Overview
Pneumonia in the immunocompromised host is a complex infection and inflammation of the lower respiratory tract, complicated by widespread multidrug antibiotic resistance, and aided by medical advances such as improvements in diagnostic measures and immunosuppressive agents. About 20-30% of hospitalized patients who are hospitalized with community-acquired pneumonia have immunocompromising conditions. [1] Though overall patient survival has increased, pneumonia is both the most common invasive infection in immunocompromised patients and continues to carry a high mortality and morbidity rate. [2, 3, 4, 5, 6]
The major immunocompromised host groups are those with:
-
HIV/AIDS
-
Solid organ and hematopoietic cell transplants
-
Malignancy on chemotherapy or radiation therapy
-
Primary immunodeficiencies and autoimmune diseases
-
Acquired immunodeficiencies: asplenia, long-term steroid use
 Chest radiograph of HIV-infected patient with PJP shows diffuse patchy infiltrates with predominantly perihilar and interstitial prominence, as well as a few pneumatocoeles up to 1cm in size. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Andrew Dixon, rID 9613.
Chest radiograph of HIV-infected patient with PJP shows diffuse patchy infiltrates with predominantly perihilar and interstitial prominence, as well as a few pneumatocoeles up to 1cm in size. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Andrew Dixon, rID 9613.
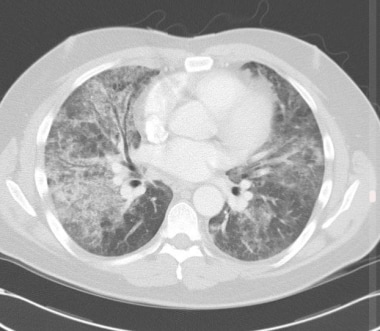 Chest CT of HIV-infected patient with PJP shows early findings of diffuse ground glass opacities, and chronic findings of linear opacities and thickening of interlobular septa. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Yune Kwong, rID 26697.
Chest CT of HIV-infected patient with PJP shows early findings of diffuse ground glass opacities, and chronic findings of linear opacities and thickening of interlobular septa. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Yune Kwong, rID 26697.
Complications
Pneumonia in immunocompromised is often complicated by superinfection, drug toxicity, empyema, sepsis, pneumothorax, and acute respiratory distress syndrome (ARDS).
Causes of Pneumonia
The number of potential pulmonary pathogens is increasing as a result of new immunosuppressive therapies, the emergence of multi-drug-resistant organisms, and improved diagnostic modalities.
There are four major groups of pathogens responsible for pneumonia in immunocompromised patients. Depending on the underlying immune defect, the likelihood of each of these etiologies for infection is varied.
Bacterial: Tuberculosis (TB) and non-TB mycobacteria, mainly Mycobacterium avium complex (MAC)
Fungal: Pneumocystis jirovecii, Aspergillus fumigatus, Candida, Cryptococcus neoformans, Mucormycosis species, and other fungi including Coccidioides immitis, and Histoplasma capsulatum
Viruses: Cytomegalovirus (CMV), community-acquired respiratory infections including influenza, and herpes simplex virus (HSV) and varicella zoster virus (VZV)
Parasites: Strongyloides, toxoplasmosis
HIV/AIDS
Patients with human immunodeficiency virus (HIV) are at risk for a number of pulmonary infections. Pneumocystis jirovecii (formerly Pneumocystis carinii) remains the most common opportunistic infection in this group, while the incidence of mycobacterial infections has decreased significantly. [2, 7]
HIV causes dysfunction of cell-mediated and humoral immunity. CD4 T cells principally help other cells achieve their effector function. Low CD4 counts, which correlate with the degree of immunosuppression, cause a disruption of B-cell differentiation. Impaired B-cell functions, particularly memory cells, are correlated with increased risk of infection. [8]
Despite the advances in the development of highly active antiretroviral therapy (HAART), pulmonary disease remains an important cause of mortality and morbidity in persons with HIV/AIDS. [9, 10, 11]
Tuberculosis
HIV is considered to be the greatest risk factor for TB. [12] Patients with HIV are more likely not only to contract TB, but progress from latent to active TB. [13] In addition, they have a higher mortality risk from TB.
 Chest radiograph in a patient with HIV infection and focal infiltrates due to tuberculosis.
Chest radiograph in a patient with HIV infection and focal infiltrates due to tuberculosis.
The clinical manifestations of TB in persons with HIV depend on the degree of immunosuppression. In severely immunocompromised individuals, the typical presentation of TB becomes less frequent. Instead of upper lobe cavitary disease, some of these patients present with lower lobe primary pneumonias, nonspecific patterns, or even no chest radiograph findings. [14]
Tuberculin skin test (TST) is more likely to be negative in persons with HIV. Typically, interferon-gamma release assays (IGRAs) are the gold standard for identification of TB-infected individuals; however, in HIV patients, the sensitivity of IGRAs is diminished. In studies, IGRAs perform similarly to the TST. Since both methods have a modest predictive value and suboptimal sensitivity, the choice of test should be based on country guidelines and resource considerations. [15]
Studies have shown that the timing of HAART and tuberculosis therapy is important in those concurrently infected. Withholding HAART until the third week of anti-tuberculosis therapy likely reduced TB mortality. [16]
Bacterial pneumonia
The most common bacterial causes of community-acquired pneumonia (CAP) in patients with HIV are the same as those in the general population [17] , the top three being Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus. [18, 19, 20]
However, the risks of contracting Streptococcus pneumonia are increased 10,000-fold in a patient with HIV. [21] Protease inhibitor (PI) containing ART regimens show great effect in lowering this risk. [22]
In a nosocomial setting, Pseudomonas aeruginosa, Staphylococcus aureus, Klebsiella pneumoniae, and Enterobacter species are common.
Fungal pneumonia
Fungal pneumonias are divided into opportunistic (ie PCP, Candida, Aspergillus, Mucor species) and endemic (Histoplasma capsulatum, Coccidioides immitis, Cryptococcus neoformans).
Opportunistic: Pneumocystis jirovecii pneumonia (PJP)
Pneumocystis jirovecii infection remains the most common opportunistic infection among patients with HIV.
It becomes a concern in individuals when CD4 count drops below 200, which is when prophylaxis with trimethoprim-sulfamethoxazole (TMP-SMX) is recommended. When the A-a gradient is >35 or a room air arterial blood gas pO2< 70, adjuvant corticosteroids are recommended.
Transmission and infectivity of P. jirovecii is incompletely understood, in most cases attributed to reactivation of latently colonized patients. [23]
Opportunistic: Aspergillus
Invasive aspergillus pneumonia is one of the four aspergillosis syndromes that primarily affects immunosuppressed individuals.
In solid organ and hematopoietic transplant patients, there is a bimodal distribution of incidence with peaks during 1. prolonged neutropenia before engraftment and 2. in later stages with corticosteroid therapy in treatment of graft-versus-host disease.
Patients with leukemia and lymphoma have a higher incidence of invasive aspergillosis which is associated with a higher mortality rate. [24]
Invasive aspergillosis is also being increasingly observed in patients with severe COPD who remain on long-term corticosteroid therapy. [25]
There are no reliable biomarkers for detection of fungal cell wall constituents or other specific measures, thus, the recommendation continues to be close monitoring of clinical signs and symptoms for prevention and prophylaxis of opportunistic fungal pneumonias. [26]
Endemic: Cryptococcus neoformans
Cryptococcal pneumonia is more severe in patients with HIV. Patients with pulmonary disease frequently progress to disseminated disease. [27]
Most cases are the result of the reactivation of a latent infection.
Endemic: Histoplasma capsulatum
For the immunocompetent host, histoplasmosis is frequently asymptomatic or self-limited. In the setting of HIV/AIDS, this infection is much more common and frequently progresses to disseminated disease.
This infection is endemic to certain areas of the United States, particularly in states bordering the Ohio River valley and the lower Mississippi River.
Spores of the mold phase are inhaled and cause a localized or patchy bronchopneumonia. CD4 lymphocytes normally activate macrophages to control the infection. [28]
Endemic: Coccidioides immitis
Coccidioides immitis is an organism endemic to large parts of the southwestern United States.
Spores are inhaled and then ingested by pulmonary macrophages. Impaired cell-mediated immunity in persons with HIV accounts for an increased risk of infection in these patients. [29]
Viruses
Varicella zoster virus
Visceral dissemination of primary varicella, especially pneumonitis, has been reported in persons with HIV. [30]
Parasites
Strongyloides stercoralis
Strongyloides is an human intestinal nematode which can reproduce and persist in the body indefinitely, and affects millions of people worldwide. In immunocompromised individuals, this autoinfective cycle can be amplified into a hyperinfection syndrome. Increased parasite burden migrates rom the gastrointestinal tract, where it causes GI bleeding, into a systemic process. Filariform larvae have been found in the respiratory system, where they cause respiratory distress and sepsis secondary to pneumonia, and the neurological system causing meningitis.
Though the two conditions most often shown to trigger hyperinfection are glucocorticoid treatment and human T-lymphotropic virus type 1 infection, it is also associated with HIV/AIDS and hematologic malignancy. Anthelmintic agents such as ivermectin have been used successfully in both treatment as well as primary and secondary prevention in patients with risk factors. [31]
 Chest radiograph demonstrating diffuse bilateral infiltrates in a patient with Pneumocystis carinii pneumonia.
Chest radiograph demonstrating diffuse bilateral infiltrates in a patient with Pneumocystis carinii pneumonia.
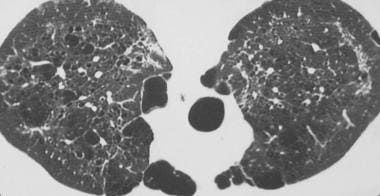 High-resolution computed tomography scan obtained through the upper lobes in the prone position in a patient with a history of Pneumocystis carinii pneumonia. This image shows parenchymal and subpleural cysts and patchy fibrosis that resulted from the Pneumocystis carinii infection.
High-resolution computed tomography scan obtained through the upper lobes in the prone position in a patient with a history of Pneumocystis carinii pneumonia. This image shows parenchymal and subpleural cysts and patchy fibrosis that resulted from the Pneumocystis carinii infection.
 Chest radiograph in a patient with HIV infection, bilateral perihilar infiltrates, and Pneumocystis carinii pericarditis.
Chest radiograph in a patient with HIV infection, bilateral perihilar infiltrates, and Pneumocystis carinii pericarditis.
Other Causes of Immunodeficiency
Malignancy/neutropenia
Malignancy, especially hematologic malignancy, is a large risk factor for developing pneumonia. The pathogenicity and severity of disease is related to the degree and duration of neutropenia. Most infectious etiologies are polymicrobial including gram-positive and gram-negative organisms from the upper respiratory tract. However, in about 10-25% of patients, an infectious focus is not identified in sputum, with the only evidence of infection being a positive blood culture. [32]
Patients with profound, prolonged neutropenia are more susceptible to invasive fungal pathogens such as Aspergillus species, and the agents of mucormycosis. [33]
Viruses are also involved, primarily VZV. Respiratory viruses such as influenza, respiratory syncytial virus (RSV), Adenovirus, and Metapneumovirus are increasingly documented in neutropenic patients.
Mortality in patients with febrile neutropenia is 30-50%. [34, 35]
The American Society of Clinical Oncology (ASCO) recommend prophylaxis (eg, with trimethoprim-sulfamethoxazole) for patients receiving chemotherapy regimens associated with >3.5% risk for Pneumocystis jirovecii pneumonia. [36, 37]
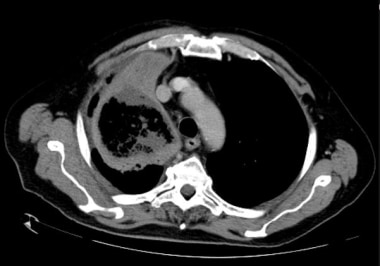 CT of AML patient with a fungal pneumonia in the right upper lobe characterized by a cavitary lesion without air fluid levels. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Roberto Schubert, rID 17628.
CT of AML patient with a fungal pneumonia in the right upper lobe characterized by a cavitary lesion without air fluid levels. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Roberto Schubert, rID 17628.
Transplant immunosuppression
Solid-organ and bone-marrow transplant patients have a heightened risk of pulmonary infection as well. The specific organ, timeframe since transplant, and use of immunosuppressive medications are all important in predicting these complications.
CMV pneumonitis is common in solid organ transplant, particularly lung, recipients. The risk is higher if the donor is seropositive and the recipient seronegative. Interestingly, the opposite is seen in hematological stem cell transplant (HCT) patients, where there is a higher risk for CMV pneumonitis among seropositive recipients transplanted with seronegative stem cells.
Nocardia species are another notable cause of pulmonary infection in organ transplant patients requiring long-term immunosuppression.
Reactivation of viruses causing pneumonia is a large concern in HCT patients, even in autologous transplants. Human herpesvirus 6 (HHV-6) reactivation is most common (seen in up to 60% of patients), followed by EBV (up to 30%). [38, 39, 40] .
HHV-6 infection is especially important in that it has been shown to be a predictor of subsequent CMV infection. [41]
Solid organ and HCT recipient are at risk also of hyperinfection with Strongyloides stercoralis, which may be accompanied by gram-negative bacterial sepsis and pneumonia.
Autoimmune diseases
Infections in persons with autoimmune conditions can result from the effects of immunosuppressive therapies as well as their underlying condition.
In systemic lupus erythematosus (SLE), distinguishing infection from an autoimmune flare is important. Treatment with steroids in the setting of infection could be deleterious.
Complement deficiencies and elevated Fc gamma III and granulocyte-macrophage colony-stimulating factor (GM-CSF) levels may contribute to increased susceptibility to infection in patients with SLE. [42]
Low complement, the use of more than 20 mg prednisone daily, and the use of cyclophosphamide in patients with SLE were important risk factors in multivariate analyses. [43]
Consideration of initiating prophylaxis for Pneumocystic jiroveci in SLE patients exceeding 20 mg of prednisone a day or with usage of cyclophosphamide has been proposed. [44]
The large majority of infectious complications are due to bacterial pathogens. Viral infections (CMV, VZV) are also common.
In connective tissue diseases, the primary condition and the use of immunosuppressive medications place patients at increased risk. One meta-analysis showed that 29% of patients developed a serious infection, and 24% died from this infection—most reported as bacteremia or pneumonia. [45]
Primary immunodeficiencies
Persons with primary immunodeficiencies are susceptible to pulmonary infections, the spectrum of which is largely determined by their underlying immune dysfunction: humoral, cellular, or combined deficiencies.
Humoral immunity deficiencies impact the ability to create functional antibodies. Characteristic infections are bacterial-based, recurrent, upper and lower respiratory tract infections. Common pathogens include the encapsulated bacteria Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis, as well as Giardia, Cryptosporidia, and Campylobacter.
Cellular deficiencies affect T-cell development and function. Dysfunction of T cells invariably has an impact on B-cell activity; therefore, most of these conditions manifest as combined deficiencies. Infections are common from viruses (RSV, HSV, VZV, CMV, EBV, influenza), mycobacteria, and fungi (Candida, Cryptococcus, and Pneumocystis).
Steroids
Patients taking steroids long-term are at higher risk for pulmonary infections. [46]
Steroids alter phagocytic function of alveolar macrophages, delay the mobilization of immune cells, and affect antigen presentation.
The dose and duration of use are predictive of increased risk of pneumonia. Low-dose and short-term use carry minimal additional risk of pneumonia, while dosages more than 10 mg/d or cumulatively 700 mg of prednisone increase patients' risk of pulmonary infection. [47]
Asplenic patients
Asplenic patients are at particularly high risk for acquiring infections from encapsulated organisms. [21] They also have a higher rate of infection from pneumonias overall. [48]
In asplenic patients, the overall incidence of invasive pneumococcal disease is 500 cases per 100,000 per year. [21]
Clinical Presentation
Patient history
The underlying cause of immunosuppression is a crucial aspect of the history.
Nonspecific findings may include the following:
-
Fever
-
Exertional dyspnea, followed by dyspnea at rest with progression of disease
-
Cough, most often nonproductive in patients with HIV/AIDS
-
Pleuritic chest pain
-
Anorexia and weight loss
-
Abdominal pain
Physical examination
Pulmonary findings may be nonspecific in immunocompromised patients.
Findings at physical examination may include the following:
-
Fever
-
Tachypnea
-
Tachycardia or bradycardia
-
Rales or rhonchi
-
Decreased breath sounds
-
Dullness to percussion
-
Egophony
Differential Diagnosis
The differential diagnosis for pneumonia in immunocompromised patients includes the noninfectious causes of pulmonary disease:
-
Radiation induced injury
-
Drug induced pulmonary disease
-
Idiopathic pneumonia syndrome
-
Engraftment syndrome
-
Primary connective tissue/collagen disease
-
Transfusion related acute lung injury (TRALI)
-
ARDS secondary to extra pulmonary processes
Laboratory Studies
Laboratory studies that should be obtained include a complete blood count (CBC) with differential, basic metabolic panel, arterial blood gas (ABG), lactate dehydrogenase (LDH) level, erythrocyte sedimentation rate (ESR), and C reactive protein (CRP).
If tuberculosis is suspected, sputum culture, sputum Gram stain, acid-fast bacillus (AFB) smear, and AFB culture should be collected while patients are in isolation.
Two sets of blood cultures, despite their low yield and infrequent impact on care, are considered standard of care. [49, 50] They are especially important in immunosuppressed individuals as they may at times be the only objective finding of infection.
Procalcitonin (PCT) level has been shown to be a reliable biomarker with good sensitivity and specificity for bacterial causes of pneumonia or other infection. As it is triggered by bacterial endotoxin, procalcitonin levels can be a useful adjuvant to distinguish bacterial etiologies of infection from viral, fungal, or autoimmune causes. Trending of PCT level is also established to be useful for initiating and guiding antibiotic therapy. [51, 52, 53]
Other routine laboratory studies may be clinically indicated, such as viral nasal swabs, urine antigen testing (Legionella pneumophila, Histoplasma capsulatum, Streptococcus pneumoniae), PCR studies (CMV, HHV6), serum antigen testing (cryptococcus, galactomannan), and other assays such as serum 1,3 beta-D-Glucan. [54]
Rapid diagnostic tests that use newer molecular techniques, such as matrix-assisted laser desorption ionization-time of flight mass spectrometry, have facilitated the identification of causative agents of pneumonia in immunocompromised patients. [1]
Chest Radiography
Chest radiography is usually the initial imaging modality.
The timing, progression, and distribution of findings are helpful in identifying correlations.
The most typical findings on chest radiography include infiltrates with consolidation, peribronchovascular lesions, and nodular space-occupying lesions.
Other findings include atelectasis, cavitation, pleural effusions, lymphadenopathy, and cardiomegaly.
Some findings are correlated with certain etiologies of pulmonary infection; however, the pattern of radiographic findings is often unreliable in immunocompromised patients given the decreased inflammatory response.
For instance, as many as 14% of chest radiographic findings are normal in AIDS patients with pulmonary TB. [55]
Chest radiograph demonstrating diffuse bilateral infiltrates in a patient with Pneumocystis carinii pneumonia.
Chest radiograph in a patient with HIV infection and focal infiltrates due to tuberculosis.
Chest CT Scanning
Chest computed tomography (CT) can often detect abnormalities that may or may not be well visualized on chest radiography, and thus are useful in identifying small or early consolidations, characterizing extent and heterogenicity of disease, facilitating earlier diagnoses, and directing therapeutic management. [56]
High-resolution computed tomography scan obtained through the upper lobes in the prone position in a patient with a history of Pneumocystis carinii pneumonia. This image shows parenchymal and subpleural cysts and patchy fibrosis that resulted from the Pneumocystis carinii infection.
CT is especially effective at defining extent of disease, including when multiple patterns of injury are occurring simultaneously.
The other major benefit of CT imaging is its utility in therapeutic procedures, including lung biopsy and tissue excision.
Lung Sampling
Lung sampling may be performed by bronchoscopy, transbronchial biopsy (TBB), or video-assisted thoracic surgery (VATS).
Bronchoscopy, the least invasive of these three sampling modalities, allows collection of diagnostic samples by bronchoalveolar lavage (BAL), fibrobronchial aspirate (FBAS), and protected specimen brush (PSB). This technique is high-yield for diagnosis of pneumonias, especially in conjunction with clinical and non-invasive methods. BAL has been specifically shown to be a highly sensitive and moderately specific test to diagnose of Pneumocystic jirovecii in HIV patients. [57]
The role of BAL in diagnosing pulmonary infections also established in non-HIV immunocompromised patients. [58, 59] Some sources suggest transbronchial biopsy in conjunction with BAL in non-HIV immunocompromised patients to detect other processes such as drug-induced lung injury or bronchiolitis obliterans.
TBB is established in diagnosis of diffuse parenchymal lung disease including interstitial fibrosis, but has shown promise in identifying fungal or viral pneumonia and inflammatory reactions. [60, 61]
Initial Treatment
Prehospital Care
Prehospital care should be initiated as soon as possible, and includes:
-
Supplemental oxygen administration
-
Establishment of intravenous access
-
Vital sign monitoring including oxygen saturation and cardiac monitoring
Emergency Department Care
Emergency department care encompasses the same measures as prehospital care above, but also includes:
-
Initial stabilization and resuscitation of the patient as needed according to "ABCs":
- Circulation: crystalloid intravascular resuscitation with or without vasopressor support
- Airway/Breathing: positive pressure ventilatory support or endotracheal intubation with mechanical ventilation
-
Diagnostic measures including:
- Basic bloodwork
- Sputum Gram stain and cultures
- Serologies including serum and urine antigen
- Imaging including radiography and CT
- Blood cultures
-
Empiric antimicrobial therapy based on most likely pathogens
-
In the case of PCP pneumonia, recommendations are for adjuvant corticosteroid therapy when a room air arterial blood gas pO2 is < 70, or if the A-a gradient is >35. In a recent double-blinded RCT in HIV-infected infants, early administration of prednisolone at 48 hours after clinical diagnosis of PJP significantly reduced mortality in hospital and 6 months after discharge. [62] New research suggests that the current guidelines of a 21-day therapy can safely be reduced to 14 days in 60% of moderate-to-severe HIV-PCP and 90% of moderate cases. [63]
Consultations
Consultation with the following consultants may be considered:
-
Pulmonologist and/or critical care specialist
-
Infectious disease specialist
-
Immunologist in cases of known or suspected primary immunodeficiency
If outpatient management is possible, arrange for follow-up with a primary care practitioner within 24 hours.
Pharmacologic Treatment
Pharmacologic therapy consists mainly of empiric antibiotics awaiting results of diagnostic studies.
Taking into consideration each patient's characteristics and risk factors, a narrow differential diagnosis can be established and help tailor therapy to the most likely organism and prevent overuse of anti-microbe therapy.
A meta-analysis by Wang et al indicated that in HIV-infected patients with P jiroveci pneumonia, early adjunctive corticosteroid treatment may lead to a 0.55 times reduced risk of mortality compared with patients who do not receive the adjunctive therapy. [64]
Prevention
Optimization of treatment of the underlying immunocompromise is a first approach to prevention of pneumonia in immunocompromised individuals. This includes HAART, chemo and radiation therapy, and other measures depending on the type of immunocompromise.
However, despite optimal therapy, prevention of opportunistic and endemic pulmonary infections can be difficult.
Vaccination against pneumococcal and influenza, as well as prophylaxis against bacteria, viruses, and fungi, are other methods of prevention.
In rheumatologic disorders in which corticosteroids and/or immunomodulators such as TNF-inhibitors play a role in symptom control, the optimization of the level of immunosuppression is as important as prophylaxis against microbial infection.
Questions & Answers
Overview
How is pneumonia characterized in immunocompromised patients?
Which immunocompromised host groups are at highest risk for pneumonia?
What are the possible complications of pneumonia in immunocompromised patients?
What causes pneumonia in immunocompromised patients?
What causes pneumonia in patients with HIV infection?
What is the clinical presentation of TB in patients with HIV infection?
How is TB diagnosed and treated in patients with HIV infection?
What causes bacterial pneumonia in patients with HIV infection?
What are the types of fungal pneumonia in patients with HIV infection?
How does Pneumocystis jirovecii pneumonia (PJP) develop in patients with HIV infection?
Which immunocompromised patients have the highest incidence of aspergillus pneumonia?
What causes cryptococcal pneumonia in immunocompromised patients?
What causes histoplasmosis pneumonia in immunocompromised patients?
What causes coccidioides immitis pneumonia in immunocompromised patients?
Which viruses cause pneumonia in immunocompromised patients?
How do strongyloides cause pneumonia in immunocompromised patients?
What are the risk factors for pneumonia in immunocompromised cancer patients?
What are the risk factors for pneumonia in immunocompromised transplant patients?
What are the risk factors for pneumonia in immunocompromised patients with autoimmune conditions?
What are the risk factors for pneumonia in patients with primary immunodeficiencies?
What is the increased risk for pneumonia in immunocompromised patients on long-term steroid therapy?
What is the incidence of pneumonia in immunocompromised asplenic patients?
Which clinical history findings are characteristic of pneumonia in immunocompromised patients?
Which physical findings are characteristic of pneumonia in immunocompromised patients?
What is the role of lab tests in the workup of pneumonia in immunocompromised patients?
What is the role of chest radiography in the workup of pneumonia in immunocompromised patients?
What is the role of chest CT scanning in the workup of pneumonia in immunocompromised patients?
What is the role of lung sampling in the workup of pneumonia in immunocompromised patients?
What is included in prehospital care for immunocompromised patients with pneumonia?
What is the initial ED treatment of suspected pneumonia in immunocompromised patients?
How is pneumonia in immunocompromised patients treated?
Which specialist consultations are beneficial to immunocompromised patients with pneumonia?
What is the role of medications in the treatment of pneumonia in immunocompromised patients?
How is pneumonia prevented in immunocompromised patients?
-
Chest radiograph demonstrating diffuse bilateral infiltrates in a patient with Pneumocystis carinii pneumonia.
-
High-resolution computed tomography scan obtained through the upper lobes in the prone position in a patient with a history of Pneumocystis carinii pneumonia. This image shows parenchymal and subpleural cysts and patchy fibrosis that resulted from the Pneumocystis carinii infection.
-
Chest radiograph in a patient with HIV infection, bilateral perihilar infiltrates, and Pneumocystis carinii pericarditis.
-
Chest radiograph in a patient with HIV infection and focal infiltrates due to tuberculosis.
-
Chest radiograph of HIV-infected patient with PJP shows diffuse patchy infiltrates with predominantly perihilar and interstitial prominence, as well as a few pneumatocoeles up to 1cm in size. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Andrew Dixon, rID 9613.
-
Chest CT of HIV-infected patient with PJP shows early findings of diffuse ground glass opacities, and chronic findings of linear opacities and thickening of interlobular septa. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Yune Kwong, rID 26697.
-
CT of AML patient with a fungal pneumonia in the right upper lobe characterized by a cavitary lesion without air fluid levels. Courtesy of Radiopaedia (https://radiopaedia.org/), case of Dr Roberto Schubert, rID 17628.









