. In 1935, Jackson and Jackson suggested a mechanical cause related to the hammer and anvil effect of the vocal processes colliding against each other, leading to superficial mucosal ulceration (the contact ulcer) and focal granulation tissue response. [3]
Signs and symptoms of contact granulomas
Signs and symptoms of contact granulomas include the following:
-
Varying degrees of hoarseness and a low-pitched, pressed voice quality
-
Cough
-
Throat clearing
-
Pain, especially on pressed phonation or with cough or throat clearing
-
A rough foreign body sensation
Workup for patients with contact granulomas
Workup includes the following:
-
Double-pH probe (24 h) - This test is performed to determine whether reflux is the cause of or merely a contributing factor in the formation or propagation of the contact ulcer
-
Pharyngeal pH probe (24 h) [4] - This is a newer technology that allows direct measurement of pharyngeal pH
-
Flexible nasopharyngoscopy - The flexible scope allows evaluation of the dynamic activity of the larynx without the distortion of the supraglottic structures that occurs when the tongue is pulled anteriorly during a mirror and rigid telescopic examination
-
Videostrobolaryngoscopy
-
Objective voice measurements - Allows objective data regarding vocal pitch and perturbation parameters and may allow modification of therapy based on parameters in patients who are not responding to the current regimen
-
Electromyography - Useful to confirm vocal fold paresis as a predisposing factor in laryngeal hyperfunction
-
Speech therapy evaluation - Evaluation provides thorough assessment of the vocally abusive behaviors of the patient that contribute to the formation and propagation of the contact ulcer
If the lesion appears irregular or suspicious for carcinoma in any way, perform a diagnostic laryngoscopy with biopsy.
Management of contact granulomas
Medical treatment
The primary management of vocal process contact ulcers or granulomas is conservative and includes the following:
-
Cough prevention and treatment
-
Antireflux treatment
-
Lifestyle modifications
-
Speech therapy
-
Botulinum toxin type A [5]
-
Systemic steroid therapy (anecdotal) – Doses of steroids stronger than those considered therapeutic have been suggested for the treatment of contact granulomas
Surgical treatment
Surgical treatment is usually reserved for cases in which other approaches fail, cancer is suspected, the lesion is a fibroepithelial polyp, or the airway is compromised. The precise surgical approach for removal or biopsy of the granuloma is controversial.
Problem
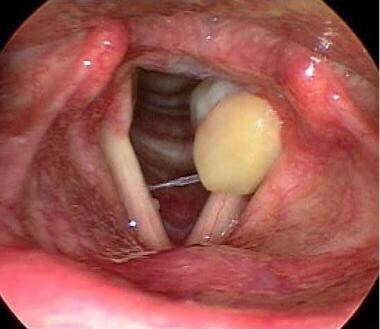
A contact granuloma is a pale or sometimes red mass located on the medial aspect of the vocal process of the arytenoid cartilage. Histologically, contact granulomas resemble pyogenic granulomas, which consist of chronic inflammatory infiltration with neovascularization and fibrosis covered by squamous epithelium.
Classic contact ulcers are thought to be the result of vocal misuse and abuse. With this etiology, the lesion most commonly is identified in men. These lesions often are similar in appearance to those found in patients after intubation (intubation granulomas) and in patients with gastroesophageal reflux.
Occasionally, a vocal process granuloma is identified in a patient for whom none of these factors are apparent. de Lima Pontes et al label this group idiopathic. The literature contains much confusion about this entity; however, for practical purposes, these lesions may be conceptualized as a group.
Etiology
Primary causes of contact granulomas may coexist in the same patient and include the following:
-
Intubation (see video below)
This patient was evaluated for hoarseness after prolonged intubation. The lesion resolved with observation and proton pump inhibitor therapy. Video courtesy of Vijay R Ramakrishnan, MD. -
Voice abuse
-
Laryngopharyngeal reflux disease
-
Idiopathic
Factors that contribute to the development of contact granulomas include smoking, allergy, infections, postnasal drip, and chronic throat clearing. Psychosocial traits associated with development of contact granulomas include aggressive personality, introversion, depression, emotional tension, and/or cancerophobia.
Certain dietary factors may affect the laryngeal milieu, leading to a detrimental mucosal environment. These factors include consumption of caffeine, chocolate, alcohol, peppermint, spicy foods, and tomato products; high-fat diet; poor water intake; and use of tobacco products. However, a direct causal relationship in the formation of contact ulcers has not been established.
Differential diagnoses include carcinoma, granular cell tumor of the larynx, and sarcoid.
Pathophysiology
Contact granulomas are usually pale, pedunculated masses found on the medial or superior edge of the vocal process of the arytenoid cartilage; however, they may also be deep red, lobulated, and sessile. These lesions may be 2-lipped structures that fit the vocal process of the opposite side.
Contact ulcers occur when the thin mucosa overlying the firm cartilage of the vocal process is crushed repetitively against the opposite side, causing a breakdown of the mucosa. An ulcer forms, accompanied by granulation tissue formation. An object such as an endotracheal tube may cause the injury leading to granulomas, or granulomas may result secondary to chronic irritation (eg, persistent gastroesophageal reflux injury).
A study by Li et al suggested that a finding of arytenoid cartilage sclerosis signals the presence of contact granuloma. High-resolution computed tomography (CT) scanning revealed that in patients with contact granuloma (41 with unilateral lesions and one with bilateral lesions), arytenoid cartilage sclerosis existed on 79.07% of the vocal folds with lesions, compared with 7.32% of those without lesions. The rate of arytenoid sclerosis associated with contact granuloma was also significantly greater than that for the lesion or nonlesion sides of vocal folds (13.11% or 2.56%, respectively) in patients with glottic laryngeal cancer or vocal cord leukoplakia without vocal process involvement. [6]
Presentation
Symptoms include the following:
-
Varying degrees of hoarseness and a low-pitched, pressed voice quality
-
Cough
-
Throat clearing
-
Pain, especially on pressed phonation or with cough or throat clearing
-
A rough foreign body sensation
The physician inquiry includes the following:
-
Intubation history, including nasogastric intubation
-
Reflux and associated high-risk habits (eg, dietary habits, caffeine intake)
-
Vocal use patterns (eg, glottal fry, hard glottal attack)
-
Pulmonary characteristics (eg, chronic cough, use of inhalers)
Indications
Even in relatively asymptomatic disease, treat the contact ulcer or vocal process granuloma to prevent growth and possible complications or sequelae of the inflammatory process, which include the following:
-
Airway obstruction
-
Bleeding (usually minor)
-
Vocal fold fixation
-
Posterior laryngeal stenosis
Surgical management of these lesions usually is frustrating because of a 37-50% recurrence rate. Surgical interventions are indicated for the following:
-
Fibroepithelial polyp
-
Airway compromise
-
Suspicion of carcinoma
Relevant Anatomy
Apices of the arytenoid cartilages are composed of elastic cartilage, and the rest of the arytenoid cartilage is hyaline cartilage. The arytenoid cartilages begin to ossify at approximately age 30 years. Ulcer or granuloma occurs on the vocal process of the arytenoid cartilage. The vocal process accounts for the posterior third of the vocal cord where the vocal ligament attaches.
The mucosa covering the vocal processes of the arytenoid cartilage is a thin layer of stratified squamous epithelium. This thin layer of mucosa is susceptible to being crushed between any unyielding object (eg, an endotracheal tube, the opposite arytenoid) and the firm cartilage beneath the mucosa.
Contraindications
Surgery is discouraged as the initial management for 2 reasons. Surgery is associated with a high recurrence rate of 37-50%, which often leads to multiple surgeries that may still be unsuccessful. Surgery may also cause the granuloma to migrate, following the wound edge.
-
Left vocal process granuloma on initial presentation (scope view of 70°).
-
Vocal process granuloma 2 months after initiation of antireflux therapy and speech therapy intervention in a patient who initially presented with left vocal process granuloma (scope view of 70°).
-
Vocal process granuloma 4 months after initiation of antireflux therapy and speech therapy intervention (scope view of 70°).
-
Flexible endoscopic view of contact ulcer in a patient upon presentation. The patient underwent surgical resection with recurrence prior to referral.
-
Resolution of contact granuloma 5 months after intensive antireflux therapy, speech therapy intervention, and botulinum toxin injection into left vocal fold (flexible endoscopic view). Note the small, red, residual spot.
-
24 hour pharyngeal pH probe study revealing moderate increase in acidity (decrease in pH) below 5.5 during the night.
-
This patient was evaluated for hoarseness after prolonged intubation. The lesion resolved with observation and proton pump inhibitor therapy. Video courtesy of Vijay R Ramakrishnan, MD.





