Practice Essentials
Pneumothorax is defined as the presence of air or gas in the pleural cavity (ie, the potential space between the visceral and parietal pleura of the lung), which can impair oxygenation and/or ventilation. The clinical results are dependent on the degree of collapse of the lung on the affected side. If the pneumothorax is significant, it can cause a shift of the mediastinum and compromise hemodynamic stability. Air can enter the intrapleural space through a communication from the chest wall (ie, trauma) or through the lung parenchyma across the visceral pleura. See the image below.

Signs and symptoms
The presentation of patients with pneumothorax varies depending on the following types of pneumothorax and ranges from completely asymptomatic to life-threatening respiratory distress:
-
Spontaneous pneumothorax: No clinical signs or symptoms in primary spontaneous pneumothorax until a bleb ruptures and causes pneumothorax; typically, the result is acute onset of chest pain and shortness of breath, particularly with secondary spontaneous pneumothoraces
-
Iatrogenic pneumothorax: Symptoms similar to those of spontaneous pneumothorax, depending on patient’s age, presence of underlying lung disease, and extent of pneumothorax
-
Tension pneumothorax: Hypotension, hypoxia, chest pain, dyspnea
-
Catamenial pneumothorax: Women aged 30-40 years with onset of symptoms within 48 hours of menstruation, right-sided pneumothorax, and recurrence
-
Pneumomediastinum: Must be differentiated from spontaneous pneumothorax; patients may or may not have symptoms of chest pain, persistent cough, sore throat, dysphagia, shortness of breath, or nausea/vomiting
See Clinical Presentation for more detail.
Diagnosis
History and physical examination remain the keys to making the diagnosis of pneumothorax. Examination of patients with this condition may reveal diaphoresis and cyanosis (in the case of tension pneumothorax). Affected patients may also reveal altered mental status changes, including decreased alertness and/or consciousness (a rare finding).
Findings on lung auscultation vary depending on the extent of the pneumothorax. Respiratory findings may include the following:
-
Respiratory distress (considered a universal finding) or respiratory arrest
-
Tachypnea (or bradypnea as a preterminal event)
-
Asymmetric lung expansion: Mediastinal and tracheal shift to contralateral side (large tension pneumothorax)
-
Distant or absent breath sounds: Unilaterally decreased/absent lung sounds common, but decreased air entry may be absent even in advanced state of pneumothorax
-
Minimal lung sounds transmitted from unaffected hemithorax with auscultation at midaxillary line
-
Hyperresonance on percussion: Rare finding; may be absent even in an advanced state
-
Decreased tactile fremitus
-
Adventitious lung sounds: Ipsilateral crackles, wheezes
Cardiovascular findings may include the following:
-
Tachycardia: Most common finding; if heart rate is faster than 135 beats/min, tension pneumothorax likely
-
Pulsus paradoxus
-
Hypotension: Inconsistently present finding; although typically considered a key sign of tension pneumothorax, hypotension can be delayed until its appearance immediately precedes cardiovascular collapse
-
Jugular venous distention: Generally seen in tension pneumothorax; may be absent if hypotension is severe
-
Cardiac apical displacement: Rare finding
Common findings among the types of pneumothoraces include the following:
-
Spontaneous and iatrogenic pneumothorax: Tachycardia most common finding; tachypnea and hypoxia may be present
-
Tension pneumothorax: Variable findings; respiratory distress and chest pain; tachycardia; ipsilateral air entry on auscultation; breath sounds absent on affected hemithorax; trachea may deviate from affected side; thorax may be hyperresonant; jugular venous distention and/or abdominal distention may be present
-
Pneumomediastinum: Variable or absent findings; subcutaneous emphysema is the most consistent sign; Hamman sign—a precordial crunching noise synchronous with the heartbeat and often accentuated during expiration—has a variable rate of occurrence, with one series reporting 10%
Lab and imaging studies
Although laboratory and imaging studies help determine a diagnosis, tension pneumothorax primarily is a clinical diagnosis based on patient presentation. Suspicion of tension pneumothorax, especially in late stages, mandates immediate treatment and does not require potentially prolonged diagnostic studies.
Arterial blood gas (ABG) studies measure the degrees of acidemia, hypercarbia, and hypoxemia, the occurrence of which depends on the extent of cardiopulmonary compromise at the time of collection. ABG analysis does not replace physical diagnosis, nor should treatment be delayed while awaiting results if symptomatic pneumothorax is suspected. However, ABG analysis may be useful in evaluating hypoxia and hypercarbia and respiratory acidosis.
When pneumothorax is suspected, confirmation by chest radiography affords additional information beyond confirmation, such as the extent of pneumothorax, potential causes, a baseline study from which to go forward, and assistance with the therapeutic plan.
The following radiologic studies may be used to evaluate suspected pneumothorax:
-
Chest radiography: Anteroposterior and/or lateral decubitus films
-
Contrast-enhanced esophagography: If emesis/retching is the precipitating event
-
Chest computed tomography scanning: Most reliable imaging study for diagnosis of pneumothorax but not recommended for routine use in pneumothorax
-
Chest ultrasonography
See Workup for more detail.
Management
Although there is general agreement on the management of pneumothorax, a full consensus about management of initial or recurrent pneumothorax does not exist. Rather, many clinicians use a risk stratification framework as well as other approaches for choosing among options to restore lung volume and an air-free pleural space and to prevent recurrences. [1]
The range of medical therapeutic options for pneumothorax includes the following:
-
Watchful waiting, with or without supplemental oxygen
-
Simple aspiration
-
Tube drainage, with or without medical pleurodesis
Surgery
If the patient has had repeated episodes of pneumothorax or if the lung remains unexpanded after 5 days with a chest tube in place, operative therapy such as the following may be necessary:
-
Thoracoscopy: Video-assisted thoracoscopic surgery (VATS)
-
Electrocautery: Pleurodesis or sclerotherapy
-
Laser treatment
-
Resection of blebs or pleura
-
Open thoracotomy
Pharmacotherapy
The following medications may be used to aid in the management of patients with pneumothorax:
-
Local anesthetics (eg, lidocaine hydrochloride)
-
Opioid anesthetics (eg, fentanyl citrate, morphine)
-
Benzodiazepines (eg, midazolam, lorazepam)
-
Antibiotics (eg, doxycycline, cefazolin)
See Treatment and Medication for more detail.
Background
Pneumothorax is defined as the presence of air or gas in the pleural cavity (ie, the potential space between the visceral and parietal pleura of the lung). The clinical results are dependent on the degree of collapse of the lung on the affected side. Pneumothorax can impair oxygenation and/or ventilation. If the pneumothorax is significant, it can cause a shift of the mediastinum and compromise hemodynamic stability. Air can enter the intrapleural space through a communication from the chest wall (ie, trauma) or through the lung parenchyma across the visceral pleura.
Among the topics this article will discuss are several areas of new information in the medical literature: (1) studies comparing aspiration and tube drainage for treatment of primary spontaneous pneumothorax (PSP), (2) long-term follow-up of surgical treatment of pneumothorax, (3) assessment of the impact of pleurodesis on transplantation outcomes in patients with lymphangiomyomatosis, (4) demonstrated utility of ultrasonography (US) in the bedside diagnosis of iatrogenic pneumothorax, and (5) inability of US to distinguish between intrapulmonary bullae and pneumothorax.
See also Restoring an Air-Free Pleural Space in Pneumothorax.
Primary and secondary spontaneous pneumothorax
Spontaneous pneumothorax is a commonly encountered problem with approaches to treatment that vary from observation to aggressive intervention. [2, 3] PSP occurs in people without underlying lung disease and in the absence of an inciting event (see the images below). [4] Air enters into the intrapleural space without preceding trauma and without an underlying history of clinical lung disease. However, many patients whose condition is labeled as PSP have subclinical lung disease (eg, pleural blebs) that can be detected with computed tomography (CT). Patients are typically aged 18-40 years, tall, and thin; often, they are smokers.

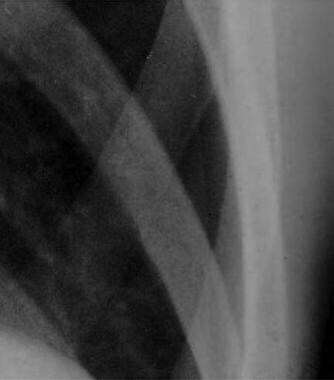 Close radiographic view of patient with small spontaneous primary pneumothorax (same patient as in previous image).
Close radiographic view of patient with small spontaneous primary pneumothorax (same patient as in previous image).
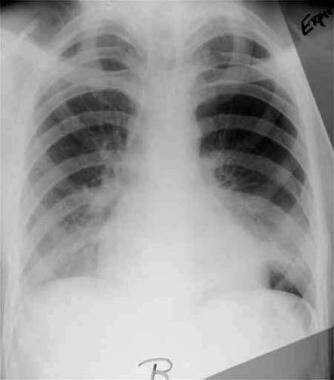 Expiratory radiograph of patient with small spontaneous primary pneumothorax (same patient as in previous images).
Expiratory radiograph of patient with small spontaneous primary pneumothorax (same patient as in previous images).
Secondary spontaneous pneumothorax (SSP) occurs in people with a wide variety of parenchymal lung diseases. [4] These individuals have underlying pulmonary pathology that alters normal lung structure (see the image below). Air enters the pleural space via distended, damaged, or compromised alveoli. The presentation of these patients may include more serious clinical symptoms and sequelae due to comorbid conditions.
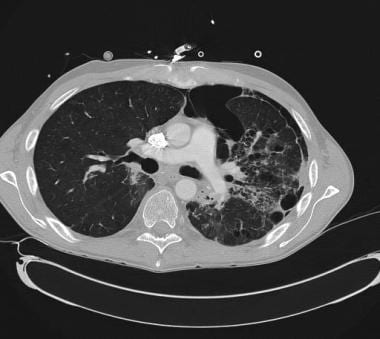 CT scan demonstrating secondary spontaneous pneumothorax (SSP) from radiation/chemotherapy for lymphoma.
CT scan demonstrating secondary spontaneous pneumothorax (SSP) from radiation/chemotherapy for lymphoma.
Iatrogenic and traumatic pneumothorax
Iatrogenic pneumothorax is a traumatic pneumothorax that results from injury to the pleura, with air introduced into the pleural space secondary to diagnostic or therapeutic medical intervention (see the following image). Half a century ago, iatrogenic pneumothorax was predominantly the result of deliberate injection of air into the pleural space for the treatment of tuberculosis (TB). The terminology evolved to the preference for "induced" or "artificial" pneumothorax to indicate pulmonary TB treatment, before arriving at the current classification. Pulmonary TB remains a significant cause of secondary pneumothorax.
 Radiograph of older man who was admitted to ICU postoperatively. Note right-side pneumothorax induced by incorrectly positioned small-bowel feeding tube in right-side bronchial tree. Marked depression of right hemidiaphragm is noted, and mediastinal shift is to left, suggestive of tension pneumothorax. Endotracheal tube is in good position.
Radiograph of older man who was admitted to ICU postoperatively. Note right-side pneumothorax induced by incorrectly positioned small-bowel feeding tube in right-side bronchial tree. Marked depression of right hemidiaphragm is noted, and mediastinal shift is to left, suggestive of tension pneumothorax. Endotracheal tube is in good position.
Traumatic pneumothorax results from blunt trauma or penetrating trauma that disrupts the parietal or visceral pleura (see the images below). Management steps for traumatic pneumothoraces are similar to those for other, nontraumatic causes. If hemodynamic or respiratory status is compromised or an open (communicating to the atmosphere) and/or hemothorax are also present, tube thoracostomy is performed to evacuate air and allow reexpansion of the lung. There is a subset of traumatic pneumothoraces classified as occult; that is, they cannot be seen on chest radiographs but can be seen on CT scans. In general, these can be observed and treated if they become symptomatic.
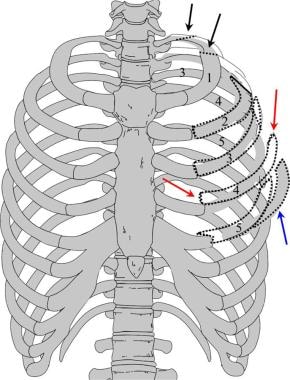 Illustration depicting multiple fractures of left upper chest wall. First rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along midlateral (red arrows) or anterior chest wall (blue arrows), flail chest (dotted black lines) may result, which may result in pneumothorax.
Illustration depicting multiple fractures of left upper chest wall. First rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along midlateral (red arrows) or anterior chest wall (blue arrows), flail chest (dotted black lines) may result, which may result in pneumothorax.
Tension pneumothorax
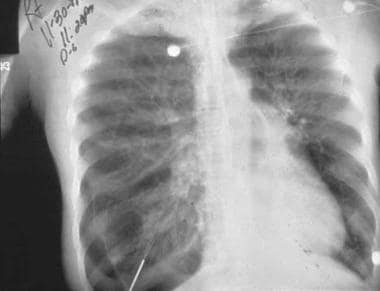
Tension pneumothorax is a life-threatening condition that develops when air is trapped in the pleural cavity under positive pressure, displacing mediastinal structures and compromising cardiopulmonary function. Prompt recognition is life-saving, both outside the hospital and in a modern intensive care unit (ICU). Because tension pneumothorax occurs infrequently and has a potentially devastating outcome, a high index of suspicion and knowledge of basic emergency thoracic decompression procedures are important for all healthcare personnel. Immediate decompression of the thorax is mandatory when tension pneumothorax is suspected and should not be delayed for radiographic confirmation. (See the image below.)
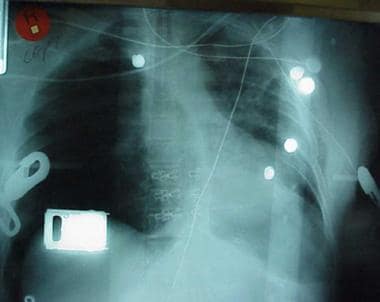 Chest radiograph shows two abnormalities: (1) tension pneumothorax and (2) potentially life-saving intervention delayed during wait for x-ray results. Tension pneumothorax is clinical diagnosis requiring emergency needle decompression, and therapy should never be delayed for x-ray confirmation.
Chest radiograph shows two abnormalities: (1) tension pneumothorax and (2) potentially life-saving intervention delayed during wait for x-ray results. Tension pneumothorax is clinical diagnosis requiring emergency needle decompression, and therapy should never be delayed for x-ray confirmation.
Pneumomediastinum
Pneumomediastinum is the presence of gas in the mediastinal tissues occurring spontaneously or following procedures or trauma (see the following images). A pneumothorax may occur secondary to pneumomediastinum.
 Pneumomediastinum from barotrauma may result in tension pneumothorax and obstructive shock.
Pneumomediastinum from barotrauma may result in tension pneumothorax and obstructive shock.
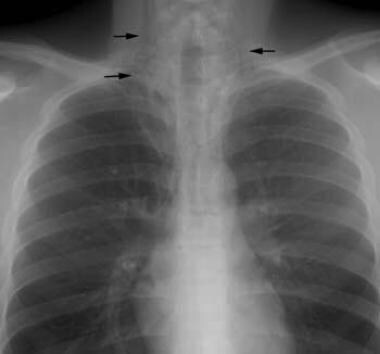
 Chest radiograph shows pneumomediastinum (radiolucency noted around left heart border) in patient who had respiratory and circulatory arrest in emergency department after experiencing multiple episodes of vomiting and rigid abdomen. Patient was taken immediately to operating room, where large rupture of esophagus was repaired.
Chest radiograph shows pneumomediastinum (radiolucency noted around left heart border) in patient who had respiratory and circulatory arrest in emergency department after experiencing multiple episodes of vomiting and rigid abdomen. Patient was taken immediately to operating room, where large rupture of esophagus was repaired.
Anatomy
The inner surface of the thoracic cage (parietal pleura) is contiguous with the outer surface of the lung (visceral pleura); this space contains a small amount of lubricating fluid and is normally under negative pressure compared to the alveoli. Determinants of pleural pressure are the opposing recoil forces of the lung and chest wall.
Pathophysiology
Spontaneous pneumothorax
Spontaneous pneumothorax in most patients occurs from the rupture of blebs and bullae. Although PSP is defined as occurring in patients without underlying pulmonary disease, these patients have asymptomatic blebs and bullae detected on CT scans or during thoracotomy. PSP is typically observed in tall, young people without parenchymal lung disease and is thought to be related to increased shear forces in the apex.
Although PSP is associated with the presence of apical pleural blebs, the exact anatomic site of air leakage is often uncertain. Fluorescein-enhanced autofluorescence thoracoscopy (FEAT) is a newer method of examining the site of air leak in PSP. FEAT-positive lesions can be detected that appear normal when viewed under normal white-light thoracoscopy. [5]
In normal respiration, the pleural space has a negative pressure. As the chest wall expands outward, the surface tension between the parietal and visceral pleura expands the lung outward. The lung tissue intrinsically has an elastic recoil, tending to collapse inwards. If the pleural space is invaded by gas from a ruptured bleb, the lung collapses until equilibrium is achieved or the rupture is sealed. As the pneumothorax enlarges, the lung becomes smaller. The main physiologic consequence of this process is a decrease in vital capacity and partial pressure of oxygen.
Lung inflammation and oxidative stress are hypothesized to be important to the pathogenesis of PSP. [6] Current smokers, at increased risk for PSP, have increased numbers of inflammatory cells in the small airways. Bronchoalveolar lavage (BAL) studies in patients with PSP reveal that the degree of inflammation correlates with the extent of emphysematouslike changes (ELCs). One hypothesis is that ELCs result from degradation of lung tissue due to imbalances of enzymes and antioxidants released by innate immune cells. [7] In one study, erythrocyte superoxide dismutase activity was significantly lower and plasma malondialdehyde levels higher in patients with PSP than in normal control subjects. [6]
A growing body of evidence suggests that genetic factors may be important in the pathogenesis of many cases of PSP. Familial clustering of this condition has been reported. Genetic disorders that have been linked to PSP include Marfan syndrome, homocystinuria, and Birt-Hogg-Dube (BHD) syndrome.
BHD syndrome is an autosomal dominant disorder that is characterized by benign skin tumors (hair follicle hamartomas), renal and colon cancer, and spontaneous pneumothorax. Spontaneous pneumothorax occurs in about 22% of patients with this syndrome. The gene responsible is a tumor suppressor gene located on band 17p11.2. The gene encoding folliculin (FLCN) is thought to be the cause. Multiple mutations have been found, and phenotypic variation is recognized. In one study, eight patients without skin or renal involvement had lung cysts and spontaneous pneumothorax. [8] A germline mutation to this gene has been found in five patients, and genetic testing is now available.
Tension pneumothorax
Tension pneumothorax occurs anytime a disruption involves the visceral pleura, parietal pleura, or the tracheobronchial tree. This condition develops when injured tissue forms a one-way valve, allowing air inflow with inhalation into the pleural space and prohibiting air outflow. The volume of this nonabsorbable intrapleural air increases with each inspiration because of the one-way valve effect. As a result, pressure rises within the affected hemithorax. In addition to this mechanism, the positive pressure used with mechanical ventilation can cause air trapping.
As pressure increases, the ipsilateral lung collapses and causes hypoxia. Further pressure increases cause the mediastinum to shift toward the contralateral side, impinging on and compressing the contralateral lung and impairing venous return to the right atrium. Hypoxia results as the collapsed lung on the affected side and the compressed lung on the contralateral side compromise gas exchange. This hypoxia and decreased venous return caused by compression of the relatively thin walls of the atria impair cardiac function. Kinking of the inferior vena cava is thought to be the initial event restricting blood to the heart. It is most evident in trauma patients who are hypovolemic with reduced venous blood return.
Arising from numerous causes, this condition rapidly progresses to respiratory insufficiency, cardiovascular collapse, and, ultimately, death if unrecognized and untreated.
Pneumomediastinum
With pneumomediastinum, excessive intra-alveolar pressures lead to rupture of alveoli bordering the mediastinum. Air escapes into the surrounding connective tissue and dissects further into the mediastinum. Esophageal trauma or elevated airway pressures may also allow air to dissect into the mediastinum. Air may then travel superiorly into the visceral, retropharyngeal, and subcutaneous spaces of the neck. From the neck, the subcutaneous compartment is continuous throughout the body; thus, air can diffuse widely.
Mediastinal air can also pass inferiorly into the retroperitoneum and other extraperitoneal compartments. If the mediastinal pressure rises abruptly or if decompression is not sufficient, the mediastinal parietal pleura may rupture and cause a pneumothorax (in 10-18% of patients).
A wide variety of disease states and circumstances may result in a pneumothorax.
Primary and secondary spontaneous pneumothorax
Risks factors for PSP include the following:
-
Smoking
-
Tall, thin stature in a healthy person
-
Marfan syndrome
-
Pregnancy
-
Familial pneumothorax
Blebs and bullae (sometimes referred to as ELCs) are related to the occurrence of PSP. Thoracic CT scans of patients with PSP shows ipsilateral ELC in 89% and contralateral changes in 80%, compared with a rate of 20% among control subjects matched for age and smoking. [4] Nonsmokers with PSP had CT scan ELC abnormalities of 80% compared with a rate of 0% among nonsmoker controls without PSP. [4]
Although patients with PSP do not have overt parenchymal disease, this condition is heavily associated with smoking—80-90% of PSP cases occur in smokers or former smokers, and the relative risk of PSP increases as the number of cigarettes smoked per day increases; that is, the risk of PSP is related to the intensity of smoking, with 102 times higher incidence rates in males who smoke heavily (ie, >22 cigarettes/d), compared with a sevenfold increase in males who smoke lightly (1-12 cigarettes/d). This incremental risk with increasing number of cigarettes smoked per day is much more pronounced in female smokers.
Typical PSP patients also tend to have a tall and thin body habitus. Whether height affects development of subpleural blebs or whether more negative apical pleural pressures cause preexisting blebs to rupture is unclear.
Pregnancy is an unrecognized risk factor, as suggested by a 10-year retrospective series in which five of 250 spontaneous pneumothorax cases were in pregnant women. [9] The cases were all managed successfully with simple aspiration or video-assisted thoracoscopic surgery (VATS), and no harm occurred to mother or fetus. [9]
Other associations with pneumothorax include increased intrathoracic pressure with the Valsalva maneuver, though contrary to popular belief, most spontaneous pneumothoraces occur while the patient is at rest. Changes in atmospheric pressure, proximity to loud music, and low-frequency noises are other reported factors.
Familial associations have been noted in more than 10% of patients. Some are due to rare connective tissue diseases, but mutations in the gene encoding folliculin (FLCN) have been described. These patients may represent an incomplete penetrance of an autosomal dominant genetic disorder. BHD syndrome is characterized by benign skin growths, pulmonary cysts, and renal cancers and is caused by mutations in the FLCN gene.
In one family study, nine ascertained cases of spontaneous pneumothorax were reported among 54 members. A review of the literature summarized 61 reports of familial spontaneous pneumothorax among 22 families. Up to 10% patients with spontaneous pneumothorax report a positive family history. [10]
Although rare, spontaneous pneumothorax occurring bilaterally and progressing to tension pneumothorax has been documented.
Diseases and conditions associated with SSP include the following:
-
Chronic obstructive pulmonary disease (COPD) or emphysema - Increased pulmonary pressure due to coughing with a bronchial plug of mucus or phlegm bronchial plug may play a role.
-
Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) with PCP infection
-
Necrotizing pneumonia
-
Bronchogenic carcinoma or metastatic malignancy
-
Inhalational and intravenous drug use (eg, marijuana, cocaine) [11]
-
Interstitial lung diseases associated with connective tissue diseases
-
Lymphangioleiomyomatosis (LAM)
-
Severe acute respiratory syndrome (SARS) - A reported 1.7% of SARS patients developed spontaneous pneumothorax. [12]
-
Thoracic endometriosis and catamenial pneumothorax
-
Collagen vascular disease, including Marfan syndrome
SSPs occur in the presence of lung disease, primarily in the presence of COPD. Other diseases that may be present when SSPs occur include tuberculosis, sarcoidosis, cystic fibrosis, malignancy, and idiopathic pulmonary fibrosis.
Pneumocystis jiroveci pneumonia (previously known as Pneumocystis carinii pneumonia [PCP]) was a common cause of SSP in patients with AIDS during the last decade. In fact, 77% of AIDS patients with spontaneous pneumothorax had thin-walled cavities, cysts, and pneumothorax from PCP infection. [13] With the advent of highly active antiretroviral therapy (HAART) and widespread use of trimethoprim-sulfamethoxazole (TMP-SMZ) prophylaxis, the incidence of PCP and associated SSP has significantly declined.
PCP in other immunocompromised patients is seen only when TMP-SMZ prophylaxis is withdrawn prematurely. For practical purposes, if the immunocompromised patient has been taking TMP-SMZ prophylaxis reliably, PCP is reasonably excluded from the differential diagnosis and should not be a causative factor for SSP.
In cystic fibrosis, up to 18.9% of patients have been reported to develop spontaneous pneumothoraces, and they have a high incidence of recurrence on the same side after conservative management (50%) or intercostal drainage (55.2%). The risk of SSP in these patients increases with Burkholderia cepacia or Pseudomonas infections and allergic bronchopulmonary aspergillosis (ABPA). [14] Pleurodesis increases the risk of bleeding associated with lung transplantation but is not an absolute contraindication.
Many different types of malignancies are known to present with a pneumothorax, especially sarcomas, but also genitourinary cancers and primary lung cancer; thus, pneumothorax in a patient with malignancy should prompt a look for metastatic disease. Chemotherapeutic agents, at times, can also induce SSP. [15]
Interstitial lung diseases are associated with connective-tissue diseases. Ankylosing spondylitis may be noted when apical fibrosis is present; in fact, the typically low incidence of spontaneous pneumothorax in patients with ankylosing spondylitis (0.29%) increases 45-fold (to 13%) when apical fibrotic disease exists. [16]
LAM may present with spontaneous pneumothorax. This disease is characterized by thin-walled cysts in women of childbearing age. Respiratory failure may lead to a need for lung transplantation, and previous pleurodesis is no longer an absolute contraindication for lung transplantation.
Thoracic endometriosis is a rare cause of recurrent pneumothorax (catamenial pneumothorax) in women that is thought to arise from endometriosis reaching the chest wall across the diaphragm (ie, its etiology may be primarily related to associated diaphragmatic defects). In a case series of 229 patients, catamenial pneumothorax caused by thoracic endometriosis was localized to the visceral pleura in 52% of patients and to the diaphragm in 39% of patients. [17] Before recurrence, this condition may be initially diagnosed as PSP.
Iatrogenic and traumatic pneumothorax
Causes of iatrogenic pneumothorax include the following:
-
Transthoracic needle aspiration biopsy of pulmonary nodules (most common cause: 32-37% of cases)
-
Transbronchial or pleural biopsy
-
Thoracentesis
-
Central venous catheter (CVC) insertion, usually subclavian or internal jugular [18]
-
Intercostal nerve block
-
Tracheostomy
-
Cardiopulmonary resuscitation (CPR) - Consider the possibility of a pneumothorax if ventilation becomes progressively more difficult.
-
Acute respiratory distress syndrome ( ARDS) and positive-pressure ventilation in the ICU - High peak airway pressures can translate into barotrauma in up to 3% of patients on a ventilator and up to 5% of patients with ARDS. [19]
-
Nasogastric feeding tube placement
Iatrogenic pneumothorax is a complication of medical or surgical procedures. It most commonly results from transthoracic needle aspiration. Other procedures commonly causing iatrogenic pneumothorax are therapeutic thoracentesis, pleural biopsy, CVC insertion, transbronchial biopsy, positive-pressure ventilation (PPV), and inadvertent intubation of the right mainstem bronchus. Therapeutic thoracentesis is complicated by pneumothorax 30% of the time when performed by inexperienced operators, in contrast to only 4% of the time when performed by experienced clinicians.
The routine use of US during diagnostic thoracentesis is associated with lower rates of pneumothorax (4.9% vs 10.3%) and need for tube thoracostomy (0.7% vs 4.1%). Similarly, in patients who are mechanically ventilated, thoracocentesis guided by bedside US without radiology support results in a relatively lower rate of pneumothorax.
Causes of traumatic pneumothorax include the following:
-
Trauma - Penetrating and nonpenetrating injury
-
Rib fracture
-
High-risk occupation (eg, diving, flying)
Traumatic pneumothoraces can result from both penetrating and nonpenetrating lung injuries. Complications include hemopneumothorax and bronchopleural fistula. Traumatic pneumothoraces often can create a one-way valve in the pleural space (only letting in air without escape) and can lead to a tension pneumothorax.
Tension pneumothorax
The most common etiologies of tension pneumothorax are either iatrogenic or related to trauma, such as the following:
-
Blunt or penetrating trauma - Disruption of either the visceral or parietal pleura occurs and is often associated with rib fractures, though rib fractures are not necessary for tension pneumothorax to occur.
-
Barotrauma secondary to PPV, especially when high amounts of positive end-expiratory pressure (PEEP) are used
-
Fiberoptic bronchoscopy with closed lung biopsy [22]
-
Markedly displaced thoracic spine fractures
-
Preexisting Bochdalek hernia with trauma [26]
-
Colonoscopy [27] and gastroscopy have been implicated in case reports.
-
Percutaneous tracheostomy [28]
-
Conversion of idiopathic, spontaneous, simple pneumothorax to tension pneumothorax
-
Unsuccessful attempts to convert an open pneumothorax to a simple pneumothorax in which the occlusive dressing functions as a one-way valve
Tension pneumothorax occurs commonly in the ICU setting in patients who are receiving PPV, and practitioners must always consider this when changes in respiratory or hemodynamic status occur. Infants requiring ventilatory assistance and those with meconium aspiration have a particularly high risk for tension pneumothorax. Aspirated meconium may serve as a one-way valve and produce a tension pneumothorax.
Any penetrating wound that produces an abnormal passageway for gas exchange into the pleural spaces and that results in air trapping may produce a tension pneumothorax. Blunt trauma, with or without associated rib fractures, and incidents such as unrestrained head-on motor vehicle accidents, falls, and altercations involving laterally directed blows may also cause tension pneumothoraces.
Significant chest injuries carry an estimated 10-50% risk of associated pneumothorax; in about 50% of these cases, the pneumothorax may not be seen on standard radiographs and are therefore deemed occult. In one study, 12% of patients with asymptomatic chest stab wounds had a delayed pneumothorax or hemothorax. McPherson et al analyzed data from the Vietnam Wound Data and Munitions Effectiveness Team study and determined that tension pneumothorax was the cause of death in 3-4% of fatally wounded combat casualties. [29]
Acupuncture is a traditional Chinese medicine technique used worldwide by alternative medical practitioners. Acupuncture's most frequently reported serious complication is pneumothorax; in one Japanese report of 55,291 acupuncture treatments, an approximate incidence of 1 pneumothorax in 5000 cases was documented. [30]
Pneumomediastinum
The following factors may result in pneumomediastinum:
-
Acute generation of high intrathoracic pressures (often as a result of inhalational drug use, such smoking marijuana or inhalation of cocaine)
-
Asthma
-
Respiratory tract infection
-
Parturition
-
Emesis
-
Severe cough
-
Mechanical ventilation
-
Trauma or surgical disruption of the oropharyngeal, esophageal, or respiratory mucosa
-
Athletic competition
Epidemiology
Primary, secondary, and recurring spontaneous pneumothorax
It is likely that the incidence for spontaneous pneumothorax is underestimated. Up to 10% of patients may be asymptomatic, and others with mild symptoms may not present to a medical provider.
PSP occurs in people aged 20-30 years, with a peak incidence is in the early 20s; it is rarely observed in people older than 40 years. The age-adjusted incidence of PSP is 7.4-18 cases per 100,000 persons per year for men and 1.2-6 cases per 100,000 persons per year for women. [31] The male-to-female ratio of age-adjusted rates is 6.2:1.
SSPs occur more frequently in patients aged 60-65 years. The age-adjusted incidence of SSP is 6.3 cases per 100,000 persons per year for men and 2.0 cases per 100,000 persons per year for women. The male-to-female ratio of age-adjusted rates is 3.2:1. COPD is a common cause of secondary spontaneous pneumothorax that carries an incidence of 26 cases per 100,000 persons. [32]
Smoking increases the risk of a first spontaneous pneumothorax by more than 20-fold in men and by nearly 10-fold in women compared with risks in nonsmokers. [33] Increased risk of pneumothorax and recurrence appears to rise proportionally with number of cigarettes smoked.
In men, the risk of spontaneous pneumothorax is 102 times higher in heavy smokers than in nonsmokers. Spontaneous pneumothorax most frequently occurs in tall, thin men aged 20-40 years.
Iatrogenic and traumatic pneumothorax
Traumatic and tension pneumothoraces occur more frequently than spontaneous pneumothoraces, and the rate is undoubtedly increasing in United States hospitals as intensive care treatment modalities have become increasingly dependent on PPV, CVC placement, and other causes that potentially induce iatrogenic pneumothorax.
Iatrogenic pneumothorax may cause substantial morbidity and, rarely, death. The incidence of iatrogenic pneumothorax is 5-7 per 10,000 hospital admissions, with thoracic surgery patients excluded because pneumothorax may be a typical outcome following these surgeries.
Pneumothorax occurs in 1-2% of all neonates, with a higher incidence in infants with neonatal respiratory distress syndrome. In one study, 19% of such patients developed a pneumothorax.
Tension pneumothorax
Tension pneumothorax is a complication in approximately 1-2% of the cases of idiopathic spontaneous pneumothorax. Until the late 1800s, TB was a primary cause of pneumothorax development. A 1962 study showed a frequency of pneumothorax of 1.4% in patients with TB.
The actual incidence of tension pneumothorax outside a hospital setting is impossible to determine. Approximately 10-30% of patients transported to level-1 trauma centers in the United States receive prehospital decompressive needle thoracostomies; however, not all of these patients actually have a true tension pneumothorax. Although this occurrence rate may seem high, disregarding the diagnosis would probably result in unnecessary deaths. A review of military deaths from thoracic trauma suggests that as many as 5% of combat casualties with thoracic trauma have tension pneumothorax at the time of death. [29]
The overall incidence of tension pneumothorax in the ICU is unknown. The medical literature provides only glimpses of the frequency. In one report, of 2000 incidents reported to the Australian Incident Monitoring Study (AIMS), 17 involved actual or suspected pneumothoraces, and four of those were diagnosed as tension pneumothorax.
Catamenial pneumothorax
Catamenial pneumothorax is a rare phenomenon that generally occurs in women aged 30-50 years. It frequently begins 1-3 days after menses onset. The risk of thoracic endometriosis cannot be predicted from the site of peritoneal lesions. [17]
Pneumomediastinum
Spontaneous pneumomediastinum generally occurs in young, healthy patients without serious underlying pulmonary disease, mostly in the second to fourth decades of life. A slight predominance of pneumomediastinum exists for males. This condition occurs in approximately 1 case per 10,000 hospital admissions.
Prognosis
Primary, secondary, and recurring spontaneous pneumothorax
Complete resolution of an uncomplicated pneumothorax takes approximately 10 days. PSP is typically benign and often resolves without medical attention. Many affected individuals do not seek medical attention for days after symptoms develop. This trend is important, because the incidence of reexpansion pulmonary edema increases in patients whose chest tubes have been placed 3 days or longer after the pneumothorax occurred.
Recurrences usually strike within the first 6 months to 3 years. The 5-year recurrence rate is 28-32% for PSP and 43% for SSP.
Recurrences are more common among patients who smoke, patients with COPD and patients with AIDS. Predictors of recurrence include pulmonary fibrosis, younger age, and increased height-to-weight ratio. In a retrospective study of 182 consecutive patients with a newly diagnosed first episode of pneumothorax, a higher rate of recurrence was noted in taller patients, thin patients, and patients with SSP.
Patients who underwent bedside chest-tube pleurodesis had cumulative rates of recurrence of 13% at 6 months, 16% at 1 year, and 27% at 3 years, compared with 26%, 33%, and 50%, respectively. The agent used (tetracycline or gentamicin) did not have any significant impact on the recurrence rate.
Bullous lesions found on CT or at thoracoscopy and the presence of ELCs in PSP are also not predictive of recurrence. In a retrospective study of 231 patients with PSP, however, contralateral blebs were more frequently seen by CT in the patients with contralateral recurrence (n = 33; 14%) than in those without a contralateral recurrence. Primary bilateral spontaneous pneumothorax (PBSP) was significantly more common in patients with lower body mass index (BMI) and among smokers. [34] In this series, all patients with contralateral recurrence were treated surgically.
Although some authors view PSP as more of a nuisance than a major health threat, deaths have been reported. SSPs are more often life threatening, depending on the severity of the underlying disease and the size of the pneumothorax (1-17% mortality). In particular, compared with similar patients without pneumothorax, age-matched patients with COPD have a 3.5-fold increase in relative mortality when a spontaneous pneumothorax occurs, and their risk of recurrence rises with each occurrence. One study indicated that 5% of patients with COPD died before a chest tube was placed.
Patients with AIDS also have a high inpatient mortality rate of 25% and a median survival of 3 months after the pneumothorax. These data were derived from an era before highly active antiretroviral therapy (HAART) was available.
Tension pneumothorax
Tension pneumothorax arises from numerous causes and rapidly progresses to respiratory insufficiency, cardiovascular collapse, and, ultimately, death if not recognized and treated. Therefore, if the clinical picture fits a tension pneumothorax, it must be treated on an emergency basis before it results in hemodynamic instability and death.
Pneumomediastinum
Pneumomediastinum is generally a benign, self-limited condition. Malignant pneumomediastinum, or tension pneumomediastinum (unvented mediastinal or pulmonary adventitial air causing pressure so high that circulatory or ventilatory failure occurs), was first described in 1944; however, all patients described in this report had serious comorbid conditions, often related to trauma or in association with Boerhaave syndrome.
The more recent literature has not included reports of fatal outcomes in patients with spontaneous pneumomediastinum in the absence of underlying disease. Mortality is as high as 70% in patients with pneumomediastinum secondary to Boerhaave syndrome, even with surgical intervention. Traumatic mediastinum, though present in as many as 6% of patients, does not portend serious injury. [35]
Patient Education
Two important concerns that clinicians should educate patients with pneumothorax/resolving pneumothorax about are (1) avoidance of travel by air or to remote regions and (2) prohibition of smoking. Patients should also be advised to wear safety belts and passive restraint devices while driving.
Avoidance of travel by air or to remote areas
Patients should not travel by air or travel to remote sites until radiography shows complete resolution. Although commercial air travel causes only minimal change in gas volumes, because of pressurization of the cabin, spontaneous pneumothorax has been described during commercial travel.
Patients with previous spontaneous pneumothoraces are at risk for recurrence and are advised not to dive unless thoracotomy or pleurodesis has been performed. [36] Ascent from deep-sea diving causes gases to expand and can lead to pneumothorax in patients with bullae and blebs.
Smoking cessation
Smoking cessation is strongly advised for all patients. patients should be assessed as to their readiness to quit, should be educated about smoking cessation, and should be provided with pharmacotherapy if ready to quit. Patients indicating a readiness to quit smoking should be directed to their primary care physician or offered referral for cessation management. This may include nicotine replacement and non-nicotine pharmacotherapy (eg, bupropion or varenicline).
With either primary or secondary pneumothorax, smoking increases the likelihood of bleb rupture and recurrence, and it does so in a predictable, dose-related manner. The relative risk of bleb rupture and recurrence rises by up to a factor of 20.
For patient education information, see the Lung and Airway Center and Breathing Difficulties Center, as well as Collapsed Lung (Pneumothorax) and Chest Pain.
-
Radiograph of patient with small spontaneous primary pneumothorax.
-
Close radiographic view of patient with small spontaneous primary pneumothorax (same patient as in previous image).
-
Expiratory radiograph of patient with small spontaneous primary pneumothorax (same patient as in previous images).
-
Radiograph of patient with spontaneous primary pneumothorax due to left-upper-lobe bleb.
-
Close radiographic view of patient with spontaneous primary pneumothorax due to left-upper-lobe bleb (same patient as in previous image).
-
Radiograph of patient with large spontaneous tension pneumothorax.
-
Radiograph showing subcutaneous emphysema and pneumothorax.
-
Chest radiograph shows two abnormalities: (1) tension pneumothorax and (2) potentially life-saving intervention delayed during wait for x-ray results. Tension pneumothorax is clinical diagnosis requiring emergency needle decompression, and therapy should never be delayed for x-ray confirmation.
-
Radiograph of new left-side pneumothorax in patient on mechanical ventilation, requiring high inflation pressures.
-
Radiograph of patient with a complete right-side pneumothorax due to stab wound.
-
Radiograph of patient with idiopathic pulmonary fibrosis and small pneumothorax, following video-assisted thoracoscopic surgery (VATS) lung biopsy.
-
Close radiographic view of small pneumothorax ina patient with idiopathic pulmonary fibrosis, following video-assisted thoracoscopic surgery (VATS) lung biopsy (same patient as in previous image). Note that hole on chest tube is outside pleural space.
-
Radiograph showing right-side iatrogenic pneumothorax after transbronchial biopsy.
-
Pneumomediastinum from barotrauma may result in tension pneumothorax and obstructive shock.
-
Radiograph of patient in ICU who developed pneumopericardium as manifestation of barotrauma.
-
Radiograph of older man who was admitted to ICU postoperatively. Note right-side pneumothorax induced by incorrectly positioned small-bowel feeding tube in right-side bronchial tree. Marked depression of right hemidiaphragm is noted, and mediastinal shift is to left, suggestive of tension pneumothorax. Endotracheal tube is in good position.
-
Radiograph showing right mainstem intubation that resulted in left-side tension pneumothorax, right mediastinal shift, deep sulcus sign, and subpulmonic pneumothorax.
-
Chest radiograph of elderly man with chronic obstructive pulmonary disease who presented with second left-side spontaneous pneumothorax in 2 months. Chest thoracostomy was performed, patient was admitted, and talc pleurodesis was performed on following day.
-
Chest radiograph shows pneumomediastinum (radiolucency noted around left heart border) in patient who had respiratory and circulatory arrest in emergency department after experiencing multiple episodes of vomiting and rigid abdomen. Patient was taken immediately to operating room, where large rupture of esophagus was repaired.
-
Radiograph demonstrating tension and traumatic pneumothorax.
-
Radiograph demonstrating tension and traumatic pneumothorax.
-
Lateral radiograph demonstrating tension and traumatic pneumothorax.
-
Lateral radiograph demonstrating tension and traumatic pneumothorax.
-
Chest radiograph showing tension and traumatic pneumothorax.
-
Lateral radiograph showing tension and traumatic pneumothorax.
-
CT scan demonstrating blebs in patient with chronic obstructive pulmonary disease (COPD).
-
CT scan demonstrating bulla in asymptomatic patient.
-
CT scan demonstrating secondary spontaneous pneumothorax (SSP) from radiation/chemotherapy for lymphoma.
-
CT scan demonstrating emphysematouslike changes (ELCs) in patient with chronic obstructive pulmonary disease (COPD).
-
CT scan in patient with history of bilateral pleurodesis and strong family history of spontaneous pneumothorax.
-
Illustration depicting multiple fractures of left upper chest wall. First rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along midlateral (red arrows) or anterior chest wall (blue arrows), flail chest (dotted black lines) may result, which may result in pneumothorax.
-
Insertion of chest tube. Video courtesy of Therese Canares, MD, and Jonathan Valente, MD, Rhode Island Hospital, Brown University.
Tables

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Approach Considerations
- Treatment Based on Risk Stratification
- Options for Restoring Air-Free Pleural Space
- Prehospital Care
- Hospital Management
- Indications for Surgical Assistance
- Video-Assisted Thoracoscopic Surgery
- Thoracotomy
- Pleurodesis
- Complications
- Prevention
- Consultations
- Long-Term Monitoring
- Show All
- Guidelines
- Medication
- Questions & Answers
- Media Gallery
- References








