Practice Essentials
The differential diagnosis for cysts in the neck includes congenital neck masses, metastatic squamous cell carcinoma, acquired laryngoceles, and cystic schwannomas. Congenital masses in the neck include branchial cleft cysts, thyroglossal duct cysts (TGDCs), ectopic thymus cysts, dermoid and teratoid cysts, cystic vascular abnormalities, and lymphatic malformations such as the cystic lymphangioma. [1, 2] This article mainly focuses on the common entities branchial cleft cysts and TGDCs; to a lesser degree, it discusses lymphatic malformations. [3, 4]
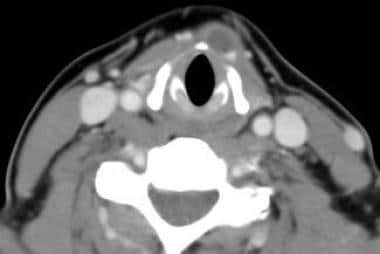
See the image below.
See 10 Patients with Neck Masses: Identifying Malignant versus Benign, a Critical Images slideshow, to help identify several types of masses.
Workup of neck cysts
To avoid complications, consider several studies in the preoperative evaluation of a thyroglossal duct cyst (TGDC). Confirmation of a normally functioning thyroid gland is important; therefore, always palpate the thyroid gland during the physical examination. If the gland is not palpated, ultrasonography or computed tomography (CT) scanning may be valuable.
Although not always the case, the patient with an ectopic thyroid often is hypothyroid and consequently has elevated thyroid-stimulating hormone (TSH). If hypothyroidism is suggested by the history, then a TSH test may be useful; however, an ectopic thyroid gland cannot be ruled out even in the presence of reference range TSH levels and a clinically euthyroid history. For this reason, ultrasonography, CT scanning, thyroid scanning, or magnetic resonance imaging (MRI) may be warranted to document a normal thyroid gland.
If the mass is infected, a fine-needle aspiration can be performed to obtain a culture to direct antibiotic therapy; however, if too much fluid is aspirated, future dissection may be more difficult.
Management of neck cysts
If the cyst is infected, treatment with an antibiotic is indicated before planning surgical excision. Complete resolution of inflammation allows for an easier and safer dissection.
Complete surgical excision is the goal when treating branchial cleft anomalies and TGDCs. Unless dangerous compromise of the aerodigestive tract is present, avoid incision and drainage procedures; these often obscure planes and make future complete surgical excision more difficult.
Surgical excision is an excellent option for lymphatic malformations that can be removed without sacrificing important adjacent structures. Infrahyoid lymphatic malformations without mediastinal involvement have been shown to have the most favorable outcome with surgical excision.
Problem
Most neck masses in children are benign inflammatory lesions, which can be successfully treated medically with antibiotics. Most neck masses in children that require surgery for diagnostic and therapeutic purposes are congenital in origin. Thyroglossal duct cysts (TGDCs) and branchial cleft cysts are the 2 most common congenital lesions.
Baer first described the branchial apparatus in 1827. The branchial arches begin to develop during the second week of gestation. During the fourth week of fetal development, 5 ridges, known as branchial arches, form on the ventrolateral surface of the embryonic head. Each arch contains mesoderm from which cartilage, muscle, and bone develop. Each arch is separated from the other arches by an external cleft of ectodermal origin. Each arch also has an internal pouch of endodermal origin and an associated cranial nerve, artery, and cartilage.
The anatomic location of a branchial cleft abnormality represents the presumed branchial cleft of origin. Branchial cleft anomalies can manifest in several different forms, including the following:
-
Fistula - Epithelial-lined tract with both an internal and an external opening
-
Sinus - Incomplete fistula with either an internal or an external opening
-
Cyst - Epithelial-lined cavity with neither an internal nor an external opening
Epidemiology
Frequency
More than 90% of branchial cleft anomalies arise from the second branchial cleft system. Approximately 8% of branchial cleft anomalies arise from the first branchial cleft system. Cysts arising from the third and fourth branchial cleft system rarely occur.
Branchial cleft anomalies and thyroglossal duct cysts (TGDCs) occur with equal frequency in males and females. Branchial cysts are twice as common as either branchial sinuses or fistulas. TGDCs are the most common mass found in the midline of the neck in children.
Etiology
Branchial cleft anomalies
Several theories are proposed to explain the genesis of branchial cleft anomalies. Incomplete closure of branchial clefts and pouches with failure of obliteration of the cervical sinus of His is suggested as a possible mechanism. Incomplete closure of branchial clefts and pouches with rupture of the branchial plate is another possible mechanism.
Thyroid gland anomalies
The thyroid gland forms as a diverticulum from the floor of the pharynx (tuberculum impar) at a site that later becomes the foramen cecum of the base of the tongue. The thyroid gland then forms 2 lobes and descends along a hollow canal called the thyroglossal duct in the midline of the neck. During the descent, the thyroglossal duct passes in close proximity to the developing hyoid bone. The thyroglossal duct normally involutes; however, when involution does not occur, the potential for development of a thyroglossal duct cyst (TGDC) increases. Arrest in the normal descent of the gland results in ectopic thyroid tissue.
The recognition of a cyst in the neck may not occur until decades later, commonly in association with a minor upper respiratory infection. This suggests that the potential for a cyst had existed for years. Many patients with a TGDC have some thyroid tissue in the cyst; therefore, thyroglossal duct anomalies might be a better term for their condition.
A study by Park et al indicated that adult patients, particularly men, who undergo radioactive iodine therapy may be more prone to TGDCs. However, the treatment did not seem to significantly affect the location, size, and shape of the cysts. [5]
Lymphatic malformations
Lymphatic malformations, which include lymphangioma and cystic hygroma, are areas of localized abnormal development of the lymphatic system. These malformations most commonly occur in the head and neck area. Although the exact embryonic origin of lymphatic malformations is unknown, several etiologies have been proposed. Possible causes include failure of the venous and lymphatic systems to connect, abnormal sequestration of the lymphatic tissue during embryogenesis, and abnormal budding of lymphatic structures from the cardinal vein. Other likely etiologies that focus on an acquired process include infection, trauma, and lymphatic obstruction.
Pathophysiology
Branchial system anomalies can manifest as a sinus, fistula, or cyst. Branchial cleft sinuses with external openings are usually associated with the first and second branchial cleft arches. Branchial cleft sinuses with internal openings are usually associated with the third and fourth arches.
First branchial cleft anomalies are subdivided into 2 types based on anatomic location. In type 1 first branchial cleft anomaly, the cyst or sinus opening can be located medial, inferior, or posterior to the conchal cartilage and pinna. A sinus tract, when present, parallels the external auditory meatus. In a type 2 first branchial cleft anomaly, the cyst and sinus tract are located in the anterior neck, always superior to the hyoid bone. A sinus tract or fistula, when present, travels over the angle of the mandible and through the parotid gland to terminate around the bony-cartilaginous junction in the external auditory meatus. The relationship to the facial nerve and parotid gland is variable with first branchial cleft cysts.
Second cleft anomalies are the most common of the branchial system. When an external opening is present in a second branchial cleft anomaly, the opening is located along the anterior border of the sternocleidomastoid muscle near the junction of the lower- and middle-third portions of the muscle, below the level of the hyoid bone. An internal opening, when present, is located in the tonsillar fossa. When present, a fistula ascends from the lower neck along the carotid sheath and crosses over the hypoglossal nerve and glossopharyngeal nerve. The fistula then passes between the internal and external carotid arteries to end in the tonsillar fossa. Second branchial cleft cysts are more common than sinuses or fistulas. The location of the cyst can be anywhere along the course of the fistula but most commonly is in the anterior triangle of the neck below the level of the hyoid bone.
Third branchial cleft anomalies are rare. When present, the external opening is located in the same location as a second branchial cleft anomaly; that is, along the anterior border of the sternocleidomastoid muscle at the junction of the middle and lower third portions of the muscle. The internal opening is located in the pyriform sinus rather than in the tonsillar fossa. The fistula tract ascends along the carotid sheath posterior to the internal carotid artery, then between the hypoglossal and glossopharyngeal nerves. The fistula tract then pierces through the thyrohyoid membrane and opens into the pyriform sinus. Cysts can occur at any location along this course but are usually found in the anteroinferior cervical triangle on the left side.
In 1972, Sanborn reported the first case of a fourth branchial arch anomaly. [6] If a fourth branchial arch anomaly occurs, it may have (1) an internal opening located near the apex of the pyriform sinus, (2) a fistula or sinus tract that travels between the superior and inferior laryngeal nerves, or (3) an external opening along the anterior border of the sternocleidomastoid muscle in the lower neck. The literature contains more than 30 cases of reputed fourth branchial cleft anomalies. Most are on the left side, with only 5 occurring on the right side.
Presentation
Branchial cleft anomalies
Branchial cleft cysts manifest in a different manner than branchial sinuses and branchial fistulae. The typical branchial cleft cyst, in the absence of infection, manifests as a nontender, smooth, round mass located along the anterior border of, or just deep to, the sternocleidomastoid muscle. Depending on the arch of derivation, the location can be anywhere from the external auditory canal to the clavicle. Branchial cleft cysts usually enlarge gradually and often are not detectable until the second or third decade of life.
Branchial cleft cysts that manifest in early childhood usually occur with an acute and painful enlargement of the cysts secondary to an upper respiratory infection. Branchial cleft cysts commonly increase in size in the presence of an upper respiratory tract infection and then decrease in size as the infection resolves.
An infected branchial cleft cyst can progress into an abscess or rupture spontaneously to form a draining sinus tract. Neonatal patients and patients with larger cysts can present with aerodigestive tract compromise and associated symptoms of stridor, dyspnea, and dysphagia. Second and third branchial cleft cysts can cause stridor with life-threatening airway obstruction in neonates.
In contrast to those patients with branchial cleft cysts, patients with branchial cleft sinuses and fistulas often present soon after birth because the external opening is visible on the skin. Branchial cleft fistulas and sinuses may also be palpable as a fibrous cord extending along the anterior border of the sternocleidomastoid muscle. Mucus drainage may occur from the external opening. Secondary infections from cutaneous organisms, most commonly Staphylococcus aureus and group A beta-hemolytic streptococci, cause purulent drainage and erythema and edema.
An infected first branchial cleft sinus or fistula may cause aural drainage in the absence of otitis media or otitis externa. A child presenting with both a draining ear and a tender mass in the neck may rarely have a first branchial cleft cyst associated with a sinus or fistula tract. A child presenting with a mass in the neck and a draining tract along the anterior border of the sternocleidomastoid muscle may have a second or third branchial cleft anomaly. A child with paratracheal swelling associated with tenderness and fever may have acute suppurative thyroiditis. Multiple authors have documented the spread of bacteria from an internal opening in the pyriform sinus in third branchial cleft anomalies.
Thyroglossal duct cysts
A thyroglossal duct cyst (TGDC) is the most common mass found in the midline of the neck. The mass is usually located at or below the level of the hyoid bone, although a TGDC can be located anywhere from the foramen cecum to the level of the thyroid gland.
Most patients with a TGDC present with asymptomatic masses in the midline of the neck. The literature reports that most of these lesions occur in patients younger than 30 years, although according to a study by Thompson et al of 685 TGDCs, the incidence of these lesions peaks in the first and fifth decades of life. [7] Interestingly, over the last decade, a number of older patients are presenting with a TGDC, some of whom are aged 80-90 years. Recurrent inflammation associated with infection of a TGDC is not uncommon. When infection is present, the cyst often enlarges and an abscess may form. Spontaneous rupture with secondary sinus tract formation can also occur.
The study by Thompson et al found a skin fistula associated with about 10% of TGDCs, with the fistula occurring twice as often in pediatric patients as in adults. [7]
Lymphatic malformations
Approximately half of all lymphatic malformations are diagnosed at birth, and 90% are diagnosed by age 2 years. With today's use of prenatal ultrasonography, diagnosing lymphatic malformations before birth is not uncommon. Most of these neck cysts present as slow-growing cystic cervical masses. When the mass is located in the suprahyoid location, the patient can present with respiratory compromise. Infection and hemorrhage of the malformation can cause sudden enlargement with respiratory compromise.
Indications
Treat branchial cleft anomalies, thyroglossal duct cysts (TGDCs), and lymphatic malformations for several reasons, including the following:
-
Removing the lesion provides a pathological diagnosis.
-
When infected, branchial cleft anomalies and TGDCs can cause acute pain and aerodigestive tract compromise.
-
Branchial cleft anomalies and TGDCs can cause cosmetic deformity.
-
Malignancy may occur (rare).
Relevant Anatomy
First branchial cleft fistulas and sinuses have a variable relationship to the facial nerve. No reliable methods are currently available to determine definitively the relationship between the sinus tract or fistula and the facial nerve prior to surgery. Surgeons, therefore, must be prepared for dissection of the facial nerve prior to embarking upon surgery for a first branchial cleft anomaly. A facial nerve monitor may be helpful.
Contraindications
Acute infection is a relative contraindication for surgical excision. Acute infection makes dissection more difficult and increases the risk of injury to surrounding structures. If possible, treat acute infection with appropriate IV antibiotics. If the infection is unresponsive secondary to abscess formation, incision and drainage or repeated aspiration in conjunction with antibiotic treatment may be required.
-
Axial CT scan of a patient with a relatively small thyroglossal duct cyst.
-
Axial CT scan of a first branchial cleft cyst.
-
Axial CT scan of a second branchial cleft cyst.
-
Axial CT scan of a third branchial cleft cyst.
-
Preoperative photograph of a 20-year-old female who underwent a simple excision of a thyroglossal duct cyst 12 years ago in Europe. The patient has had multiple infections over the past 10 years. The patient was actively infected at the time of this photograph, as seen by the skin erythema and swelling.
-
CT scan showing an infected recurrent thyroglossal cyst 12 years after simple excision.
-
Surgical specimen from the patient in Image 5 with prior simple excision of a thyroglossal duct cyst. Fistula tract with surrounding skin, cyst, midportion of the hyoid bone (which was not removed on prior surgery), and cuff of the base of the tongue muscle were excised.
-
Preoperative photograph of a man with a recurrent infected thyroglossal duct cyst.
-
Axial CT scan of the man in Image 8 with an infected thyroglossal duct cyst.
-
Intraoperative picture of the patient in Image 8 undergoing a Sistrunk procedure. The central portion of the hyoid bone is being resected along with the cyst, overlying skin, and cuff of the base of the tongue muscle.
-
Postoperative picture of the patient in Image 8 after a successful Sistrunk procedure.
-
CT scan of a man with a large neck lymphangioma.
-
Intraoperative picture of the resection of a large cystic lymphangioma.
-
Resection specimen of a well-circumscribed lymphangioma that was able to be removed in its entirety without sacrificing any surrounding structures.
-
Second branchial cleft fistula.
-
First branchial cleft cyst.
-
Thyroglossal duct cyst.
-
Picture of a 5-year-old-boy one year after having a Sistrunk procedure to remove a thyroglossal duct cyst.





