Practice Essentials
Fractures of the alveolar process of the mandible are uncommon. Unfortunately, their treatment is often fraught with problems, and uninitiated surgeons tend to underestimate these types of fractures and their challenges.
Signs and symptoms of mandibular alveolar fractures
The usual presenting reports with any fracture of the mandible as a result of trauma are localized tenderness, swelling, and malocclusion.
Workup in mandibular alveolar fractures
Computed tomography (CT) scanning has become the criterion standard for evaluating the mandible for fractures. In patients with multiple traumas, many emergency departments obtain near whole-body CT scans so that the needed information is available.
The panoramic dental radiograph was long the criterion standard for evaluating the mandible and is still an excellent alternative to and/or adjunct to CT scanning. It does offer the advantage of better evaluation of the teeth for injuries.
When the needed equipment is not available or the patient cannot be placed in the apparatus, plain radiographs of the mandible may be sufficient.
Periapical dental radiographs are often helpful in providing precise information about the status of teeth within a fractured segment of the alveolar process.
Management of mandibular alveolar fractures
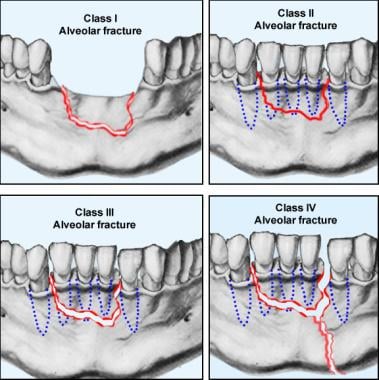
Reduction and immobilization of the fracture is mandated for alveolar process fractures. [1] The specific approach depends on the specifics of the injury. Previously, no classification of these fractures was available to guide decision making. The authors offer the following classification:
-
Class I fracture of the alveolar process - This involves a fracture of the edentulous segment
-
Class II fracture of the alveolar process - The fracture involves dentulous segment with little, if any, displacement
-
Class III fracture of the alveolar process - The fracture involves dentulous segment with moderate to severe displacement
-
Class IV fracture of the alveolar process - The alveolar process fracture shares one or more fracture lines with other fractures of the tooth-bearing facial skeleton
Class II fractures that need reduction may require a great deal of force to move into anatomic position. Class III fractures, however, typically offer the most challenges, likely because the encompassing portion of the mandible is intact, and to reduce the displaced segment of the alveolar process one must overcome the resistance produced by the interaction of the small irregularities of the bony surfaces. Class IV fractures are usually less challenging than class III fractures.
History of the Procedure
Mandible fractures are described in early Egyptian writings. Hippocrates advocated the use of bandages and interdental wiring for the treatment of mandibular fractures. In a 3-part article published during the Civil War, Gunning wrote of using dental splints attached to elaborate external appliances. In 1881, Gilmer first described the use of bars on both arches, fixed to the teeth and each other with fine wire ligatures.
Schede is credited for the first mandibular bone plating. He is said to have used a steel plate screwed to the mandible in the late 1880s. In 1934, Vorschutz described external fixation using transdermal bone screws and plaster. The Morris biphase is a refinement of that technique.
The history of rigid internal fixation devices is ongoing; a new theory and a corresponding set of devices appear every few years.
Clark's classes of alveolar fractures are depicted below.
Problem
Simply stated, the approach to treating these injuries is to do what is necessary to reduce them and then do what is necessary to hold them in reduction until they are healed. [2] The treatment options are somewhat limited by the lack of room for drill holes and associated hardware when the fracture involves a dentulous segment. Even with an edentulous segment, hardware is rarely practical because it usually ends up under a dental prosthesis and cannot be tolerated.
Epidemiology
Frequency
As pertains to the prevalence of facial fractures in the United States, the mandible is second only to the nose. Fractures of the alveolus account for only 1-5% of all mandibular fractures, making the alveolus one of the least commonly fractured regions.
The major difference in mandible fractures in countries other than the United States is in the etiology of these fractures. Some locations have less vehicular trauma because of a relative lack of vehicular transportation. Interpersonal facial trauma tends to have lower energy than vehicular trauma and, therefore, generally results in less severe injuries. Most countries other than the United States have fewer incidents concerning civilian firearms and a correspondingly lower frequency of penetrating trauma.
A study by Bicsák et al of isolated mandibular fractures seen at a German trauma center found that out of 541 fracture sites (328 patients), 40 (7.4%) occurred in the dentoalveolar region (ie, alveolar process fractures, dental injuries). [3]
Etiology
Alveolar process fractures are the result of blunt or penetrating trauma. The 2 most common etiologies of such blunt trauma in adults are fist fights and motor vehicle accidents. Other sources of facial trauma include athletic injuries, falls, and industrial accidents. [4]
Penetrating trauma to the mandible is most commonly in the form of a gunshot wound.
A retrospective study by Marotti et al found that in patients with isolated alveolar process fracture with associated trauma to the permanent teeth, pulp necrosis was the most frequent tooth complication, being found in over 40% of the traumatized teeth. The investigators reported that mature root development and concomitant injury were significant risk factors for pulp necrosis. [5]
A study by Lauridsen et al reported that for teeth with mature root development that have been involved in an alveolar process fracture, risk factors for pulp necrosis include fracture in relation to the apex, a greater than 2 mm displacement in the horizontal portion of the fracture, incomplete repositioning, and patient age above 30 years. [6]
Pathophysiology
For blunt trauma to produce an isolated fracture of the alveolar process, the blow must be concentrated on a segment of the alveolar process; however, this is an uncommon event. Alveolar process fractures that share fracture lines with other mandibular fractures are more common, usually representing a comminution of a body of mandible fractures.
A study by McCarty et al, using the National Trauma Data Bank, indicated that the prevalence of traumatic brain injury (TBI) in patients with an isolated facial fracture varies according to the fracture’s location. In patients with an alveolar process or palate fracture, the prevalence of mild traumatic TBI was found to be 46.0%. [7]
Presentation
The usual presenting reports with any fracture of the mandible as a result of trauma are localized tenderness, swelling, and malocclusion.
Indications
The presence of an alveolar fracture is the indication for treatment. The mode of treatment varies among patients.
Relevant Anatomy
A dental alveolus is a tooth socket. The alveolar process of the mandible is defined as the portion of the mandible surrounding and supporting the teeth. After loss of teeth, the associated alveolar process undergoes atrophy. Cortical bone covers the exposed surface of the alveolar process and the underlying cancellous bone; tooth sockets and teeth fill the remainder of the process. Tooth sockets are lined with thin, compact bone that is penetrated by blood vessels, lymphatics, and nerves. This alveolar bone contains the embedded ends of the connective-tissue fibers of the periodontal membrane (ie, Sharpey fibers).
Contraindications
Few contraindications exist to treating alveolar fractures. A nondisplaced class I fracture requires only observation. With other alveolar fractures, the patient's general condition may prohibit definitive treatment; examples include a chronic medical condition or results of trauma sustained when the mandibular fracture occurred. Head trauma resulting in an altered state of consciousness is the most common contraindication encountered in patients with alveolar fractures. Suspected or proven cervical spine injuries are also common contraindications. Most of these contraindications resolve with time and treatment. Hopefully, the alveolar process fracture can still be treated once the patient's general condition permits.
-
The various classes of alveolar fractures (per Clark).
-
An acid-etch wire composite splint can be used to stabilize an alveolar segment in selected patients. Support from a dentist is essential when using this technique. A heavy stainless steel wire is attached to the crowns of the teeth using a dental composite restorative material that requires acid etching of the enamel for adherence.
-
A lingual splint wired to the mandibular teeth and, perhaps, to the mandible is an excellent tool for stabilizing an alveolar segment. Dental laboratory facilities are required to fabricate such a splint.









