Practice Essentials
Poisoning with the neurotoxin tetrodotoxin (TTX) occurs after ingestion of various species of puffer fish (see the image below).

The flesh of the puffer fish (ie, fugu) is considered a delicacy in Japan. It is prepared by chefs specially trained and certified by the government to prepare the flesh free of the toxic liver, gonads, and skin. Despite these precautions, many cases of tetrodotoxin poisoning are reported each year in patients ingesting fugu. Poisonings usually occur after eating fish caught and prepared by uncertified handlers.
While the US Food and Drug Administration (FDA) does allow legal importation of puffer fish into the United States, through a single certified Japanese importer, [1] illegal importation continues in response to consumer demand and has resulted in multiple poisonings.
Tetrodotoxin interferes with the transmission of signals from nerves to muscles by blocking sodium channels. This results in rapid weakening and paralysis of muscles, including those of the respiratory tract, which can lead to respiratory arrest and death. [2]
The toxic dose is not clear because puffer fish have different concentrations of tetrodotoxin. A dose of 1-2 mg of purified toxin can be lethal. Reported cases from the Centers for Disease Control and Prevention (CDC) have documented toxicity with ingestion of as little as 1.4 ounces of puffer fish.
Tetrodotoxin also is found in the the following:
-
Gastropod mollusc
-
The eggs of horseshoe crabs
-
Newts of the genus Taricha
-
The skin of Atelopid frogs
-
The skin and viscera of porcupine fish, globefish, balloon fish, blowfish, sunfish, toadfish, blue-ringed octopus, and some species of salamanders [3]
Detection of tetrodotoxins in European bivalve shellfish have been reported in the Netherlands, United Kingdom, France, Greece, and Italy, although concentrations were low in comparison to published minimum lethal doses for humans. [4, 5] In New Zealand, TTX was detected in approximately 30% of samples of shellfish. The concentrations were low except in pipi (Paphies australis), a surf clam endemic to New Zealand, where TTX was consistently detected in levels of 0.044 mg/kg or above. [6]
According to the CDC, to meet the clinical description for tedrotoxin poisoning, rapid onset of the following signs and symptoms are needed [7] :
-
Oral paresthesias (may progress to include the arms and legs)
-
Cranial nerve dysfunction
-
Weakness (may progress to paralysis)
-
Nausea or vomiting.
No known antidote exists. Providing the victim with respiratory support or mechanical ventilation until the toxin is excreted completely, or gastric lavage, are the only treatments for TTX intoxication that have been shown to reduce deaths. [8]
For patient education information, see Pufferfish Poisoning.
Pathophysiology
Puffer fish contain the potent neurotoxin tetrodotoxin. TTX is thought to be synthesized by a bacterial or dinoflagellate species associated with the puffer fish. [9, 8] The toxin is concentrated in the liver, gonads, and skin. The level of toxicity is seasonal, and, in Japan, fugu is served only from October through March.
TTX in terrestrial animals is limited to newts, toads and frogs. The origin of TTX in these animals is thought to be endogenous because this toxin has a role in defence. In particular, the levels of TTX in newts are higher in the skin than in the liver, leading to the theory that TTX is biosynthetically produced as a protection mechanism against predators. [8]
Tetrodotoxin is a heat-stable (except in alkaline environments) and water-soluble nonprotein.
It is a heterocyclic, small, organic molecule that acts directly on the electrically active sodium channel in nerve tissue (see the image below).
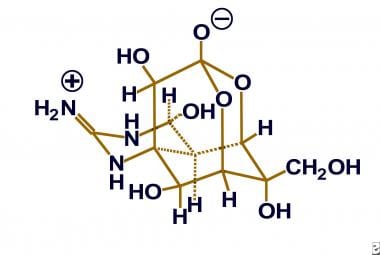
Tetrodotoxin blocks diffusion of sodium through the sodium channel, thus preventing depolarization and propagation of action potentials in nerve cells. All of the observed toxicity is secondary to blockade of the action potential. Tetrodotoxin acts on the central and the peripheral nervous systems (ie, autonomic, motor, sensory nerves).
Tetrodotoxin also stimulates the chemoreceptor trigger zone in the medulla oblongata and depresses the respiratory and vasomotor centers in that area.
TTX exerts analgesic properties by inhibiting the initiation and conduction of impulses in the peripheral nervous system. Clinical trials have been ongoing to evaluate the analgesic effect of TTX in cancer pain. [10] If tetrodotoxin begins to be used clinically, the incidence of toxicity may increase.
Etiology
Almost all toxicity is caused by the ingestion of fugu, but other species of animals have been shown to produce tetrodotoxin (eg, California newt, parrot fish, blue-ringed octopus). A death from ingestion of tetrodotoxin from a California newt has been documented.
Epidemiology
According to the 2019 Annual Report of the American Association of Poison Control Center National Poison Data System (AAPC-NPDS), 209 single exposures to tetrodotoxin were reported. [11] A 2014 report describes two patients in Minneapolis, Minnesota, who developed tetrodotoxin poisoning after consuming dried puffer fish purchased during a recent visit to New York City; the patients noted that two friends who consumed the same fish had similar but milder symptoms and had not sought care. [12]
Despite the careful training and certification of fugu chefs in Japan, cases of mortality and morbidity from puffer fish ingestion continue to be reported. Estimates vary, but up to 50 deaths may occur each year from tetrodotoxin poisoning in Japan. No known racial predilection exists. However, the poisoning is more common in Japanese people because of their dietary preferences for fugu.
Prognosis
Mortality rates are difficult to calculate, but estimates of mortality approach 50%, even with modern supportive medical care. Patients who live through the acute intoxication (ie, first 24 h) usually recover without residual deficits. Symptoms may last several days, even in nonlethal ingestions. The prognosis is generally good if the patient survives the first 24 hours. [2]
-
Puffer fish.
-
Chemical structure of tetrodotoxin.








