Practice Essentials
An anorectal abscess originates from an infection arising in the cryptoglandular epithelium lining the anal canal. The internal anal sphincter is believed to serve normally as a barrier to infection passing from the gut lumen to the deep perirectal tissues. This barrier can be breached through the crypts of Morgagni, which can penetrate through the internal sphincter into the intersphincteric space.
Once infection gains access to the intersphincteric space, it has easy access to the adjacent perirectal spaces. Extension of the infection can involve the intersphincteric space, ischiorectal space, or even the supralevator space. In some instances, the abscess remains contained within the intersphincteric space. The severity and depth of the abscess are quite variable, and the abscess cavity is often associated with formation of a fistulous tract. For that reason, fistulas are also discussed in this article where relevant.
The variety of anatomic sequelae of the primary infection is translated into variable clinical presentations. The relatively simple perianal abscess is to be distinguished from the more complex perirectal abscesses. Treatment also differs according to the type of abscess present.
Treatment of anorectal abscesses involves early surgical drainage of the purulent collection. Primary antibiotic therapy alone is ineffective in resolving the underlying infection and simply postpones surgical intervention. The ability to drain an anorectal abscess depends on patient comfort and on the location and accessibility of the abscess. When the abscess is perianal or superficial, drainage can usually be accomplished in the office or ED with local anesthesia.
For patient education resources, see the Esophagus, Stomach, and Intestine Center and the Digestive Disorders Center, as well as Anal Abscess, Rectal Pain, and Rectal Bleeding.
Anatomy
Normal anatomy demonstrates anywhere from four to 10 anal glands lying at the level of the dentate line, which divides the squamous epithelium distally and the columnar epithelium proximally. Obstruction of these anal glands by debris leads to stasis, bacterial overgrowth, and abscess formation that extends into the intersphincteric groove between the internal and external anal sphincters. [1] From this space, the abscess can spread along various potential spaces.
Anorectal abscesses are classified according to their anatomic location; the following are the most common locations (see the image below):
-
Perianal
-
Ischiorectal
-
Intersphincteric
-
Supralevator
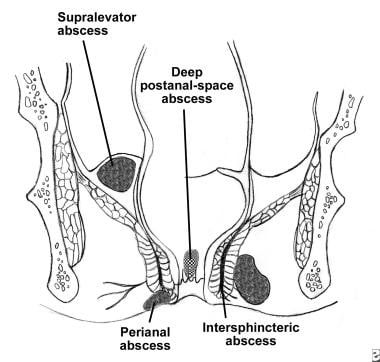 Illustration of major types of anorectal abscesses (submucosal type not pictured).
Illustration of major types of anorectal abscesses (submucosal type not pictured).
Perianal abscesses represent the most common type of anorectal abscesses, accounting for approximately 60% of reported cases. [1, 2, 3, 4] These superficial collections of purulent material are located beneath the skin of the anal canal and do not transverse the external sphincter.
Ischiorectal abscesses are the next most common type. These abscesses form when suppuration transverses the external anal sphincter into the ischiorectal space. An ischiorectal abscess may traverse the deep postanal space into the contralateral side, forming a so-called horseshoe abscess.
Intersphincteric abscesses, the third most common type, result from suppuration contained between the internal and external anal sphincters. They may lie completely within the anal canal, leading to severe pain, and may only be found by digital rectal examination or anoscopy.
Supralevator abscesses, the least common of the four major types, may form from cephalad extension of the intersphincteric abscess above the levator ani or from caudal extension of a suppurative abdominal process (eg, appendicitis, diverticular disease, gynecologic sepsis) into the supralevator space. These abscesses may be diagnosed by means of computed tomography (CT), and they cause pelvic and rectal pain.
According to the widely used Parks classification system, anorectal fistulas may also be classified into four major types, as follows [5] :
-
Intersphincteric (70%) - Found between the internal and external sphincters
-
Transsphincteric (23%) - Extends through the external sphincter into the ischiorectal fossa
-
Extrasphincteric (5%) - Passes from the rectum to the skin through the levator ani
-
Suprasphincteric (2%) - Extends from the intersphincteric plane through the puborectalis, exiting the skin after traversing the levator ani
The characteristics of perianal fistulas vary according to their anatomic location. According to the Goodsall rule, the external opening of a fistulous tract located anterior to a transverse line drawn across the anal verge is associated with a straight radial tract of the fistula into the anal canal/rectum, whereas an external opening posterior to the transverse line follows a curved, fistulous tract to the posterior midline of the rectal lumen (see the image below). This rule is important for planning surgical treatment of the fistula (see Treatment).
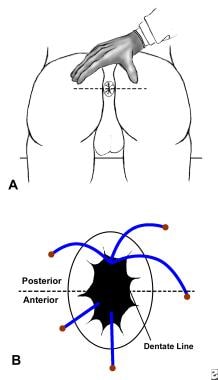 Goodsall rule for anorectal fistulas. Fistulas that exit in posterior half of rectum generally follow curved course toward posterior midline, whereas those that exit in anterior half of rectum usually follow radial course to dentate line.
Goodsall rule for anorectal fistulas. Fistulas that exit in posterior half of rectum generally follow curved course toward posterior midline, whereas those that exit in anterior half of rectum usually follow radial course to dentate line.
Pathophysiology
Perirectal abscesses and fistulas represent anorectal disorders arising predominantly (~90% of cases) from the obstruction of anal crypts, [4] possibly involving increased sphincter tone. [6] Infection of the now static glandular secretions results in suppuration and abscess formation within the anal gland. Typically, the abscess forms initially in the intersphincteric space and then spreads along adjacent potential spaces.
Etiology
Both aerobic and anaerobic bacteria have been found to be responsible for abscess formation. The anaerobes most commonly implicated are Bacteroides fragilis, Peptostreptococcus, Prevotella, Fusobacterium, Porphyromonas, and Clostridium. The aerobes most commonly implicated are Staphylococcus aureus, Streptococcus, and Escherichia coli. [7] More recent studies have noted community-acquired methicillin-resistant S aureus (MRSA) as a pathogen leading to abscess formation. [8, 9]
Approximately 10% of anorectal abscesses may be caused by reasons other than anal gland infection, including Crohn disease, trauma, immunodeficiency resulting from HIV infection or malignancy (both hematologic and anorectal cancer), tuberculosis, hidradenitis suppurativa, sexually transmitted diseases, radiation therapy, foreign bodies, perforated diverticular disease, inflammatory bowel disease, or appendicitis (a rare cause of supralevator abscesses). [1]
Epidemiology
United States and international statistics
Approximately 30% of patients with anorectal abscesses report a previous history of similar abscesses that either resolved spontaneously or required surgical intervention.
The incidence of abscess formation appears to be higher in spring and summer. Whereas demographics point to a clear disparity in the occurrence of anal abscesses with respect to age and sex, no obvious pattern exists among various countries or regions of the world. Although it has been suggested that there is a direct relation between the formation of anorectal abscesses and bowel habits, frequent diarrhea, and poor personal hygiene, this relation remains unproven.
Age- and sex-related demographics
The peak incidence of anorectal abscesses is in the third and fourth decades of life. [10] These abscesses are also quite common in infants (see Anorectal Abscesses in Children). The exact mechanism is poorly understood but does not appear to be related to constipation. Fortunately, this condition is quite benign in infants, rarely necessitating any operative intervention other than simple drainage. [11]
Men are affected more frequently than women are, with a male-to-female predominance of 2:1 to 3:1. [10]
Prognosis
Overall mortality from anorectal abscesses is quite low. [2]
Early data indicated that abscess formation recurred in approximately 10% of patients, with chronic fistula-in-ano occurring in as many 50% of patients. [1, 2, 12] A later study found that 37% of patients developed chronic anal fistula or recurrent sepsis. [6] In this study, risk factors were age younger than 40 years and nondiabetic status; no difference in these complications was noted with regard to HIV status, sex, antibiotic usage, or smoking status.
Approximately two thirds of patients with rectal abscesses who are treated by incision and drainage or by spontaneous drainage will develop a chronic anal fistula. After fistula formation, multiple complications may develop after surgery. As many as 43% of patients may experience fecal incontinence after surgical repair for complex fistula-in-ano. [13] Other postoperative complications include temporary postejaculation urethral irritation and postoperative urinary retention. [14] Constipation may also occur as a result of pain on defecation.
The recurrence rate of anorectal fistulas after fistulotomy, fistulectomy, or the use of a seton is about 1.5%. The success rate of primary surgical treatment with fistulotomy appears to be fairly good. [15]
-
Illustration of major types of anorectal abscesses (submucosal type not pictured).
-
Goodsall rule for anorectal fistulas. Fistulas that exit in posterior half of rectum generally follow curved course toward posterior midline, whereas those that exit in anterior half of rectum usually follow radial course to dentate line.
-
Goodsall rule for anorectal fistulas. Note curved nature of posterior fistulas and radial (straight) orientation of anterior fistulas.






