Background
According to the American Psychiatric Association (APA), anxiety disorders are the most common type of psychiatric disorders. [1] Many patients with anxiety disorders experience physical symptoms related to anxiety and subsequently visit their primary care providers. Despite the high prevalence rates of these anxiety disorders, they often are underrecognized and undertreated clinical problems.
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), [2] anxiety disorders include disorders that share features of excessive fear and anxiety and related behavioral disturbances. These disorders include separation anxiety disorder, selective mutism, specific phobia, social anxiety disorder, panic disorder, agoraphobia, generalized anxiety disorder, substance/medication-induced anxiety disorder, and anxiety disorder due to another medical condition. Obsessive-compulsive disorder (included in the obsessive-compulsive and related disorders), acute stress disorder, and posttraumatic stress disorder (included in the trauma and stress-related disorders) are no longer considered anxiety disorders as they were in the previous version of the DSM. However, these disorders are closely related to anxiety disorders and the sequential order of these chapters in the DSM-5-TR reflects this close relationship.
Anxiety disorders appear to be caused by an interaction of biopsychosocial factors, including genetic vulnerability, which interact with situations, stress, or trauma to produce clinically significant syndromes. (See Pathophysiology and Etiology.)
Symptoms vary depending on the specific anxiety disorder. (See Clinical Presentation.)
Treatment usually consists of a combination of pharmacotherapy (see Medication), psychotherapy, and/or healthy lifestyle interventions. (See Treatment Strategies and Management.)
Anatomy
The brain circuits and regions associated with anxiety disorders are beginning to be understood with the development of functional and structural imaging. The amygdala appears to play a pivotal role in modulating fear of imminent threats and anxiety in anticipation of future threats. Patients with anxiety disorders often show heightened amygdala response to anxiety cues in such imaging studies. [3] The amygdala and other limbic system structures are connected to prefrontal cortex regions. Hyperresponsiveness of the amygdala may relate to reduced activation thresholds when responding to perceived social threat. [4, 5] Abnormal activations in the amygdala appear to be reversible with clinical responses to psychological or pharmacological treatments. [6]
Pathophysiology
In the central nervous system (CNS), the major mediators of the symptoms of anxiety disorders appear to be norepinephrine, serotonin, dopamine, and gamma-aminobutyric acid (GABA). Other neurotransmitters and peptides, such as corticotropin-releasing factor, may be involved in the hypothalamic-pituitary-adrenal (HPA) axis. [7] Peripherally, the autonomic nervous system, especially the sympathetic nervous system, mediates many of the symptoms. [8] Positron emission tomography (PET) scanning has demonstrated increased flow in the right parahippocampal region in those with anxiety disorders that is reversible with treatment. [9] Those with anxiety disorders also appear to have reduced serotonin type 1A receptor binding in the anterior and posterior cingulate and raphe of patients with panic disorder. [10, 11] In patients with panic disorder in particular, MRI has demonstrated smaller temporal lobe volume despite normal hippocampal volume. [12, 13] CSF studies in humans show elevated levels of orexin, also known as hypocretin, which is thought to play an important role in the pathogenesis of panic in rat models. [14]
Etiology
Anxiety disorders in general
The first consideration is the possibility that anxiety is due to a known or unrecognized medical condition. Substance-induced anxiety disorder (over-the-counter medications, herbal medications, substances of abuse) is a diagnosis that often is missed.
Genetic factors significantly influence risk for many anxiety disorders. Environmental factors such as trauma, neglect, chaos, or Adverse Childhood Experiences (ACEs) [15] can also contribute to risk for later anxiety disorders. The debate whether gene or environment is primary in anxiety disorders has evolved to a better understanding of the important role of the interaction between genes and environment. [16] Some individuals appear resilient to stress, while others are vulnerable to stress, which precipitates an anxiety disorder.
Most presenting anxiety disorders are functional psychiatric disorders. Psychological theories range from explaining anxiety as a displacement of an intrapsychic conflict (psychodynamic models) to conditioning (learned) paradigms (cognitive-behavioral models). Many of these theories capture portions of the disorder.
The psychodynamic theory has explained anxiety as a conflict between the id and ego. Aggressive and impulsive drives may be experienced as unacceptable resulting in repression. These repressed drives may break through repression, producing automatic anxiety. The treatment uses exploration with the goal of understanding the underlying conflict. Cognitive theory has explained anxiety as the tendency to overestimate the potential for danger. Patients with anxiety disorder tend to imagine the worst possible scenario and avoid situations they think are dangerous, such as crowds, heights, or social interaction.
Panic disorder
Panic disorder appears to be a genetically inherited (heritability of 40% [17] ) neurochemical dysfunction that may involve autonomic imbalance; decreased GABA-ergic tone; [18] allelic polymorphism of the catechol-O-methyltransferase (COMT) gene; increased adenosine receptor function; increased cortisol; [19] diminished benzodiazepine receptor function; and disturbances in serotonin, [20, 21] serotonin transporter (5-HTTLPR) [22] and promoter (SLC6A4) genes, [23] norepinephrine, dopamine, cholecystokinin, and interleukin-1-beta. [24] Some theorize that panic disorder may represent a state of chronic hyperventilation and carbon dioxide receptor hypersensitivity. [25, 26] Some epileptic patients have panic as a manifestation of their seizures. Genetic studies suggest that the chromosomal regions 13q, 14q, 22q, 4q31-q34, and probably 9q31 may be associated with the heritability of panic disorder phenotype. [17]
The cognitive theory regarding panic is that patients with panic disorder have a heightened sensitivity to internal autonomic cues (eg, tachycardia). Triggers of panic can include the following:
-
Injury (eg, accidents, surgery)
-
Illness
-
Interpersonal conflict or loss
-
Use of stimulants, such as caffeine, decongestants, cocaine, and sympathomimetics (eg, amphetamine, MDMA ["ecstasy"]) [29]
-
Certain settings, such as stores and public transportation (especially in patients with agoraphobia)
-
A case report found sertraline can trigger panic attacks in those who were previously symptom-free. [30]
-
The SSRI discontinuation syndrome can induce symptoms similar to those experienced by panic patients. [31]
In experimental settings, symptoms can be elicited in people with panic disorder by hyperventilation, inhalation of carbon dioxide, caffeine consumption, or intravenous infusions of hypertonic sodium lactate or hypertonic saline, [32] cholecystokinin, isoproterenol, flumazenil, [33] or naltrexone. [34] The carbon dioxide inhalation challenge is especially provocative of panic symptoms in smokers. [35]
Social anxiety disorder
The term “social phobia” was removed from DSM-5-TR in 2022.
Genetic factors seem to play a role in social anxiety disorder. Based on family and twin studies, the risk for social anxiety disorder appears to be moderately heritable. [36, 37]
Social anxiety disorder can be initiated by traumatic social experience (eg, embarrassment) or by social skills deficits that produce recurring negative experiences. A hypersensitivity to rejection, perhaps related to serotonergic or dopaminergic dysfunction, is present. Current thought is that social anxiety disorder appears to be an interaction between biological and genetic factors and environmental events.
A psychoanalyst would likely conceptualize social anxiety as a symptom of a deeper conflict, for instance, low self-esteem or unresolved conflicts with internal objects. A behaviorist would see phobia as a learned conditioned response resulting from a past association with a situation with negative emotional valence at the time of association (eg, social situations are avoided because intense anxiety was originally experienced in that setting). Even if no danger is posed in most social encounters, an avoidance response has been linked to these situations. Treatment from this perspective aims to weaken and eventually separate the specific response from the stimulus.
Specific phobia
Genetic factors seem to play a role in specific phobia as well (eg, the most common being zoophobia, the fear of animals [38] ), and the risk for such phobias also seems to be moderately heritable. [36] In addition, specific phobia can be acquired by conditioning, modeling, or traumatic experience.
Agoraphobia
Agoraphobia may be the result of repeated, unexpected panic attacks, which, in turn, may be linked to cognitive distortions, conditioned responses, and/or abnormalities in noradrenergic, serotonergic, or GABA-related neurotransmission.
Epidemiology
United States statistics
Anxiety disorders are the most common type of psychiatric disorders in the United States. The lifetime prevalence of anxiety disorders among American adults is 28.8%. [39]
While specific phobias are the most common anxiety disorders, social anxiety disorder is the second most common anxiety disorder and presents more commonly for treatment than specific phobias do. Social anxiety disorder has an early age of onset—by age 11 years in about 50% and by age 20 years in about 80% of individuals that have the diagnosis—and it is a risk factor for subsequent depressive illness and substance abuse. [40]
According to the DSM-5-TR, [2] the 12-month community prevalence estimate for specific phobia is approximately 8–12% in the United States. The 12-month prevalence estimate of social anxiety disorder for the United States is approximately 7%. The 12-month prevalence of generalized anxiety disorder is 0.9% among adolescents and 2.9% among adults in the United States. The 12-month prevalence estimate for panic disorder across the United States and several European countries is about 2–3% in adults and adolescents. The prevalence of agoraphobia is approximately 1–1.7% of adolescents and adults worldwide.
International statistics
The prevalence of specific anxiety disorders appears to vary between countries and cultures. A systematic review of the current prevalence of anxiety disorders in 89 countries found significant variation ranging from 0.9% in China to 28.3% in Afghanistan. [41] As an example, in the United States the prevalence of social anxiety disorder is approximately 7%, while in Europe it is 2.3%. [2]
Cross-cultural factors need to be considered. In some Far East cultures, individuals with social anxiety disorder may develop fears of being offensive to others rather than fears of being embarrassed. In Japan and Korea, this syndrome is referred to as taijin kyofusho. [2]
Prevalence of anxiety disorders by race
Respondents who were White, Native American, or Hispanic/Latino were more likely to be diagnosed with an anxiety disorder compared to those who were African American. [42]
Sex ratio for anxiety disorders
The female-to-male ratio for any lifetime anxiety disorder is 3:2 (see the image below).
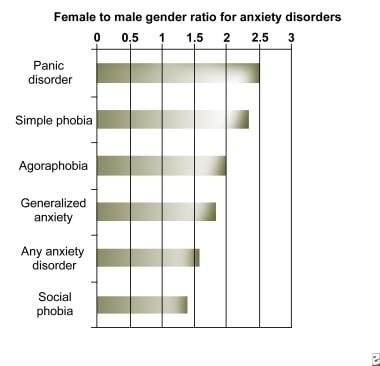 Anxiety. Chart showing the female-to-male sex ratio for anxiety disorders. Adapted from Kessler et al, 1994.
Anxiety. Chart showing the female-to-male sex ratio for anxiety disorders. Adapted from Kessler et al, 1994.
Age distribution for anxiety disorders
Most anxiety disorders begin in childhood, adolescence, and early adulthood (see the image below). Separation anxiety is an anxiety disorder that commonly begins in childhood and during adolescence but can uncommonly begin during adulthood. [2] It often includes anxiety related to going to school and may be a precursor for adult anxiety disorders, most commonly panic disorder.
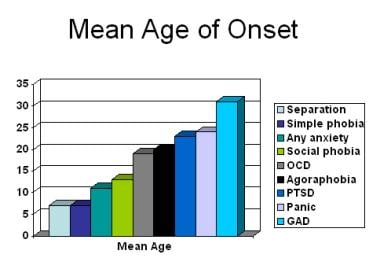 Anxiety. Age of onset for anxiety disorders based on specific anxiety disorder type.
Anxiety. Age of onset for anxiety disorders based on specific anxiety disorder type.
Panic disorder demonstrates a bimodal age of onset in the NCS study [39] in the age groups of 15–24 years and 45–54 years. The age of onset for OCD appears to be in the mid-20s to early 30s.
Most social anxiety disorders begin before age 20 years (median age at illness onset, 16 years [43] ).
Agoraphobia usually begins in late adolescence to early adulthood (median age at illness onset, 29 years [43] ).
In general, specific phobia appears earlier than social anxiety disorder or agoraphobia. The age of onset depends on the particular phobia. For example, animal phobia is most common at the elementary school level and appears at a mean age of 7 years; blood phobia appears at a mean age of 9 years; dental phobia appears at a mean age of 12 years; and claustrophobia appears at a mean age of 20 years. Most simple (specific) phobias develop during childhood (median age at illness onset, 15 years) [43] and eventually disappear. Those that persist into adulthood rarely go away without treatment.
New-onset anxiety symptoms in older adults should prompt a search for an unrecognized general medical condition, a substance abuse disorder, or major depression with secondary anxiety symptoms.
Prognosis
Anxiety disorders have high rates of comorbidity with major depression and alcohol and drug abuse. Some of the increased morbidity and mortality associated with anxiety disorders may be related to this high rate of comorbidity. Anxiety disorders may contribute to morbidity and mortality through neuroendocrine and neuroimmune mechanisms or by direct neural stimulation (eg, hypertension or cardiac arrhythmia). Chronic anxiety may be associated with increased risk for cardiovascular morbidity and mortality.
Considerable evidence shows that social anxiety disorder results in significant functional impairment and decreased quality of life. [44, 45]
Severe anxiety disorders may be complicated by suicide, with or without secondary mood disorders (eg, depression). The Epidemiological Catchment Area study found that panic disorder was associated with suicide attempts (odds ratio = 18 compared with populations without psychiatric disorders). How much of the association of panic disorder with suicide is mediated through the association of panic disorder with mood and substance abuse disorders is unclear. Acute stress may play a role in producing suicidal behavior. The presence of any anxiety disorder, phobias included, in combination with a mood disorder appears to increase likelihood of suicide attempts compared with a mood disorder alone. [46] Suicide attempts can be precipitated by adverse life events such as divorce or financial disaster. The effects of acute stress in producing suicidal behavior are increased in those with underlying mood, anxiety, and substance abuse problems.
Phobias are highly comorbid. Most comorbid specific phobias and social anxiety disorders are temporally primary, while most comorbid agoraphobia is temporally secondary. Comorbid phobias are generally more severe than pure phobias. Social anxiety disorder is also frequently comorbid with major depressive disorder and atypical depression, which results in increased disability. [45, 47] Despite evidence of impairment, only a minority of individuals with specific phobia ever seek professional treatment.
Interestingly, in clinical samples, more than 95% of the patients reporting agoraphobia also present with panic disorder, while in epidemiologic samples, simple agoraphobia appears to be more prevalent than panic disorder with agoraphobia. [48]
Patient Education
Education can be obtained through books, newsletters, support groups, and the Internet. Some useful Web sites are as follows:
-
National Institute of Mental Health, Anxiety Disorders
-
SAMHSA’s National Mental Health Information Center, Anxiety Disorders
-
eMedicineHealth, Mental Health Center
-
eMedicineHealth, Stress, Anxiety Disorders, Panic Attacks, and Hyperventilation
Family members should receive information about the effect of anxiety disorders on mood, behavior, and relationships. Family members can assist in care by reinforcing the need for medical treatment and supervision. Family members may also assist by providing a collaborative resource for monitoring the severity of the patient’s anxiety symptoms and response to treatment interventions.
-
Anxiety. Chart showing the female-to-male sex ratio for anxiety disorders. Adapted from Kessler et al, 1994.
-
Anxiety. Age of onset for anxiety disorders based on specific anxiety disorder type.
-
Brain structures involved in dealing with fear and stress.







