Practice Essentials
Tracheobronchial foreign bodies are most commonly caused by aspiration and can result in a spectrum of presentations, from minimal symptoms, often unobserved, to respiratory compromise, failure, and even death. The epidemiology of tracheobronchial foreign bodies is bimodal, with peaks at the extremes of age.
Children aged 1-3 years are particularly at risk because of their increasing independence, mobility, and curiosity; decreased intensity of parental supervision with increased age; and the frequent tendency of young children to investigate their environment with their hands and mouths. Children in this age group are at risk for aspiration of various foods (grapes, raisins, nuts, seeds, candy), small toys, and balloons, as well as any object less than 1.5 cm in diameter.
Elderly patients are also at risk, particularly those with primary neurologic disorders such as stroke, Parkinson disease, and dementia, as well as patients of any age with a decreased gag reflex due to alcohol, drug overdose, seizures, or trauma. Any number of substances or objects can be aspirated, including food, gastric contents, pills, dental appliances, and teeth.
A third category of at-risk individuals is those undergoing procedures with sedation, particularly dental procedures or emergency intubation.
The diagnosis is often missed initially, especially in children where the history may be vague and the patient cannot verbalize the events. [1] In as many as 30% of patients, symptoms are treated as those of other common diseases, especially in patients with minimal symptoms. [2, 3] A high index of suspicion is required to make the diagnosis, especially in children and patients who are debilitated. [4]
Signs and symptoms of tracheal foreign bodies
Choking or coughing is present in 95% of patients presenting with foreign body aspiration. [4] Stridor is commonly present with upper airway or upper tracheal foreign bodies. Patients may present with respiratory distress, pneumonia, pulmonary edema, or wheezing.
Workup in tracheal foreign bodies
Computed tomography (CT) scanning is rapidly becoming the imaging study of choice in stable patients with suspected aspiration. [5, 6, 7]
Posteroanterior and lateral chest films are often used as an initial screening test. Bronchoscopy may be necessary to assist in making the diagnosis when other tests do not reveal the problem.
Management of tracheal foreign bodies
Emergency department care
Initial supportive therapy includes oxygen administration, cardiac monitor, pulse oximetry, and intravenous (IV) line. Definitive airway management may be required.
In stridorous patients, racemic epinephrine via a nebulizer may be a temporizing measure until bronchoscopy can be performed.
In unstable patients, rapid sequence intubation may be needed.
Extraction by bronchoscopy is the treatment of choice for tracheal foreign bodies. [8, 9, 10, 11] In children, bronchoscopy is performed with general anesthesia in the operating room, with inhalational induction generally preferred. Adults may tolerate awake or sedated bronchoscopy if nebulized lidocaine (4%) is used.
Pathophysiology
Aspirated foreign bodies most commonly are lodged in the right main stem and lower lobe. Aspiration has been documented in all lobes, including the upper lobes, though with less frequency.
In the United States, peanuts are by far the most commonly aspirated material in children, followed by organic material such as sunflower seeds, pieces of vegetables, and hazelnuts. [4] In other countries, the most common aspirated material remains food items, especially small seeds such as peanuts, corn, and peas, but other types of food differs from culture to culture. [12, 13]
In adults, vegetable matter, meat, and bones rank highest, followed by dental and medical appliances. Aspiration of teeth after trauma is occasionally observed.
Etiology
Mortality
Choking is the fourth leading cause of accidental injury death in the United States. According to the National Safety Council, 3000 people suffered choking deaths in 2020, including 1430 persons older than age 74 years. [14]
Sex
Male predominance is found in most studies, particularly in children. Approximately 60% of patients male. [4, 13, 11]
Age
Age frequency is bimodal, with individuals aged 1-3 years and those in the seventh decade of life at higher risk of foreign body aspiration.
Clinical Presentation
History
The history leads to diagnosis in most cases. [12, 2]
In adults, aspiration occurs with choking after eating or choking when holding a foreign body in the mouth. Aspiration should also be suspected in adults with respiratory distress associated with sedation from drugs, alcohol, or trauma; after medical procedures such as sedation or intubation; after facial trauma; and in patients with decreased ability to handle secretions. In particular, patients with strokes, either new or old, are at high risk for aspiration.
Suspicion of foreign body aspiration in children is raised with sudden paroxysms of coughing when not directly supervised, sudden choking after eating (particularly when an older sibling feeds a younger sibling), or choking and/or coughing when a known, small object or food particle (particularly peanuts) is within reach of the child. [4, 2]
In children undergoing treatment of new-onset asthma, bronchitis, or pneumonia that is not responding to appropriate treatment (ie, bronchodilators, steroids, antibiotics), consider the possibility of foreign body aspiration, particularly with unilateral wheezing, [3, 13] although in children with asthma, the diagnosis can be confusing as wheezing is a confounding physical finding. Asthmatic children have a higher rate of negative bronchoscopy for foreign body. [15]
Physical
Choking or coughing is present in 95% of patients presenting with foreign body aspiration. [4] Stridor is commonly present with upper airway or upper tracheal foreign bodies. Patients may present with respiratory distress, pneumonia, pulmonary edema, or wheezing.
Children present similarly. Approximately 50% of children have inspiratory stridor or expiratory wheezing, with prolongation of the expiratory phase, and medium-to-coarse rhonchi. [16] Tachypnea; nasal flaring; intercostal, subcostal, and suprasternal retractions; and differences in percussion between hemithoraces also are common findings. [16] Fever and central cyanosis are less common. Only rarely do children with a positive history have an examination with completely normal findings. [4, 9]
Stridor in children or adults indicates a partial upper airway or tracheal occlusion and is an ominous sign. These patients require prompt interventions.
Causes
In children, the primary factors leading to aspiration are underlying curiosity about the world and the oral phase of children aged 1-3 years. Loose, small objects and food found around the household increase risk. An older sibling feeding younger children is an important historical clue.
Objects that tend to stay in the mouth for prolonged periods of time, such as gum, sunflower seeds, or hard candy, also increase risk. Eating while lying supine, especially just prior to falling asleep, increases risk of aspiration.
Baby powder can be a particularly dangerous aspiration. A symptom-free period may occur before suffocation. Immediate lavage of bronchial system is required in severe cases.
In adults, factors that increase risk are underlying primary neurologic disorders, such as dementia, intellectual disability, seizures, strokes, and parkinsonism. Conditions that depress the central nervous system, cause coma, or depress the gag reflex, such as alcohol, narcotics, barbiturates, or benzodiazepines, can increase likelihood of aspiration.
Meats, bones, and medical and dental appliances are the most commonly aspirated objects in adults. In patients who have sustained facial or dental trauma, including traumatic intubations, who have a missing tooth, the tooth must be presumed to have been aspirated, and radiographic evaluation is needed.
A retrospective study by Sasso et al reported that out of 27,381 US emergency department visits in 2013 for suffocation injuries, as assessed using the Nationwide Emergency Department Sample database, 14,140 (51.6%) resulted from inhalation and ingestion of food. [17]
Differential Diagnosis
Workup
Lab studies
Complete blood count (CBC) and sedimentation rate may be elevated, particularly with chronic foreign bodies. In patients going to the operating room for bronchoscopy, routine preoperative laboratory studies are indicated.
Imaging studies
Computed tomography (CT) scanning is rapidly becoming the imaging study of choice in stable patients with suspected aspiration. [5, 6, 7] This is especially true because the majority of tracheal foreign bodies (plant seeds) are radiolucent. CT is very accurate in identifying and localizing foreign bodies.
A study by Behera et al indicated that virtual bronchoscopy using multidetector CT (MDCT) scanning is effective in diagnosing the presence of radiolucent vegetable foreign bodies in the tracheobronchial airway. The study found that in 59 out of 60 pediatric cases, rigid bronchoscopy confirmed MDCT-scan findings with regard to the presence of a vegetable foreign body, as well as the foreign body's size, shape, and location, giving virtual bronchoscopy a positive predictive value of 98.3%. [18]
Posteroanterior and lateral chest films are often used as an initial screening test. Foreign bodies, atelectasis, air trapping, mediastinal shift, compensatory emphysema on the contralateral side, pneumonia, or pneumothorax may be observed. [19, 20, 21]
Hyperlucency and atelectasis are observed in 63% of cases in children. Bilateral decubitus films may be helpful in children. A foreign object may prevent normal pulmonary collapse when the involved hemithorax is dependent (or on the "down" side, on the radiography table). However, a recent large study brings into question the test accuracy and clinical benefit of these radiographs, showing an increase in false positives without any increase in true positives. [22] In very young children, decubitus films are not helpful. [20] Expiratory films may be of some benefit.
Fluoroscopy may show Holzknecht-Jacobson phenomena (swinging mediastinum).
In patients with stridor, a soft-tissue lateral film of the neck may be useful.
 Aspirated foreign body (backing to an earring) lodged in the right main stem bronchus.
Aspirated foreign body (backing to an earring) lodged in the right main stem bronchus.
 A tooth (molar) was dislodged during intubation and can be observed in the right hilum. It was not noticed on initial review of this film.
A tooth (molar) was dislodged during intubation and can be observed in the right hilum. It was not noticed on initial review of this film.
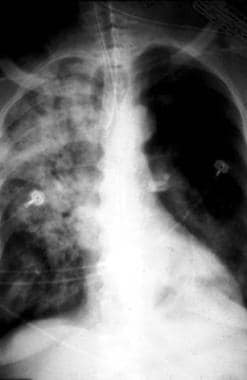 A tooth (molar) was dislodged during intubation. The patient developed a lobar pneumonia from the tooth, which on this radiograph has migrated to the left hilum. Attempts at removal by bronchoscopy were unsuccessful, and the tooth was removed surgically.
A tooth (molar) was dislodged during intubation. The patient developed a lobar pneumonia from the tooth, which on this radiograph has migrated to the left hilum. Attempts at removal by bronchoscopy were unsuccessful, and the tooth was removed surgically.
Procedures
Bronchoscopy may be necessary to assist in making the diagnosis when other tests do not reveal the problem.
Treatment & Management
Prehospital care
If the patient is coughing, wheezing, or is stridorous but maintaining an airway, do not attempt to intervene; transport to the nearest facility where definitive treatment can be provided.
If severe airway compromise or total obstruction occurs, attempt chest compressions, back blows, abdominal thrusts, or the Heimlich maneuver. The method depends on the age of the patient.
Emergency department care
Initial supportive therapy includes oxygen administration, cardiac monitor, pulse oximetry, and intravenous (IV) line. Definitive airway management may be required.
In stridorous patients, racemic epinephrine via a nebulizer may be a temporizing measure until bronchoscopy can be performed.
In patients who experience out-of-hospital cardiac arrest associated with airway foreign body aspiration, the use of Magill forceps has been associated with improved outcomes. [23] This approach utilizes a laryngoscope and Magill forceps to remove supraglottic foreign bodies.
The use of ketamine, a short-acting, dissociative anesthetic and analgesic, may be useful in the examination of the nose, nasopharynx, and oropharynx in children. Although the agent produces a dissociative state, the patient maintains respiratory and airway reflexes. The drug has an action duration of 15-30 minutes; the dose is 1-2 mg/kg intravenously or 4-5 mg/kg intramuscularly. Laryngospasm is an uncommon adverse effect. In children, ketamine can cause increased salivation and respiratory secretions; atropine is often given in adjunct in a dose of 0.01 mg/kg (maximum of 0.5 mg). In patients with a true airway foreign body involving the glottis and distal airways, this approach is not recommended. For further information, see Sedation.
In unstable patients, rapid sequence intubation may be needed. In these cases, be prepared with suction and Magill forceps. In emergent situations with tracheal foreign bodies below the level of the vocal cords, intubation may be required. One option is to insert the endotracheal tube all the way to the hub, thus pushing the foreign body down into a mainstem bronchus (normally, the right). The endotracheal tube is then removed to the normal position (normally 20-22 cm at the lips in adults), and the patient is ventilated after ensuring the tip of the tube is not occluded with the foreign body. Even though only one lung will be ventilated, sufficient air exchange and oxygenation should occur to allow the patient to be taken for formal bronchoscopy.
Extraction by bronchoscopy is the treatment of choice for tracheal foreign bodies. [8, 9, 10, 11]
In children, bronchoscopy is performed with general anesthesia in the operating room, with inhalational induction generally preferred. Adults may tolerate awake or sedated bronchoscopy if nebulized lidocaine (4%) is used. Complications of bronchoscopy generally are uncommon and self-limited. However, in-hospital mortality is reportedly 1-2%, partially attributable to large tracheal foreign bodies lost during a procedure. The lost foreign body may become lodged in the subglottic region, causing complete airway obstruction.
A retrospective study by Zhang et al of 3149 pediatric patients found that with regard to rigid bronchoscopy for suspected inhaled tracheobronchial foreign bodies, the rate of severe postprocedure complications—specifically, severe hypoxemia, complete laryngospasm, laryngeal edema, pneumothorax, total segmental atelectasis, and death—was 9% (or individually, 3.2%, 1.3%, 0.9%, 0.3%, 0.3%, and 0.1%, respectively). [24]
A retrospective study by Tenenbaum et al indicated that, if performed in an optimized clinical setting, flexible bronchoscopy carried out through a laryngeal mask can effectively remove airway foreign bodies in children. Using flexible bronchoscopy, an airway foreign body was found in 28 children in the study, with the object removed through this procedure—via a grasping forceps, a basket forceps, suction, or a polypectomy snare—in all of these patients. [25]
A study by Golan-Tripto et al performed on pediatric patients also indicated that, if carried out by an experienced multidisciplinary team, flexible bronchoscopy can be effectively used in children with inhaled foreign bodies. The rates of success for foreign body removal by rigid and flexible bronchoscopy were 88.73% and 95%, respectively, while complication rates were 9.2% and 0%, respectively. Procedure length for rigid bronchoscopy was 58 minutes, versus 42 minutes for flexible bronchoscopy. Length of hospital stay was comparable between the two groups. [26]
If initial bronchoscopy is unsuccessful, a repeat attempt usually is performed. Rarely, a second attempt is unsuccessful, and thoracotomy is necessary. If the foreign body has expanded (as can occur with organic matter) or is larger than the subglottic region, a tracheostomy may be required.
Follow-up
Further Inpatient Care
Admit patients with suspected foreign body aspiration to the hospital. These patients require bronchoscopy, observation, and possibly antibiotics.
Transfer
Transfer stable patients who require intervention (normally bronchoscopy) that is not available at the current facility. Typically, this will be pediatric patients who are transferred to a pediatric center. Ensure ALS personnel who are capable of airway management in case of deterioration are used as the transport team.
Prevention
Avoid feeding children younger than 3 years dried nuts, such as peanuts, which account for a large majority of tracheal aspirations in this age group.
Complications
Complications include atelectasis, recurrent pneumonia, pulmonary compromise, and pulmonary infarct. [4]
Prognosis
The prognosis for complete tracheal obstruction from aspirated foreign body is grim, unless immediate action such as the Heimlich maneuver, back blows, or chest thrusts are used. In patients with foreign bodies that are not occlusive, or are in a main-stem bronchus, the prognosis is excellent if a high level of suspicion is maintained, and early intervention such as CT and bronchoscopy are used. [4, 19]
Medical Therapy
Corticosteroids
These agents have anti-inflammatory properties and cause profound and varied metabolic effects. Corticosteroids modify the body's immune response to diverse stimuli. Tenenbaum et al found that 85.7% of patients with proven airway foreign bodies were given IV/oral steroids either preceding or following bronchoscopic retrieval. [25] Corticosteroids that can be used in patients with trachea foreign bodies include the following:
Antibiotics
Empiric antimicrobial therapy—in which nafcillin and cefazolin are agents—must be comprehensive and should cover all likely pathogens in the context of the clinical setting. In the aforementioned study by Tenenbaum et al, 53.6% of patients with proven airway foreign bodies were treated with antibiotics around the time of surgery. [25]
Local epinephrine
Local epinephrine can occasionally be used to provide vasoconstriction and facilitate extraction of a lodged tracheobronchial foreign body. [25]
Dissociative agents
Ketamine elicits profound dissociative and amnestic actions. It does not affect pharyngeal-laryngeal reflexes and, thus, allows a patent airway as well as spontaneous respiration to maintain intact.
Ketamine (Ketalar) is a short-acting dissociative anesthetic and analgesic agent. It acts on the cortex and limbic system, decreasing bronchospasm.
-
Aspirated foreign body (backing to an earring) lodged in the right main stem bronchus.
-
A tooth (molar) was dislodged during intubation and can be observed in the right hilum. It was not noticed on initial review of this film.
-
A tooth (molar) was dislodged during intubation. The patient developed a lobar pneumonia from the tooth, which on this radiograph has migrated to the left hilum. Attempts at removal by bronchoscopy were unsuccessful, and the tooth was removed surgically.





