Background
Relapsing fever is a bacterial infection caused by spirochetes of the genus Borrelia. It is characterized by recurring episodes of high fever, headache, and muscle and joint aches. The high fevers of presenting patients spontaneously abate and then recur. This characteristic pattern of remission and relapse not only gives relapsing fever its name but also allows it to be differentiated clinically from other febrile illnesses as it has since the 1840s.
There are two types of relapsing fever: tick-borne relapsing fever (TBRF) and louse-borne relapsing fever (LBRF).
Tick-borne relapsing fever
The two main Borrelia species in North America include Borrelia hermsii (in the west), and Borrelia turicatae (southwest and south central). Relapsing fever caused by these species is usually associated with sleeping in rustic, rodent-infested settings, especially in mountainous areas.
Louse-borne relapsing fever
Louse-borne relapsing fever is caused by Borrelia recurrentis, which is usually transmitted by the human body louse. Thus, louse-borne relapsing fever generally is restricted to refugee settings in developing countries.
Large outbreaks of louse-borne relapsing fever have occurred throughout the past century. These outbreaks usually occur following man-made breakdowns in public health, as typified by the epidemic following World War II that involved about 10 million people.
Pathophysiology
Relapsing fever is transmitted to humans by 2 vectors, ticks and lice. The human body louse, Pediculus humanus, is the specific vector (Pediculus pubis is not a vector). Louse-borne relapsing fever is more severe than the tick-borne variety.
Louse-borne relapsing fever is caused by B recurrentis, which is transmitted from human to human via the body louse. No animal reservoir exists. Lice that feed on infected humans acquire the Borrelia organisms that then multiply in the gut of the louse. When an infected louse feeds on an uninfected human, the organism gains access when the victim crushes the louse or scratches the area where the louse is feeding. B recurrentis infects the person via either abraded or intact skin (or mucous membranes) and then invades the bloodstream.
Soft ticks of the genus Ornithodoros spread the tick-borne variety. The responsible Borrelia species are identified closely with its tick vector and they share parallel nomenclature. (For example, Borrelia parkeri infects Ornithodoros parkeri; Borrelia hermsii is the agent transmitted by tick bite by Ornithodoros hermsii.) Soft ticks differ in 2 important ways from the more familiar hard ticks (eg, dog tick and deer tick). First, soft ticks feed for short periods (< 30 minutes), and the Borrelia organisms are inoculated within minutes. This is an important distinction from other tick-borne diseases such as Lyme disease. Second, soft ticks do not search for a prey in tall grass or bush; instead, they live within rodent burrows, feeding as needed on the rodent as it sleeps. [1]
 Relapsing fever can be tick- or louse-borne. Soft-bodied ticks of the genus Ornithodoros transmit tick-borne cases. Above is an image of such a tick. Unlike the hard-bodied ticks, the Ornithodoros feed briefly and can transmit disease within minutes. Photo courtesy of Julie Rawlings, MPH, Texas Department of Health.
Relapsing fever can be tick- or louse-borne. Soft-bodied ticks of the genus Ornithodoros transmit tick-borne cases. Above is an image of such a tick. Unlike the hard-bodied ticks, the Ornithodoros feed briefly and can transmit disease within minutes. Photo courtesy of Julie Rawlings, MPH, Texas Department of Health.
Regardless of the mode of transmission, a spirochetemia develops. Borrelia organisms then invade the endothelium. This can produce a low-grade disseminated intravascular coagulation and thrombocytopenia. The relapse phenomenon occurs because of genetically programmed shifting of outer surface proteins of the Borrelia that allows a new clone to avoid destruction by antibodies directed against the majority of the original infecting organisms. Thus, the person clinically improves until the new clone multiplies sufficiently to cause another relapse. Tick-borne disease tends to have more relapses (average of 3) compared with the louse-borne variety (often just 1).
The recent resurgence of interest in Borrelia because of Lyme disease and, especially the recent publication of the genomic sequence of B burgdorferi, has led to advances in the understanding of the host-parasite interactions of the relapsing fever Borrelia.
Epidemiology
Frequency
United States
Louse-borne relapsing fever is not endemic in the United States, although an occasional traveler presents with an imported case.
Few cases of tick-borne relapsing fever are reported in the United States; however, sporadic cases continue to occur. It is highly focal, with 13 counties producing 50% of cases. Most of these are found in the late spring and summer in the western mountainous states, south into California and Colorado and northwest into Washington. Undoubtedly, many cases occur that either are misdiagnosed or unreported.
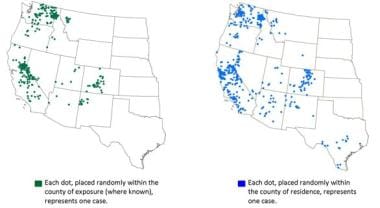 Cases of Tick-borne Relapsing Fever - United States, 1990-2011. Courtesy of the Centers for Disease Control and Prevention (CDC).
Cases of Tick-borne Relapsing Fever - United States, 1990-2011. Courtesy of the Centers for Disease Control and Prevention (CDC).
International
Endemic foci of louse-borne relapsing fever occur in much of the world where war, poverty, and overcrowding exist; all of these are conditions that favor louse infestation. Civil wars, which result in large refugee camps, also are fertile ground for lice and relapsing fever. [2, 3, 4, 5, 6]
Louse-borne relapsing fever epidemics were common in Europe during the 20th century. Between 1919 and 1923, 13 million cases, resulting in 5 million deaths, occurred in social upheaval that overtook Russia and Eastern Europe. During World War II, a million cases occurred in North Africa. Today, louse-borne relapsing fever causes sporadic illness and outbreaks in sub-Saharan Africa, particularly in regions affected by war and in refugee camps. [7, 8, 9, 10]
Mortality/Morbidity
Mortality rates from 30-70% are reported in untreated patients during epidemics of the louse-borne variety; the mortality rate falls to about 5% with treatment. This striking figure probably reflects the underlying malnutrition and coexisting infections that exist in these situations.
The mortality rate of patients with tick-borne relapsing fever who are treated is less than 1%.
Sex
A slight preponderance of female patients exists in louse-borne epidemics (60%); tick-borne relapsing fever occurs more often in males (60%) than in females. The latter figure probably reflects the greater likelihood of males being exposed to ticks through recreational and occupational activities.
Age
A trend toward pediatric cases of both forms of relapsing fever exists. In the case of the louse-borne variety, this may reflect the general state of health in populations where relapsing fever is endemic. Regarding the tick-borne disease, this may reflect activities that lead to tick exposure.
Prognosis
The mortality rates of untreated louse-borne relapsing fever and tick-borne relapsing fever range from 10-70% and 4-10%, respectively.
With prompt antibiotic treatment, the mortality rate of louse-borne relapsing fever and tick-borne relapsing fever decreases to 2-5% and less than 2%, respectively. [11]
The following features are associated with a poor prognosis:
-
Stupor or coma on admission
-
Diffuse bleeding
-
Myocarditis
-
Poor hepatic function
-
Bronchopneumonia
-
Coinfection with malaria, typhoid, or typhus
Patient Education
Educate patients about the vectors and how they can be avoided.
For excellent patient education resources, see eMedicineHealth's patient education article Ticks.
-
Relapsing fever can be tick- or louse-borne. Soft-bodied ticks of the genus Ornithodoros transmit tick-borne cases. Above is an image of such a tick. Unlike the hard-bodied ticks, the Ornithodoros feed briefly and can transmit disease within minutes. Photo courtesy of Julie Rawlings, MPH, Texas Department of Health.
-
Photomicrograph of a patient who presented to the ED with cyclical fevers and chills, which she developed while traveling in one of the recently formed Soviet Republics in 1990. A blood smear for malaria was obtained, and this is what the laboratory technician observed.
-
Cases of Tick-borne Relapsing Fever - United States, 1990-2011. Courtesy of the Centers for Disease Control and Prevention (CDC).