Practice Essentials
Viral hemorrhagic fevers (VHFs) are a group of febrile illnesses caused by RNA viruses from several viral families. These highly infectious viruses lead to a potentially lethal disease syndrome characterized by fever, malaise, vomiting, mucosal and gastrointestinal (GI) bleeding, edema, and hypotension. The image below depicts palatal petechiae and hemorrhage in a patient with Ebola virus disease (EVD).
 Filovirus disease - Ebola fever. Patient with Ebola hemorrhagic fever during 1976 outbreak in Zaire demonstrating palatal petechiae and hemorrhage. Photo courtesy of Joel Breman.
Filovirus disease - Ebola fever. Patient with Ebola hemorrhagic fever during 1976 outbreak in Zaire demonstrating palatal petechiae and hemorrhage. Photo courtesy of Joel Breman.
Four viral families are known to cause VHFs in humans: Arenaviridae, Bunyaviridae, Filoviridae, and Flaviviridae. General characteristics of these viral families can be found in the table below.
Table. Viral Families Causing Viral Hemorrhagic Fever (Open Table in a new window)
Virus Family |
Disease (Virus) |
Natural Distribution |
Usual Source of Human Infection |
Incubation (Days) |
Arenaviridae |
|
|
|
|
Arenavirus |
Lassa fever |
Africa |
Rodent |
5-16 |
|
Argentine HF (Junin) |
South America |
Rodent |
7-14 |
|
Bolivian HF (Machupo) |
South America |
Rodent |
9-15 |
|
Brazilian HF (Sabia) |
South America |
Rodent |
7-14 |
|
Venezuelan HF (Guanarito) |
South America |
Rodent |
7-14 |
Bunyaviridae |
|
|
|
|
Phlebovirus |
Rift Valley fever |
Africa |
Mosquito |
2-5 |
Nairovirus |
Crimean-Congo HF |
Europe, Asia, Africa |
Tick |
3-12 |
Hantavirus |
Hemorrhagic fever with renal syndrome, Hantavirus pulmonary syndrome |
Asia, Europe, worldwide |
Rodent |
9-35 |
Filoviridae |
|
|
|
|
Filovirus |
Marburg and Ebola |
Africa |
Fruit bat |
2-216 |
Flaviviridae |
|
|
|
|
Flavivirus |
Yellow fever |
Tropical Africa, South America |
Mosquito |
3-6 |
|
Dengue HF |
Asia, Americas, Africa |
Mosquito |
Unknown for dengue HF, 5-7 for dengue |
See Ebola: Care, Recommendations, and Protecting Practitioners, a Critical Images slideshow, to review treatment, recommendations, and safeguards for healthcare personnel.
Also, see the 11 Travel Diseases to Consider Before and After the Trip slideshow to help identify and manage infectious travel diseases.
For patient education resources, see the First Aid and Injuries Center, as well as Biological Warfare and Personal Protective Equipment.
Pathophysiology
The primary defect in patients with viral hemorrhagic fever (VHF) is that of increased vascular permeability. Hemorrhagic fever viruses have an affinity for the vascular system, leading initially to signs such as flushing, conjunctival injection, and petechial hemorrhages, usually associated with fever and myalgias. Later, frank mucous membrane hemorrhage may occur, with accompanying hypotension, shock, and circulatory collapse. The relative severity of the clinical presentation may vary depending on the virus in question, amount, and route of exposure.
In acute disease, patients are extremely viremic, and messenger ribonucleic acid (mRNA) evidence of multiple cytokine activation exists. In vitro studies reveal these cytokines lead to shock and increased vascular permeability, the basic pathophysiologic processes most often seen in viral hemorrhagic fever infection.
Another prominent pathologic feature is pronounced macrophage involvement. Inadequate or delayed immune response to these novel viral antigens may lead to rapid development of overwhelming viremia. Extensive infection and necrosis of affected organs also are described.
Hemorrhagic complications are multifactorial and are related to hepatic damage, consumptive coagulopathy, and primary marrow injury to megakaryocytes.
Multisystem organ failure affecting the hematopoietic, neurologic, and pulmonary systems often accompanies the vascular involvement. Hepatic involvement varies with the infecting organism and is at times seen with Ebola, Marburg, RVF, Crimean-Congo hemorrhagic fever (CCHF), and yellow fever. Acute kidney injury with oliguria is a prominent feature of hemorrhagic fever with renal syndrome (HFRS) seen in Hantavirus infection and may be seen in other VHFs as intravascular volume depletion becomes more pronounced. Bleeding complications are particularly prominent with Ebola, Marburg, CCHF, and the South American arenaviruses.
Although the pathophysiology of dengue infection is complex and incompletely understood, severe dengue infection can be differentiated from milder forms by the presence of increased vascular permeability. The greatest risk factor for severe dengue infection is secondary infection with a dengue serotype different from the initial dengue infection. This increased vascular permeability is thought to be secondary to widespread T-cell activation and apoptosis and is also thought to be related to a process known as antibody-dependent enhancement, best described as the balance between neutralizing versus enhancing antibodies after an initial dengue infection, which can contribute to the severity of secondary dengue infection.
Etiology
Arenaviridae
Arenaviridae are spread to humans by rodent contact and include Lassa virus in Africa and several rare South American hemorrhagic fevers such as Machupo, Junin, Guanarito, and Sabia. Lassa virus is the most clinically significant of the Arenaviridae, accounting for serious morbidity and mortality in West Africa.
Lassa fever first appeared in Lassa, Nigeria, in 1969. It has been found in all countries of West Africa and is a significant public health problem in endemic areas. In populations studied, Lassa fever accounts for 5-14% of hospitalized febrile illnesses. Its natural reservoir is a small rodent whose virus-containing excreta is the source of transmission. (See the image below.)
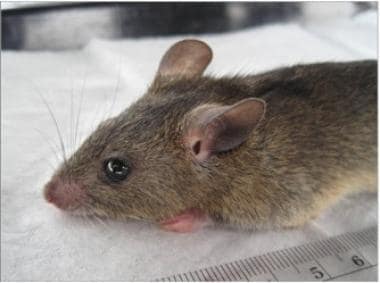 Mastomys natalensis, natural host of Lassa virus. Photo courtesy of BioMed Central, originally published in Kelly JD, Barrie MB, Ross RA, Temple BA, Moses LM, Bausch DG. Housing equityfor health equity: a rights-based approach to the control of Lassa fever inpost-war Sierra Leone. BMC Int Health Hum Rights. 2013 Jan 2;13:2.
Mastomys natalensis, natural host of Lassa virus. Photo courtesy of BioMed Central, originally published in Kelly JD, Barrie MB, Ross RA, Temple BA, Moses LM, Bausch DG. Housing equityfor health equity: a rights-based approach to the control of Lassa fever inpost-war Sierra Leone. BMC Int Health Hum Rights. 2013 Jan 2;13:2.
Bunyaviridae
This group includes Rift Valley fever (RVF) virus, Crimean-Congo hemorrhagic fever (CCHF) virus, and several hantaviruses. The RVF and CCHF viruses are both arthropod-borne viruses. RVF virus, an important African pathogen, is transmitted to humans and livestock by mosquitos and by the slaughter of infected livestock.
CCHF virus is carried by ticks and causes a fulminant, highly pathogenic form of VHF notable for aerosol transmission of infective particles (see the image below). CCHF virus has a wide geographic range that includes Africa, Asia, the Middle East, and Europe with sequence variation approaching 20% across the three negative-sense RNA genome segments. While phylogenetic clustering generally aligns with geographic origin of individual strains, distribution can be wide due to tick/CCHF virus dispersion via migrating birds. [1]
Many hantaviruses are spread worldwide, causing 2 major syndromes: hemorrhagic fever with renal syndrome (HFRS) and Hantavirus pulmonary syndrome (HPS). They are divided into Old World hantaviruses (such as the prototypical Hantaan virus of Korea), which generally cause HFRS, and New World hantaviruses, causing HPS. Rodents carry both types. A previously undiscovered Hantavirus, Sin Nombre virus, was the cause of an outbreak of highly lethal HPS in the southwestern United States in 1993. More than 450 cases have been identified in the US since 1993, with a 35% mortality rate. [2]
Filoviridae
The most notorious of the VHF viruses, Ebola and Marburg viruses, belong to the Filoviridae family. Both viruses originated in sub-Saharan Africa.
Ebola virus
Ebola virus (see the image below) was first described in 1976 after outbreaks of a febrile, rapidly fatal hemorrhagic illness were reported along the Ebola River in Zaire (now the Democratic Republic of the Congo) and Sudan. Sporadic outbreaks have continued since that time, usually in isolated areas of central Africa. An outbreak in Kikwit, Zaire, in 1995 led to 317 confirmed cases, with an 81% mortality rate. Two thirds of the cases were in health care workers caring for infected individuals. An outbreak in Uganda in late 2000 resulted in 425 cases and claimed 225 lives.
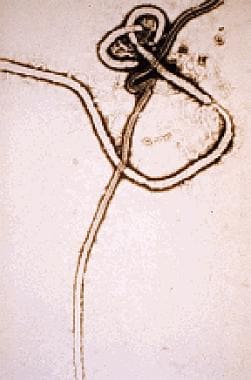 Ebola virus. Electron micrograph courtesy of the Centers for Disease Control and Prevention.
Ebola virus. Electron micrograph courtesy of the Centers for Disease Control and Prevention.
The largest Ebola outbreak to date occurred in West Africa from 2014 to 2016. This outbreak primarily occurred in Guinea, Sierra Leone, and Liberia, with >28,000 cases and >13,000 deaths. As a result of this outbreak, several sporadic cases of imported Ebola virus disease also occurred in industrialized nations, including the United States, the United Kingdom, Spain, and Italy.
From 2018 to 2020, the Democratic Republic of Congo (DRC) reported the emergence of another Ebola virus outbreak. As of June 2020, there were more than 3400 cases and 2200 deaths, making this the world’s second-largest Ebola outbreak to date. [3]
Ebola has 6 distinct subtypes:
-
Zaire ebolavirus
-
Sudan ebolavirus
-
Reston ebolavirus
-
Taï Forest ebolavirus
-
Bundibugyo ebolavirus
-
Bombali ebolavirus
The newest member of this genus is Bombali ebolavirus, discovered in 2018 and named after the Bombali area in Sierra Leone. [4] Reston ebolavirus causes illness in nonhuman primates and pigs but not in humans. [5]
Fruit bats have been identified as a reservoir for Ebola virus. [6]
Marburg virus
Marburg virus (see the image below), named after the German town where it first was reported in 1967, is another highly pathogenic member of the Filoviridae family that is traced to central Africa. As with Ebola virus, the natural host for the virus is likely the fruit bat. Marburg virus was contracted by a traveler to central Africa in 1987 and has been endemic since 1998 in Durba, Democratic Republic of the Congo, and in persons exposed in caves or mines.
 Marburg virus. Negative stain image courtesy of the Centers for Disease Control and Prevention.
Marburg virus. Negative stain image courtesy of the Centers for Disease Control and Prevention.
Marburg virus was determined to be the causative agent in a 2004-2005 outbreak of hemorrhagic fever in Angola that led to 252 confirmed cases and 227 deaths (90% case-fatality rate). In late 2012, an outbreak in Uganda resulted in 26 confirmed and probable cases of Marburg virus infection, including 15 deaths. [7]
Flaviviridae
Yellow fever and dengue fever are the most well-known diseases caused by flaviviruses. Both are mosquito-borne; yellow fever is found in tropical Africa and South America, and dengue fever is found in Asia, Africa, and the Americas. They are notable for their significant effect on prior military campaigns and their continued presence throughout endemic areas.
Due to a resurgence in the last 3 decades, dengue fever is now considered second only to malaria in terms of importance as a tropical disease. Multiple large outbreaks have occurred throughout the tropics recently, with the most severe outbreaks occurring in Southeast Asia and the western Pacific regions. Transmission is via the bite of the infected female Aedes mosquito, although dengue can also be transmitted via transfusion. [8]
Epidemiology
Frequency
United States
Cases of viral hemorrhagic fever (VHF) in the United States are extremely rare and usually are found in patients who recently have visited endemic areas or among those with potential occupational exposure to hemorrhagic fever viruses. Lassa fever has been reported in the United States in travelers from West Africa and was most recently reported in the United States in 2010. [9] In 1994, a virologist working with Sabia, a Brazilian HF virus, accidentally contracted the disease. Sporadic cases of Hantavirus pulmonary syndrome (HPS) continue to be reported throughout the western United States. [10]
During the 2014-2016 Ebola outbreak in West Africa, 2 imported cases were reported in the United States, including one death, as well as two locally acquired cases in healthcare workers. [11] In 1989, an outbreak of hemorrhagic fever among imported macaque monkeys in Reston, Virginia, led to the discovery of Reston ebolavirus, a variant of Ebola virus that originated in the Philippines and does not cause disease in humans.
An estimated 100-200 cases of imported dengue fever are reported in the United States each year. Occasional dengue outbreaks have occurred in the United States, and well-documented local transmission of dengue continues to occur in south Florida, specifically in Key West. [12]
International
Lassa fever is responsible for an estimated 100,000-300,000 infections per year, with 5,000 deaths. Cases have been reported throughout West Africa, particularly in Nigeria, Sierra Leone, Guinea, and Liberia. Other arenaviruses are responsible for sporadic VHF outbreaks throughout South America.
Rift Valley fever (RVF) virus and Crimean-Congo hemorrhagic fever (CCHF) are responsible for intermittent epidemics in Africa (for RVF) and in areas of Africa, Asia, and Europe (for CCHF). Hemorrhagic fever with renal syndrome (HFRS) due to Hantavirus infection continues to be an ongoing health concern, particularly in Asia, affecting up to 200,000 patients annually.
Ebola virus appears sporadically in endemic areas of the former Zaire and Sudan. Ebola virus also has been reported in Gabon, the Ivory Coast, and Uganda. Outbreaks appear to propagate in hospital settings, often involving health care providers. In the 2014-2016 outbreak centered in Guinea, Sierra Leone, and Liberia, over 28,652 confirmed cases and 11,325 deaths were reported. [13]
Yellow fever continues to be a serious problem in tropical areas of South America and Africa, where vaccination is not widespread. World Health Organization 2013 estimates suggest that 84,000 to 170,000 cases per year occur in Africa, with 29,000 to 60,000 deaths. [14] A yellow fever outbreak in Brazil from 2016-2019 involved more than 2200 cases and resulted in nearly 800 deaths. [15]
Dengue is endemic in Southeast Asia, Africa, Central America, and South America. Statistical models suggest that as many as 390 million cases may occur annually, of which 96 million manifest clinically. [16] According to the Pan American Health Organization, in 2018, a total of 560,586 cases of dengue were reported (incidence rate of 57.3 cases per 100,000 population) in the Americas, including 336 deaths. Rates of severe dengue and dengue with warning signs were higher than the previous 2 years but lower than in the preceding 10 years, and have remained below 1% of dengue cases overall since 2015. [17]
Prognosis
Case-fatality rates of patients with viral hemorrhagic fever (VHF) vary from less than 10% (eg, in dengue) to as high as 90%, as has been reported in some filovirus outbreaks. The case-fatality rate for the 2014-2016 West Africa Ebola outbreak was ~40%.
Complications from VHF include the following:
-
Retinitis
-
Orchitis
-
Encephalitis
-
Hepatitis
-
Transverse myelitis
-
Uveitis
Following the recent West Africa Ebola outbreak, a post-Ebola syndrome has been reported that consists of myalgias, arthralgias, visual problems including blindness and uveitis, and neurologic findings including memory problems, lethargy, and fatigue. [18] Persistence of Ebola virus RNA has been noted in semen samples even 13 months after infection, although a statistical analysis suggests that semen will be Ebola-free at 4 months in 50% of survivors. [19]
In patients who recover from Lassa fever infection, deafness is the most common complication. Spontaneous abortion also is common.
Recovery from hemorrhagic fever with renal syndrome may be complicated by chronic kidney disease.
-
Ebola virus. Electron micrograph courtesy of the Centers for Disease Control and Prevention.
-
Marburg virus. Negative stain image courtesy of the Centers for Disease Control and Prevention.
-
Mastomys rodent, natural host of Lassa virus. Image courtesy of the Centers for Disease Control and Prevention.
-
Bunyavirus infection. Ecchymoses encompassing left upper extremity one week after onset of CCHF. Ecchymoses often are accompanied by hemorrhage in other locations: epistaxis, puncture sites, hematemesis, melena, and hematuria. Image provided by Robert Swaneopoel, PhD, DTVM, MRCVS, National Institute of Virology, Sandringham, South Africa.
-
Apodemus agrarius, the vector of Korean hemorrhagic fever caused by a hantavirus. Photo courtesy of David McClain, MD.
-
Bunyavirus infection - Hantaan virus. Patient with Korean hemorrhagic fever caused by Hantaan virus demonstrating typical 'sunburn flush' of cheeks, chin, and base of neck. Photo courtesy of John Huggins, PhD.
-
Bunyavirus infection. A patient with Korean hemorrhagic fever demonstrating conjunctival hemorrhages, facial petechiae, and "sunburn flush" of the cheeks. Photo courtesy of John Huggins, PhD.
-
Filovirus disease - Ebola fever. Patient with Ebola hemorrhagic fever during 1976 outbreak in Zaire demonstrating palatal petechiae and hemorrhage. Photo courtesy of Joel Breman.
-
Patient with morbilliform exanthem of dengue fever. Note islands of sparing, which is characteristic for dengue. Photo courtesy Duane Gubler, PhD.
-
Patient with dengue hemorrhagic fever complicated by ecchymoses. Photo courtesy of Duane Gubler, PhD.
-
Dengue Virus Notice posted outside Maracanã Stadium, Rio de Janeiro, Brazil, 2012. Translation: This site is a strategic point for controlling Dengue.
-
Mastomys natalensis, natural host of Lassa virus. Photo courtesy of BioMed Central, originally published in Kelly JD, Barrie MB, Ross RA, Temple BA, Moses LM, Bausch DG. Housing equityfor health equity: a rights-based approach to the control of Lassa fever inpost-war Sierra Leone. BMC Int Health Hum Rights. 2013 Jan 2;13:2.
Tables
Virus Family |
Disease (Virus) |
Natural Distribution |
Usual Source of Human Infection |
Incubation (Days) |
Arenaviridae |
|
|
|
|
Arenavirus |
Lassa fever |
Africa |
Rodent |
5-16 |
|
Argentine HF (Junin) |
South America |
Rodent |
7-14 |
|
Bolivian HF (Machupo) |
South America |
Rodent |
9-15 |
|
Brazilian HF (Sabia) |
South America |
Rodent |
7-14 |
|
Venezuelan HF (Guanarito) |
South America |
Rodent |
7-14 |
Bunyaviridae |
|
|
|
|
Phlebovirus |
Rift Valley fever |
Africa |
Mosquito |
2-5 |
Nairovirus |
Crimean-Congo HF |
Europe, Asia, Africa |
Tick |
3-12 |
Hantavirus |
Hemorrhagic fever with renal syndrome, Hantavirus pulmonary syndrome |
Asia, Europe, worldwide |
Rodent |
9-35 |
Filoviridae |
|
|
|
|
Filovirus |
Marburg and Ebola |
Africa |
Fruit bat |
2-216 |
Flaviviridae |
|
|
|
|
Flavivirus |
Yellow fever |
Tropical Africa, South America |
Mosquito |
3-6 |
|
Dengue HF |
Asia, Americas, Africa |
Mosquito |
Unknown for dengue HF, 5-7 for dengue |





