Practice Essentials
Atrial fibrillation (AF) has strong associations with other cardiovascular diseases, such as heart failure, coronary artery disease (CAD), valvular heart disease, diabetes mellitus, and hypertension. It is characterized by an irregular and often rapid heartbeat (see the first image below). The exact mechanisms by which cardiovascular risk factors predispose to AF are not understood fully but are under intense investigation. Catecholamine excess, hemodynamic stress, atrial ischemia, atrial inflammation, metabolic stress, and neurohumoral cascade activation are all purported to promote AF.
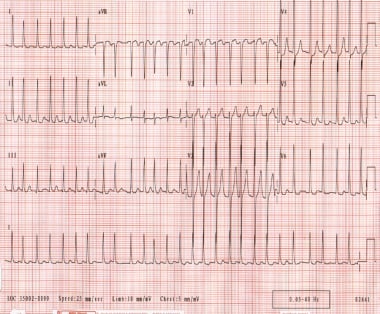 Ventricular rate varies from 130-168 beats per minute. Rhythm is irregularly irregular. P waves are not discernible.
Ventricular rate varies from 130-168 beats per minute. Rhythm is irregularly irregular. P waves are not discernible.
Signs and symptoms
The clinical presentation of AF spans the entire spectrum from asymptomatic AF with rapid ventricular response to cardiogenic shock or devastating cerebrovascular accident (CVA). Unstable patients requiring immediate direct current (DC) cardioversion include the following:
-
Patients with decompensated congestive heart failure (CHF)
-
Patients with hypotension
-
Patients with uncontrolled angina/ischemia
Initial history and physical examination include the following:
-
Documentation of clinical type of AF (paroxysmal, persistent, long-standing persistent or permanent)
-
Assessment of type, duration, and frequency of symptoms
-
Assessment of precipitating factors (eg, exertion, sleep, caffeine, alcohol use)
-
Assessment of modes of termination (eg, vagal maneuvers)
-
Documentation of prior use of antiarrhythmics and rate-controlling agents
-
Assessment of presence of underlying heart disease
-
Documentation of any previous surgical or percutaneous AF ablation procedures
-
Airway, breathing, and circulation (ABCs)
-
Vital signs (particularly heart rate, blood pressure, respiratory rate, and oxygen saturation)
-
Evaluation of head and neck, lungs, heart, abdomen, lower extremities, and nervous system
See Clinical Presentation for more detail.
Diagnosis
Findings from 12-lead electrocardiography (ECG) usually confirm the diagnosis of AF and include the following:
-
Typically irregular ventricular rate (QRS complexes)
-
Absence of discrete P waves, replaced by irregular, chaotic F waves
-
Aberrantly conducted beats after long-short R-R cycles (ie, Ashman phenomenon)
-
Heart rate (typically 110-140 beats/min, rarely >160-170 beats/min)
-
Preexcitation
-
Left ventricular hypertrophy
-
Bundle-branch block or intraventricular conduction delay
-
Acute or prior myocardial infarction (MI)
Transthoracic echocardiography (TTE) is helpful for the following applications:
-
To evaluate for valvular heart disease
-
To evaluate atrial and ventricular chamber and wall dimensions
-
To estimate ventricular function and evaluate for ventricular thrombi
-
To estimate pulmonary systolic pressure (pulmonary hypertension)
-
To evaluate for pericardial disease
Transesophageal echocardiography (TEE) is helpful for the following applications:
-
To evaluate for atrial thrombus (particularly in the left atrial appendage)
-
To guide cardioversion (if thrombus is seen, cardioversion should be delayed)
See Workup for more detail.
Management
The cornerstones of AF management are rate control and anticoagulation, [1] as well as rhythm control for those symptomatically limited by AF. The clinical decision to use a rhythm-control or a rate-control strategy requires integrated consideration of the following:
-
Degree of symptoms
-
Likelihood of maintaining sinus rhythm after successful cardioversion
-
Presence of comorbidities
-
Candidacy for AF ablation
Anticoagulation
The 2014 American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Rhythm Society (HRS) guidelines on anticoagulation for patients with nonvalvular AF include the following [1] :
-
No risk factors: No anticoagulation or antiplatelet therapy
-
One moderate-risk factor: Aspirin 81-325 mg/day, or anticoagulants
-
Any high-risk factor or more than one moderate-risk factor: Anticoagulants
Risk factors for thromboembolism in AF are as follows:
-
High-risk factors: Prior stroke or transient ischemic attack (TIA), systemic thromboembolism, or age 75 years or older
-
Moderate-risk factors: Age 65-74 years, female sex, hypertension, diabetes mellitus, heart failure, arterial disease (prior myocardial infarction, peripheral arterial disease, aortic plaque)
Anticoagulation is indicated as follows:
-
Patients with newly diagnosed AF and those awaiting electrical cardioversion can be started on intravenous (IV) heparin or low-molecular-weight heparin (LMWH) (1 mg/kg twice daily)
-
Concomitantly, patients can be started on warfarin in an inpatient setting while awaiting a therapeutic international normalized ratio (INR) value of 2-3
-
Newer oral anticoagulants present an alternative to warfarin in patients with nonvalvular AF; their onset of action is almost immediate and eliminates the need for bridging with heparin/LMWH.
Newer oral anticoagulants that have been approved by the US Food and Drug Administration (FDA) include the following:
-
One direct thrombin inhibitor: Dabigatran
-
Three factor Xa inhibitors: Rivaroxaban, apixaban, edoxaban
Risk of bleeding
Optimal long-term strategies for AF management should be based on a thoroughly integrated consideration of patient-specific factors and the likelihood of success. Selection of an appropriate antithrombotic regimen should be balanced between the risk of stroke and the risk of bleeding.
Factors that increase the risk of bleeding with anticoagulation include the following:
-
History of bleeding (the strongest predictive risk factor)
-
Age older than 75 years
-
Liver or renal disease
-
Malignancy
-
Thrombocytopenia or aspirin use
-
Hypertension
-
Diabetes mellitus
-
Anemia
-
Prior stroke
-
Fall risk
-
Genetic predisposition
-
Supratherapeutic INR (for warfarin)
For patients with clinical indications for anticoagulation who are at an unacceptably high risk of clinically significant bleeding, two treatment alternatives exist:
-
Left atrial appendage isolation using the catheter-based WATCHMAN device (the only FDA device currently approved in the United States)
-
Left atrial appendage ligation using the LARIAT epicardial/endocardial suture system
Rate control strategies
-
Medications (non-dihydropyridine calcium channel blockers, beta-blockers, digoxin [rarely as monotherapy], amiodarone [mainly for patients who are intolerant of, or unresponsive to, other agents])
-
Atrioventricular node modification with placement of a permanent pacemaker (invasive procedure indicated in patients when other rate and rhythm control alternatives have been exhausted)
Rhythm control strategies
-
Electrical cardioversion (generally employed as a the first-line management strategy in young symptomatic patients)
-
Medications (flecainide, propafenone, dofetilide, amiodarone, sotalol)
-
Ablation (catheter based, surgical, or hybrid)
Catheter ablation is recommended in the 2014 ACC/AHA/HRS AF guidelines for the following indications [1] :
-
It is useful for patients with symptomatic paroxysmal AF who are intolerant of, or whose condition is refractory to, rhythm-control medications.
-
It is reasonable as a treatment for patients with symptomatic persistent AF who are intolerant of, or whose condition is refractory to, a rhythm-control strategy using medications.
-
It is a reasonable alternative for patients with recurrent symptomatic paroxysmal AF who have not tried a rhythm-control medication.
See Treatment and Medication for more detail.
Background
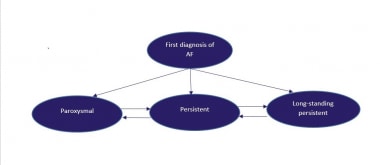
Classification of atrial fibrillation (AF) begins with distinguishing a first detectable episode, irrespective of whether it is symptomatic or self-limited. Published guidelines from an American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Rhythm Society (HRS) committee of experts on the treatment of patients with atrial fibrillation recommend classification of AF into the following three patterns (also see the image below) [1] :
-
Paroxysmal AF: Episodes of AF that terminate spontaneously within 7 days (most episodes last less than 24 hours)
-
Persistent AF: Episodes of AF that last more than 7 days and may require either pharmacologic or electrical intervention to terminate
-
Long-standing persistent AF: AF that has persisted for more than 12 months, either because cardioversion has failed or because cardioversion has not been attempted
-
Permanent AF: When both patient and clinician have decided to abort any further restoration strategies after shared clinical decision making
This classification schema pertains to cases that are not related to a reversible cause of AF (eg, thyrotoxicosis, electrolyte abnormalities, acute ethanol intoxication). In current clinical practice, atrial fibrillation secondary to acute myocardial infarction, cardiac surgery, pericarditis, sepsis, pulmonary embolism, or acute pulmonary disease is considered separately. This is because, in these situations, AF is thought to be less likely to recur once the precipitating condition has been treated adequately and has resolved.
However, data from the Framingham Heart Study suggest that over 60% of the participants with secondary AF developed recurrent AF over 15-years of follow-up. [2] Furthermore, the long-term risks of stroke and all-cause mortality were similar between participants without a secondary precipitant and those with secondary precipitants. Thus, long-term AF screening strategies can be considered in these patients similar to the current standard of practice for patients with cryptogenic stroke. [3]
Paroxysmal AF
Atrial fibrillation is considered to be recurrent when a patient has two or more episodes. If recurrent AF terminates spontaneously, it is designated as paroxysmal.
Some patients with paroxysmal AF, typically younger patients, have been found to have distinct electrically active foci within their pulmonary veins. These patients generally have many atrial premature beats noted on Holter monitoring. Isolation or elimination of these foci can lead to elimination of the trigger for paroxysms of AF.
Paroxysmal AF may progress to persistent AF, and aggressive attempts to restore and maintain sinus rhythm may prevent comorbidities associated with AF.
Persistent AF
If recurrent AF is sustained, it is considered persistent, irrespective of whether the arrhythmia is terminated by either pharmacologic therapy or electrical cardioversion.
Persistent AF may be either the first presentation of AF or the result of recurrent episodes of paroxysmal AF. Patients with persistent AF also include those with longstanding AF in whom cardioversion has not been indicated or attempted, often leading to permanent AF.
Patients can also have AF as an arrhythmia secondary to cardiac disease that affects the atria (eg, congestive heart failure, hypertensive heart disease, rheumatic heart disease, coronary artery disease). These patients tend to be older, and AF is more likely to be persistent.
Persistent AF with an uncontrolled, rapid ventricular heart rate response can cause a dilated cardiomyopathy and can lead to electrical remodeling in the atria (atrial cardiomyopathy). Therapy, such as drugs or atrioventricular nodal modification and permanent pacemaker implantation, to control the ventricular rate can improve left ventricular function and improve quality-of-life scores.
Long-standing persistent AF
Permanent AF is recognized as the accepted rhythm, and the main treatment goals are rate control and anticoagulation. Although it is possible to reverse the progression from paroxysmal to persistent and to long-standing persistent, this task can be challenging.
Lone atrial fibrillation
In addition to the above schema, the term "lone atrial fibrillation" has been used to identify AF in younger patients without structural heart disease, who are at a lower risk for thromboembolism. The definition of lone AF remains controversial, but it generally refers to paroxysmal, persistent, or permanent AF in younger patients (< 60 y) who have normal echocardiographic findings. [4] The most recent ACC/AHA/HRS guidelines recommend against using “lone AF” as a separate entity and utilizing the standard AF management tools for all patients. [1]
For patient education resources, see Heart Health Center and Brain and Nervous System Center, as well as Atrial Fibrillation (AFib), Arrhythmias (Heart Rhythm Disorders), Stroke, and Supraventricular Tachycardia (SVT, PSVT).
Pathophysiology
Three forms of atrial remodeling during a progression of atrial fibrillation (AF) have been described: electrical, contractile, and structural. [5] Electrical remodeling is a consequence of high atrial rates and includes shortening of the refractory period of atrial myocytes and slowing of atrial conduction velocity. [6] Structural remodeling is characterized both by changes in atrial myocytes [7, 8] in the interstitium, [9, 10] and by changes in extracellular matrix composition and deposition of fibrotic tissue. [11] Changes at the level of atrial myocytes include the loss of contractile structures and expression of fetal-like proteins, and accumulation of glycogen in the atrial interstitium. [12]
Changes in the interstitium are primarily manifested by the deposition of collagen fibers around cardiomyocytes. [13] Contractile remodeling is caused mainly by impaired calcium handling and may result in atrial mechanical dysfunction that may be transient or progress to irreversible dysfunction. Impaired contractility results from local changes in cell physiology and also from structural remodeling of atrial myocytes (loss of gap junctions).
Another observed morphologic feature related to AF is the presence of inflammatory cells in the atrial myocardium. [8] The role of inflammation and myocardial inflammatory infiltrate was suggested by morphologic studies on atrial tissue removed at the time of cardiac surgery and by clinical studies that monitored serum levels of inflammatory cytokines in patients with AF. [14, 15] Despite the observed association between elevated plasma levels of inflammatory markers and AF, it remains unknown whether inflammation is a systemic or local phenomenon reflecting an active inflammatory process in the atria. [14] It is also not known whether the inflammatory cells are a marker of local reaction to tissue injury caused by factors leading to AF or whether they actively participate in the maintenance of AF due to direct cytotoxic or profibrotic effects or due to indirect effects from released cytokines that may promote arrhythmogenesis. [16]
AF shares strong associations with other cardiovascular diseases, such as heart failure, coronary artery disease (CAD), valvular heart disease, diabetes mellitus, and hypertension. [17] These factors have been termed upstream risk factors, but the relationship between comorbid cardiovascular disease and AF is incompletely understood and more complex than this terminology implies. The exact mechanisms by which cardiovascular risk factors predispose to AF are not understood fully but are under intense investigation. Catecholamine excess, hemodynamic stress, atrial ischemia, atrial inflammation, metabolic stress, and neurohumoral cascade activation are all purported to promote AF.
Because diabetes mellitus and obesity are increasing in prevalence and are associated with an elevated risk of AF, Fontes et al examined whether insulin resistance is an intermediate step for the development of AF. In a community-based cohort that included 279 patients who developed AF within 10 years of follow-up, no significant association was observed between insulin resistance and incident AF. [18]
Although the precise mechanisms that cause atrial fibrillation are incompletely understood, AF appears to require both an initiating event and a permissive atrial substrate. The importance of focal pulmonary vein triggers has been highlighted in multiple studies, but alternative and nonmutually exclusive mechanisms have also been evaluated. [19] These mechanisms include multiple wavelets, mother waves, fixed or moving rotors, and macro-reentrant circuits. [19] In a given patient, multiple mechanisms may coexist at any given time. The automatic focus theory and the multiple wavelet hypothesis appear to have the best supporting data.
Automatic focus
A focal origin of AF is supported by several experimental models showing that AF persists only in isolated regions of atrial myocardium. This theory has garnered considerable attention, as studies have demonstrated that a focal source of AF can be identified in humans and that isolation of this source can eliminate AF.
The pulmonary veins appear to be the most frequent source of these automatic foci, but other foci have been demonstrated in several areas throughout the atria. Cardiac muscle in the pulmonary veins appears to have active electrical properties that are similar, but not identical, to those of atrial myocytes. Heterogeneity of electrical conduction around the pulmonary veins is theorized to promote reentry and sustained AF. Thus, pulmonary vein automatic triggers may provide the initiating event, and heterogeneity of conduction may provide the sustaining conditions in many patients with AF.
Multiple wavelet
The multiple wavelet hypothesis proposes that fractionation of wave fronts propagating through the atria results in self-perpetuating "daughter wavelets." In this model, the number of wavelets is determined by the refractory period, conduction velocity, and mass of atrial tissue. Increased atrial mass, shortened atrial refractory period, and delayed intra-atrial conduction increase the number of wavelets and promote sustained AF. This model is supported by data from patients with paroxysmal AF demonstrating that widespread distribution of abnormal atrial electrograms predicts progression to persistent AF. [20] Intra-atrial conduction prolongation has also been shown to predict recurrence of AF. [21] Together, these data highlight the importance of atrial structural and electrical remodeling in the maintenance of AF [19] —hence the phrase "atrial fibrillation begets atrial fibrillation."
Etiology
Atrial fibrillation (AF) is strongly associated with the following risk factors:
-
Hemodynamic stress
-
Atrial ischemia
-
Inflammation
-
Noncardiovascular respiratory causes
-
Alcohol and drug use
-
Endocrine disorders
-
Neurologic disorders
-
Genetic factors
-
Advancing age
Hemodynamic stress
Increased intra-atrial pressure results in atrial electrical and structural remodeling and predisposes to AF. The most common causes of increased atrial pressure are mitral or tricuspid valve disease and left ventricular dysfunction. Systemic or pulmonary hypertension also commonly predisposes to atrial pressure overload, and intracardiac tumors or thrombi are rare causes.
Atrial ischemia
Coronary artery disease infrequently leads directly to atrial ischemia and AF. More commonly, severe ventricular ischemia leads to increased intra-atrial pressure and AF.
Inflammation
Myocarditis and pericarditis may be idiopathic or may occur in association with collagen vascular diseases; viral or bacterial infections; or cardiac, esophageal, or thoracic surgery.
Noncardiovascular respiratory causes
Pulmonary embolism, pneumonia, lung cancer, and hypothermia have been associated with AF.
Drug and alcohol use
Stimulants, alcohol, and cocaine can trigger AF. Acute or chronic alcohol use (ie, holiday or Saturday night heart, also known as alcohol-related cardiomyopathy) and illicit drug use (ie, stimulants, methamphetamines, cocaine) have been specifically found to be related to AF. Whereas the association of more than moderate chronic alcohol use and AF has been reported in multiple studies previously, a more recent community-based study found an association with even moderate alcohol use with an increased risk of AF. [22]
Endocrine disorders
Hyperthyroidism, diabetes, and pheochromocytoma have been associated with AF.
Neurologic disorders
Intracranial processes such as subarachnoid hemorrhage or stroke can precipitate AF.
Familial AF
A history of parental AF appears to confer increased likelihood of AF (and occasional family pedigrees of AF are associated with defined ion channel abnormalities, especially sodium channels). [23] One cohort study suggests that familial AF is associated with an increased risk of AF. This increase was not lessened by adjustment for genetic variants and other AF risk factors. [24]
Advancing age
AF is strongly age-dependent, affecting 4% of individuals older than 60 years and 8% of persons older than 80 years.
Other
In a 15-year prospective cohort study of 132,250 Japanese subjects, Xu et al found that anemia and chronic kidney disease, alone and in combination, were associated with an increased risk of new-onset AF. [25, 26] During a mean follow-up of 13.8 years in 1232 patients with new-onset AF, multivariate analysis showed that those with an estimated glomerular filtration rate (eGFR) lower than 60 mL/min/1.73 m2 were 2.56 times more likely to experience new-onset AF compared with patients with normal kidney function; those whose hemoglobin levels were lower than 13 g/dL had a 1.5 times increased risk of new-onset AF relative to patients with normal hemoglobin levels (P< 0.0001 for both analyses). [25, 26] Patients with CKD and anemia had a threefold higher incidence of AF. [26]
Epidemiology
Atrial fibrillation (AF) is the most frequently encountered cardiac arrhythmia. [19] It affects more than 2.7 to 6.1 million persons in the United States. [27] AF is strongly age-dependent, affecting 4% of individuals older than 60 years and 8% of persons older than 80 years. Approximately 25% of individuals aged 40 years and older will develop AF during their lifetime. [28]
The prevalence of AF is 0.1% in persons younger than 55 years, 3.8% in persons 60 years or older, and 10% in persons 80 years or older. With the projected increase in the elderly population in the United States, the prevalence of AF is expected to more than double by the year 2050. AF is uncommon in childhood except after cardiac surgery. [29]
The incidence of AF is significantly higher in men than in women in all age groups, although this effect may be mediated through the difference in average height between men and women. [30] AF appears to be more common in white individuals than in black persons, with black individuals have less than half the age-adjusted risk of developing AF.
In 10-15% of cases of AF, the disease occurs in the absence of comorbidities. However, AF is often associated with other cardiovascular diseases, including hypertension; heart failure; diabetes-related heart disease; ischemic heart disease; and valvular, dilated, hypertrophic, restrictive, and congenital cardiomyopathies. [28] The Atherosclerosis Risk in Communities (ARIC) Study suggests reduced kidney function and presence of albuminuria are strongly associated with AF. [31]
The rate of ischemic stroke in patients with nonrheumatic AF averages 5% a year, which is somewhere between 2 and 7 times the rate of stroke in patients without AF. The risk of stroke is not due solely to AF; it increases substantially in the presence of other cardiovascular diseases. [32] The prevalence of stroke in patients younger than 60 years is less than 0.5%; however, in those older than 70 years, the prevalence doubles with each decade. [33] The attributable risk of stroke from AF is estimated to be 1.5% for those aged 50-59 years, and it approaches 30% for those aged 80-89 years. Women are at a higher risk of stroke due to AF than men and some have suggested this may be due to undertreatment with warfarin. However, one study of patients 65 years or older with recently diagnosed AF found warfarin use played no part in the increased risk of stroke among female patients. [34]
Prognosis
Atrial fibrillation (AF) is associated with a 1.5- to 1.9-fold higher risk of death, which is in part due to the strong association between AF and thromboembolic events, according to data from the Framingham heart study. [35]
Medical therapies aimed at rhythm control offered no survival advantage over rate control and anticoagulation, according to the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) trial. The study addressed whether rate control and anticoagulation are sufficient goals for asymptomatic, elderly patients. [36]
AF is associated with increased morbidity and mortality, in part due to the risk of thromboembolic disease, particularly stroke, in AF and in part due to its associated risk factors. Studies have shown that individuals in sinus rhythm live longer than individuals with AF. Disruption of normal atrial electromechanical function in AF leads to blood stasis. This, in turn, can lead to development of thrombus, most commonly in the left atrial appendage. Dislodgement or fragmentation of a clot can then lead to embolic phenomena, including stroke.
Development of AF predicts heart failure and is associated with a worse New York Heart Association Heart Failure classification. AF may also worsen heart failure in individuals who are dependent on the atrial component of the cardiac output. Those with hypertensive heart disease and those with valvular heart disease are particularly at high risk for developing heart failure when AF occurs. In addition, AF may cause tachycardia-mediated cardiomyopathy if adequate rate control is not established.
In critically ill patients, new-onset AF is independently associated with in-hospital and post-ICU risk of death. [37]
Findings from the observational multicenter PLECTRUM study that evaluated the thromboembolic risk regarding the type and site of mechanical prosthetic heart valves, as well as the quality of anticoagulation and risk factors associated with thromboembolism, found that there was a low rate of bleeding and thromboembolic events in patients with these valves, even when anticoagulation control was suboptimal. [38] There was no association between the thromboembolic risk and low time in therapeutic range, but the presence of AF and a history of thromboembolism and of mitral prosthesis were independent risk factors for thromboembolism. [38]
In a systematic review (13 studies) and meta-analysis (10 eligible studies) of death and adverse outcomes in 54,587 patients with AF and concomitant heart failure, investigators reported a significantly higher all-cause mortality in AF patients with reduced ejection fraction compared to those with preserved ejection fraction. [39] However, the rates of stroke and hospitalizations were similar between the groups.
The risk of stroke from AF that lasts longer than 24 hours is a major concern and is usually addressed by prescribing a blood thinner (warfarin, dabigatran, rivaroxaban, apixaban, or edoxaban). The CHADS2 prognostic scoring system was originally derived to estimate the risk of ischemic stroke in patients with AF. A higher CHADS2 score implies a higher risk of ischemic stroke; in older guidelines, a CHADS2 score of 2 or greater was considered an indication for using blood thinners. [40] However, the CHADS2 score appears to underestimate the risk of embolic stroke in patients older than 75 years. [41] Furthermore the CHADS2 score does not include some of the other risk factors associated with ischemic stroke in AF patients, such as female sex and vascular disease.
An analysis of the AFNET (Central Registry of the German Competence NETwork on Atrial Fibrillation) registry of 8847 patients with nonvalvular AF indicated that the CHA2 DS2-VASc score is more sensitive than the CHADS2 score for risk stratification of thromboembolic events (ischemic stroke, transient ischemic attack [TIA], systemic embolism), particularly in patients with a CHADS2 score of 0 or 1 who would have otherwise not received prescribed anticoagulation therapy on the basis of previous guidelines. [42, 43] However, CHA2 DS2-VAScc scoring—which adds age 65-74 years, arterial disease, and female sex as stroke risk factors to the CHADS2 score [43] —placed 30.3% of those classified as CHADS2 0 or 1 into CHA2 DS2-VASc 1 or 2 and higher, groups in which oral anticoagulation is now recommended.
In another investigation of over 47,000 participants with a CHADS2 score of 0 to 1 who were not on anticoagulation therapy, Olesen et al reported a serial increase in the risk of stroke/thromboembolism with an increase in CHA2 DS2-VASc score. [44] Furthermore, a regression model with the CHA2 DS2-VASc score showed higher discrimination for predicting stroke than the model with the CHADS2 score. [44]
A post-hoc analysis of the ONTARGET and TRANSCEND studies, which evaluated the efficacy of treatment with ramipril plus telmisartan or telmisartan alone in reducing cardiovascular disease, used the Mini–Mental State Examination (MMSE) to measure the cognitive function of participants at baseline and after two and five years. Results show that AF is associated with an increased risk of cognitive decline, new dementia, loss of independence in performing activities of daily living and admission to long-term care facilities. [45]
Atrial fibrillation in association with acute myocardial infarction
AF is a common finding in patients presenting with an acute myocardial infarction. A meta-analysis pooled data from 43 studies and more than 278,800 patients. [46] The study found that AF in the setting of acute myocardial infarction was associated with 40% increase in mortality compared to patients in sinus rhythm with acute myocardial infarction. The causes of death were unclear, but may be related to triple anticoagulation therapy with aspirin, clopidogrel, and warfarin, or may be related to hemodynamic consequences associated with the loss of atrial contraction. Whether AF is a complication of myocardial infarction or a marker for myocardial infarction severity is unclear.
A study by van Diepen et al suggests that patients with heart failure or atrial fibrillation have a significantly higher risk of noncardiac postoperative mortality than patients with coronary artery disease; thus, patients and physicians should consider this risk, even if a minor procedure is planned. [47]
Catheter ablation in association with mortality and stroke
A systemic review and meta-analysis comprising 30 studies and 78,966 patients (about one third receiving AF ablation and two thirds on medical therapy) with 233,990 patient-years of follow-up found a survival benefit for AF ablation relative to medical treatment alone, but these findings were only supported in the setting of heart faiure and left ventricular systolic dysfunction. [48]
-
Ventricular rate varies from 130-168 beats per minute. Rhythm is irregularly irregular. P waves are not discernible.
-
Classification scheme for patients with atrial fibrillation (AF).
-
Patient management for newly diagnosed atrial fibrillation (Afib). *Therapeutic anticoagulation implies either treatment with warfarin with a therapeutic international normalized ratio (INR) (2-3) or with newer oral anticoagulants (dabigatran, rivaroxaban, apixaban, or edoxaban). Transesophageal echocardiography (TEE)/cardioversion should be performed with an anticoagulation strategy using either low molecular-weight heparin (LMWH) 1 mg/kg twice daily as a bridge, with initiation of warfarin (INR 2-3) or newer oral anticoagulants.
-
Antiarrhythmic drug algorithm for the medical management of sinus rhythm in patients with atrial fibrillation.
-
The image on the right is a reconstructed 3-dimensional image of the right atrium in a patient undergoing atrial fibrillation ablation. The figure on the left was created with a mapping catheter using Endocardial Solutions mapping technology. It represents the endocardial shell of the right atrium and is used as the template during left atrial ablation procedures.
Tables
- Table 1. Stroke Rate in Patients with Nonvalvular Atrial Fibrillation not Treated with Anticoagulation [67]
- Table 2. Recommendations for Antithrombotic Therapy in Patients with Nonvalvular Atrial Fibrillation
- Table. Antithrombotic Therapy Recommendations for Atrial Fibrillation
- Table. Medications, Strategies, and Techniques Specified or Not Mentioned in the 2019 Guidelines
CHA2 DS2-VASc Score |
Unadjusted Stroke Rate (%/y) |
0 |
0.2 |
1 |
0.6 |
2 |
2.2 |
3 |
3.2 |
4 |
4.8 |
5 |
7.2 |
6 |
9.7 |
7 |
11.2 |
8 |
10.8 |
9 |
12.2 |
CHA2 DS2-VASc Score |
Recommended Therapy |
| 0 | No therapy |
| 1 | No therapy, or aspirin 81-325 mg daily, or anticoagulation therapy (eg, warfarin [international normalized ratio (INR) goal 2-3], dabigatran, rivaroxaban, apixaban, edoxaban) |
≥2 |
Anticoagulation therapy (eg, warfarin [INR goal 2-3], dabigatran, rivaroxaban, apixaban, edoxaban) |
| Issuing Organization | Year | Patient Groups | Antithrombotic Therapy |
|---|---|---|---|
| American Heart Association/American College of Cardiology/ Heart Rhythm Society (AHA/ACC/HRS) [1] | 2014 |
|
|
| American Heart Association/American Stroke Association (AHA/ASA) [151] | 2014 |
|
|
| American Academy of Neurology (AAN) [97] | 2014 |
|
|
| American College of Chest Physicians (ACCP) [150] | 2012 | NVAF intermediate risk (CHADS2 score = 1) or high risk (CHADS2 score ≥2) |
|
| European Society of Cardiology (ESC) [149] | 2012 |
|
|
Note: Edoxaban was approved by the FDA in January 2015 for use as an oral anticoagulant in atrial fibrillation. AF = atrial fibrillation; BID = twice daily; CKD = chronic kidney disease; CrCl = creatinine clearance; INR = international normalized ratio; LMWH = low-molecular-weight heparin; NVAF = nonvalvular atrial fibrillation; OD = before bedtime; TIA = transient ischemic attack. |
|||
Type of Tachycardia |
Treatment (Grade) |
Not Mentioned in 2019 Guidelines |
Narrow QRS tachycardias |
Verapamil and diltiazem; beta-blockers (now all are grade IIa) |
Amiodarone, digoxin |
Wide QRS tachycardias |
Procainamide, adenosine (both grade IIa); amiodarone (IIb) |
Sotalol, lidocaine |
Inappropriate sinus tachycardia |
Beta-blockers (IIa) |
Verapamil/diltiazem, catheter ablation |
Postural orthostatic tachycardia syndrome |
Salt and fluid intake (IIb) |
Head-up tilt sleep, compression stockings, selective beta-blockers, fludrocortisone, clonidine, methylphenidate, fluoxetine, erythropoietin, ergotaminel octreotide, phenobarbitone |
Focal atrial tachycardia |
Acute: beta-blockers (IIa); flecainide/propafenone, amiodarone (IIb) |
Acute: procainamide, sotalol, digoxin |
Chronic: beta-blockers; verapamil and diltiazem (all IIa) |
Chronic: amiodarone, sotalol, disopyramide |
|
Atrial flutter |
Acute: ibutilide (I); verapamil and diltiazem, beta-blockers (all IIa); atrial or transesophageal pacing (IIb); flecainide/propafenone (III) |
Acute: digitalis |
Chronic: — |
Chronic: dofetilide, sotalol, flecainide, propafenone, procainamide, quinidine, disopyramide |
|
Atrioventricular nodal re-entrant tachycardia (AVNRT) |
Acute: — |
Acute: amiodarone, sotalol, flecainide, propafenone |
Chronic: verapamil and diltiazem; beta-blockers (all IIa) |
Chronic: amiodarone, sotalol, flecainide, propafenone, “pill-in-the-pocket” approach |
|
Atrioventricular re-entrant tachycardia (AVRT) |
Beta-blockers (IIa); flecainide/propafenone (IIb) |
Amiodarone, sotalol, “pill-in-the-pocket” approach |
SVT in pregnancy |
Verapamil (IIa); catheter ablation (IIa when fluoroless ablation is available) |
Sotalol, propafenone, quinidine, procainamide |
Adapted from Brugada J, Katritsis DG, Arbelo E, et al, for the ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2019 Aug 31;ehz467. https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehz467/5556821 |
||

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Approach Considerations
- Risk-Management Decisions
- Management of New-Onset AF
- Long-Term Management
- Overview of Surgical and Catheter Ablation
- Compartmentalization of the Atria
- Catheter Ablation of Focal Triggers of AF
- AV Node Modification and Permanent Pacemakers
- Left Atrial Appendage Percutaneous Closure
- Consultations
- Long Term Monitoring
- Show All
- Guidelines
- Atrial Fibrillation Classification
- Stroke Risk Assessment
- Antithrombotic Therapy
- Rate Control
- Cardioversion
- Maintaining Sinus Rhythm
- Catheter Ablation
- Supraventricular Arrhythmias Guidelines
- 2019 ESC/AEPC Guidelines for the Management of Supraventricular Tachycardia
- 2017 EHRA Consensus Document on the Management of Supraventricular Arrhythmias
- Resources
- Show All
- Medication
- Questions & Answers
- Media Gallery
- Tables
- References




