Background
Trigeminal neuralgia (TN), also known as tic douloureux, is a pain syndrome often recognizable by the patient's history alone. Trigeminal neuralgia is characterized by facial pain often accompanied by a brief facial spasm or tic. Pain distribution is unilateral and follows the sensory distribution of cranial nerve V, typically radiating to the maxillary (V2) or mandibular (V3) area, or rarely, the ophthalmic (V1) area. [1] At times, both distributions are affected. Physical examination will usually eliminate alternative diagnoses. Signs of dysfunction of other cranial neruves or other neurologic abnormality exclude the diagnosis of classic trigeminal neuralgia and suggest that pain may be secondary to a structural lesion.
The International Association for the Study of Pain (IASP) classifies TN into three categories. Classical TN is described as vascular compression that causes anatomical changes in the trigeminal nerve root. Next, secondary TN is due to an underlying neurologic disease. Third, idiopathic TN, is diagnosed after all studies reveal no etiology or there is no apparent cause. [2]
Classic trigeminal neuralgia includes all cases without established etiology after investigation, as well as those with potential microvascular compression of the fifth cranial nerve. In symptomatic trigeminal neuralgia, the pain syndrome is secondary to tumor, multiple sclerosis, or other structural abnormalities. [3]
Diagnosis
According to the International Classification of Headache Disorders (ICHD), specific crtieria have been developed to diagnose TN. [2] They are as follows:
A. At least three attacks of unilateral facial pain fulfilling criteria B and C
B. Occurring in one or more divisions of the trigeminal nerve, with no radiation beyond the trigeminal distribution
C. Pain has at least three of the following four characteristics:
- recurring in paroxysmal attacks lasting from a fraction of a second to 2 min
- severe intensity
- electric shock-like, shooting, stabbing or sharp in quality
- precipitated by innocuous stimuli to the affected side of the face
D. No clinically evident neurological deficit
E. No alternative diagnosis
Pathophysiology
The mechanism of pain production remains controversial. One theory suggests that peripheral injury or disease of the trigeminal nerve increases afferent firing in the nerve; failure of central inhibitory mechanisms may be involved as well. Pain is perceived when nociceptive neurons in a trigeminal nucleus involve thalamic relay neurons. An abnormal vascular course of the superior cerebellar artery is often cited as the cause, as well as other small arteries or veins compressing the facial nerve. In about 85% of cases, no lesion is identified, even after extensive investigations, and the etiology is labeled idiopathic (classic) by default.
Aneurysms, tumors, chronic meningeal inflammation, or other lesions may irritate trigeminal nerve roots along the pons, causing symptomatic trigeminal neuralgia. Uncommonly, an area of demyelination from multiple sclerosis may be the precipitant. Lesions of the entry zone of the trigeminal roots within the pons may cause a similar pain syndrome.
An area of demyelination is shown in the image below.
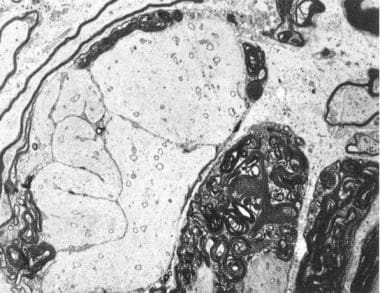 Microscopic demonstration of demyelination in primary trigeminal neuralgia. A tortuous axon is surrounded by abnormally discontinuous myelin. Electron microscope, 3, 300 X.
Microscopic demonstration of demyelination in primary trigeminal neuralgia. A tortuous axon is surrounded by abnormally discontinuous myelin. Electron microscope, 3, 300 X.
Infrequently, adjacent dental fillings composed of dissimilar metals may trigger attacks, [4] and an atypical case has been reported following tongue piercing. A case report of trigeminal neuralgia in a patient with spontaneous intracranial hypotension has been reported; both conditions resolved following surgical treatment of a cervical root sleeve dural defect. [5]
Epidemiology
Frequency
Trigeminal neuralgia (TN) is uncommon, with an estimated prevalence of 155 cases per million persons. In patients over 75 years old it can occur in up to 1 per 1000 patients. Females are affected twice as often as males. [6]
Mortality/Morbidity
No mortality is associated with idiopathic trigeminal neuralgia (TN), although secondary depression is common if a chronic pain syndrome evolves. Depression can be severe enough that some patients have committeed suicide. Many patients suffer from decreased quality of life and imparirment of daily function. [1] In rare cases, pain may be so frequent that oral nutrition is impaired.
In symptomatic or secondary trigeminal neuralgia, morbidity or mortality relates to the underlying cause of the pain syndrome.
Age
Development of trigeminal neuralgia in a young person suggests the possibility of multiple sclerosis.
Idiopathic trigeminal neuralgia typically occurs in patients in the fifth to eigth decade of life, but it may occur at any age.
Symptomatic or secondary trigeminal neuralgia tends to occur in younger patients.
-
Microscopic demonstration of demyelination in primary trigeminal neuralgia. A tortuous axon is surrounded by abnormally discontinuous myelin. Electron microscope, 3, 300 X.
-
MRI with high resolution on the pons demonstrating the trigeminal nerve root. In this case, the patient with trigeminal neuralgia has undergone gamma-knife therapy, and the left-sided treated nerve (arrow) is enhanced by gadolinium.