Background
Sunburn is an acute cutaneous inflammatory reaction that follows excessive exposure of the skin to ultraviolet radiation (UVR). UVR exposure can come from a variety of sources, including sun, tanning beds, phototherapy lamps, and arc lamps. [1] Long-term adverse health effects of repeated exposure to UVR are well described but are beyond the scope of this article. Most sunburns are classified as superficial or first-degree burns.
See the image below.

Pathophysiology
Exposure to solar radiation has the beneficial effects of stimulating the cutaneous synthesis of vitamin D and providing radiant warmth. Unfortunately, when the skin is subjected to excessive radiation in the ultraviolet range, deleterious effects may occur. The most conspicuous is acute sunburn or solar erythema. [2]
The principal injury responsible for sunburn is direct damage to DNA by UVR, resulting in inflammation and apoptosis of skin cells. [3] Sunburn inflammation causes vasodilation of cutaneous blood vessels, resulting in the characteristic erythema. Within an hour of UVR exposure, mast cells release preformed mediators including histamine, serotonin, and tumor necrosis factor, leading to prostaglandin and leukotriene synthesis. [2, 4] Cytokine release additionally contributes to the inflammatory reaction, leading to an infiltrate of neutrophils and T lymphocytes. [5] Within 2 hours after UV exposure, damage to epidermal skin cells is seen. Both epidermal keratinocytes ("sunburn cells") and Langerhans cells undergo apoptotic changes as a consequence of UVR-induced DNA damage. [6, 7] Erythema usually occurs 3-4 hours after exposure, with peak levels at 24 hours. [8]
See the image below.
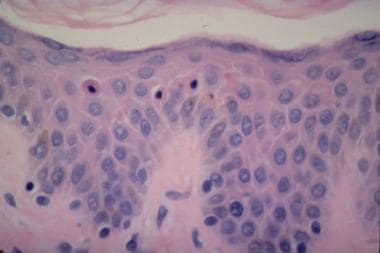 Note the apoptotic sunburn cells in the epidermis. Photograph courtesy of David Shum, MD, Division of Dermatology, University of Western Ontario.
Note the apoptotic sunburn cells in the epidermis. Photograph courtesy of David Shum, MD, Division of Dermatology, University of Western Ontario.
Less intense or shorter-duration exposure to UVR results in an increase in skin pigmentation, known as tanning, which provides some protection against further UVR-induced damage. [9] The increased skin pigmentation occurs in 2 phases: (1) immediate pigment darkening and (2) delayed tanning. Immediate pigment darkening occurs during exposure to UVR and results from alteration of existing melanin (oxidation, redistribution). It may fade rapidly or persist for several days. Delayed tanning results from increased synthesis of epidermal melanin and requires a longer period of time to become visible (24-72 h). With repeated exposure to UVR, the skin thickens, primarily due to epidermal hyperplasia with thickening of the stratum corneum. UVR exposure also suppresses cutaneous cell–mediated immunity, which might contribute to nonmelanoma skin cancer and certain infections. [2]
Etiology
Sunburn is caused by excessive exposure of the skin to UVR. The ultraviolet spectrum can be divided into ultraviolet A-I (UVA-I), 340-400 nm; ultraviolet A-II (UVA-II), 320-340 nm, ultraviolet B (UVB), 290-320 nm; and ultraviolet C (UVC), 200-290 nm. [1] Solar UVR of wavelengths shorter than 290 nm are filtered out or absorbed in the outer atmosphere and are not encountered at sea level. [1] Shorter wavelength UVB rays are much more effective at inducing erythema than UVA rays and, therefore, are the principal cause of sunburn. [1] However, UVA comprises the majority of UVR reaching the surface of the earth (about 95-98% at midday) and, therefore, accounts for a significant percentage of the immediate and long-term cutaneous effects of UVR. [1]
The minimal single dose of UVR (energy per unit area) required to produce erythema after 24 hours at an exposed site is known as the minimal erythema dose (MED). This dose differs by skin type. [2]
Multiple factors influence UVR-induced erythema; these are listed below:
-
Wavelength: UVB is more erythemogenic than UVA. [2]
-
Skin type/pigmentation: Compared with type I-II skin, patients with type IV-V skin require 3-5 times more UVR exposure to cause erythema. [10]
-
Hydration: UVR causes erythema in moist skin more effectively than dry skin. [11]
-
Environmental reflection: Radiation is 80% reflected by snow and ice, compared with 15% by sand. [12]
-
Ozone coverage: Increased levels of ozone filter out more UVR. [12]
-
Altitude: Thinner atmosphere at higher altitudes absorbs less UVR. [12]
-
Latitude: Exposure is greater nearer the equator. [12]
-
Time of day: UVR exposure is greatest from 10 am to 4 pm, when the sun is highest in the sky. [12]
-
Season: In locations outside the tropics, UVR is much greater in summer than winter. [12]
-
Cloud cover: Light clouds attenuate UVR by 10%, which may not be enough to protect from sunburn. [12]
Epidemiology
Frequency
United States
Previous reports have stated that about one third of US adults have a sunburn each year [13, 14] and about two thirds of US children have a sunburn each summer. [15] The US Centers for Disease Control and Prevention (CDC) reported in 2012 that just over 50% of all adults reported at least one sunburn in the past 12 months and that just over 65% of whites aged 18-29 years reported at least one sunburn in the past 12 months. [16]
International
Risk of sunburn is increased in regions that are closer to the equator and that are higher in altitude. [12]
Race
Lighter-skinned individuals are affected more frequently and severely. Skin types are traditionally classified into the following Fitzpatrick categories, based on an individual's tendency to tan, burn, or both (see the Table below).
Table. Fitzpatrick Skin Types and Recommended Sunscreen Sun Protection Factor (SPF) Levels [2, 10, 17] (Open Table in a new window)
Skin Type |
Description |
Skin Color |
Routine SPF |
SPF for Outdoor Activity |
I |
Always burns, never tans |
White |
15 |
25-30 |
II |
Always burns, tans minimally |
White |
12-15 |
25-30 |
III |
Burns minimally, tans slowly |
White |
8-10 |
15 |
IV |
Burns minimally, tans well |
Olive |
6-8 |
15 |
V |
Rarely burns, tans profusely/darkly |
Brown |
6-8 |
15 |
VI |
Rarely burns, always tans |
Black |
6-8 |
15 |
Sex
Surveys of US adults show that men have a slightly higher prevalence of sunburn than women. [13]
Age
Sunburn is more common in children than in adults. [14, 15] Easy sunburning during infancy may indicate a serious underlying disease, such as porphyria or xeroderma pigmentosum. Referral for further evaluation is prudent. [18]
Prognosis
Uncomplicated sunburn is associated with minimal short-term morbidity. Most cases resolve spontaneously with no significant sequelae. In rare cases, sunburn may be so severe and diffuse that it results in second-degree burns, dehydration, or secondary infection. [8]
Morbidity and mortality associated with long-term sun exposure is related primarily to the development of cutaneous neoplasms, including basal cell carcinoma, squamous cell carcinoma, and malignant melanoma. [2] For more information on skin cancers, see Medscape's Skin Cancer Resource Center.
Patient Education
Educate patients on the short- and long-term complications (see Complications).
Educate patients on prevention of sunburn (see Prevention).
For patient education resources, see the patient education article Sunburn.
-
Note the apoptotic sunburn cells in the epidermis. Photograph courtesy of David Shum, MD, Division of Dermatology, University of Western Ontario.
-
Acute sunburn of face after a soccer match in a 15 year-old female.
-
Subacute sunburn of shoulder with peeling in a 21-year-old male.
Tables
Skin Type |
Description |
Skin Color |
Routine SPF |
SPF for Outdoor Activity |
I |
Always burns, never tans |
White |
15 |
25-30 |
II |
Always burns, tans minimally |
White |
12-15 |
25-30 |
III |
Burns minimally, tans slowly |
White |
8-10 |
15 |
IV |
Burns minimally, tans well |
Olive |
6-8 |
15 |
V |
Rarely burns, tans profusely/darkly |
Brown |
6-8 |
15 |
VI |
Rarely burns, always tans |
Black |
6-8 |
15 |








