Overview of Multifocal Atrial Tachycardia
Multifocal atrial tachycardia (MAT) is a cardiac arrhythmia caused by multiple sites of competing atrial activity. It is characterized by an irregular atrial rate greater than 100 beats per minute (bpm). Atrial activity is well organized, with at least 3 morphologically distinct P waves, irregular P-P intervals, and an isoelectric baseline between the P waves. [1]
Shine, Kastor and Yurchak first proposed this definition of MAT in 1968. [2] MAT has previously been described by terms such as chaotic atrial rhythm or tachycardia, chaotic atrial mechanism, and repetitive paroxysmal MAT.
Usually, treatment of the patient's underlying problem (eg, respiratory failure, sepsis, theophylline toxicity) takes therapeutic precedent. The condition is transient and resolves when the underlying condition improves. [1]
For more information, see Atrial Tachycardia
Pathophysiology of MAT
The mechanism of the arrhythmia has not been well defined. Delayed afterdepolarizations leading to triggered automaticity are postulated to result in the development of multifocal atrial tachycardia (MAT). The evidence that implicates this mechanism is mainly indirect and points to intracellular calcium overload by various mechanisms (eg, catecholamine excess, phosphodiesterase inhibition, acidosis, hypoxemia). Electrolyte imbalances associated with severe underlying illnesses can further potentiate the development of this arrhythmia. MAT most often is found in the elderly patient with decompensated chronic lung disease and should be thought of as a hypoxic complication of underlying heart conduction pathology. However, other underlying causes may be present, such as heart failure, sepsis, or methylxanthine toxicity. The effect of MAT on the heart’s conduction system may or may not lead to hemodynamic instability.
Etiology of MAT
Causes of multifocal atrial tachycardia (MAT) are mainly related to underlying illnesses. The following common underlying illnesses are associated with this arrhythmia:
-
Decompensated chronic lung disease
-
Coronary artery disease
-
Valvular heart disease
-
Diabetes mellitus
-
Postoperative state
-
Pneumonia
-
Sepsis
-
Methylxanthine toxicity (theophylline toxicity)
Epidemiology of MAT
Multifocal atrial tachycardia (MAT) is a relatively infrequent arrhythmia, with a prevalence rate of 0.05-0.32% in patients who are hospitalized. It is predominantly observed in males and in older patients—in particular, elderly patients with multiple medical problems. The average age of patients from 9 studies was 72 years.
Patients with MAT frequently have significant comorbidities, especially chronic obstructive pulmonary disease (COPD) and respiratory failure, and are often treated in ICUs. Consequently, a high mortality rate (ie, up to 45%) is associated with this arrhythmia, although it is not a direct consequence of the rhythm abnormality.
MAT is seldom life threatening. The overall clinical picture and symptoms improve when the underlying condition is addressed and MAT is controlled. Morbidity is difficult to quantify because the underlying disease is the primary determinant of complications.
Clinical Presentation
Patient history
Patients may complain of a variety of symptoms, or more rarely, the disease may be asymptomatic. The most common complaints include the following:
-
Palpitations
-
Shortness of breath
-
Chest pain
-
Lightheadedness
-
Syncopal episode
These symptoms may be transient.
Physical examination
Physical examination findings are typically related to the underlying disease process and are not specific for MAT. The pulse is rapid and irregular, [3] and the first heart sound may be variable. The physical examination is not typically sufficient to differentiate multifocal atrial tachycardia from atrial fibrillation. Respiratory adventitial sounds often are prominent.
Depending upon comorbid conditions or general health status, the patient may be hemodynamically unstable. However, determining whether this is due to the underlying condition or the dysrhythmia may be difficult.
Complications
Potential acute complications of MAT include the following:
-
Atrial thrombi with embolization and subsequent stroke
-
Myocardial infarction from incongruous myocardial supply and demand
-
Pulmonary emboli
Underlying disorders
COPD is the most common underlying disease process, seen in approximately 60% of MAT cases. MAT is commonly precipitated by exacerbation of COPD, sometimes due to infection or cardiac decompensation. Increasing hypoxemia with respiratory acidosis and advanced disease also leads to increased bronchodilator usage, thereby increasing catecholamine levels, which may contribute to development of MAT.
Patients with MAT frequently have cardiac diseases, mainly coronary artery disease and valvular heart diseases, often in conjunction with COPD. [4] Heart failure is often present when the diagnosis of MAT is first made.
In various series, 24% of patients with MAT were found to have diabetes mellitus. Fourteen percent had hypokalemia, and 14% had azotemia. Twenty-eight percent of patients with MAT were recovering from major surgery, while others had postoperative infections, sepsis, pulmonary embolism, and heart failure.
The link between pulmonary embolism and MAT is weak (ie, 6-14% of such patients have been said to have MAT), but the methods of diagnosing pulmonary embolism have not been well documented.
Experimental evidence demonstrates that IV cocaine use may lead to the development of MAT.
Differential Diagnosis
The differential diagnosis of MAT includes atrial fibrillation and atrial flutter. Clear differentiation of multifocal atrial tachycardia (MAT) from atrial fibrillation is very important because the treatment of atrial fibrillation differs from that of MAT. MAT with aberration or preexisting bundle branch block may be misinterpreted as ventricular tachycardia. MAT must also be differentiated from other tachyarrhythmias, both narrow-complex and wide-complex, including sinus tachycardia with frequent premature atrial contractions (PACs).
Electrocardiography
The diagnosis of multifocal MAT is confirmed with an electrocardiogram (ECG) that displays the following features (see the image below):
-
Irregular ventricular rate greater than 100 bpm
-
Organized and discrete P waves with at least 3 different morphologies in the same electrocardiographic lead
-
Irregular PP, PR, and RR intervals with an isoelectric baseline between the P waves
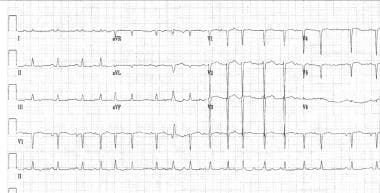 ECG showing multifocal atrial tachycardia (MAT).
ECG showing multifocal atrial tachycardia (MAT).

Some authors have suggested that patients who have a heart rate less than 100 bpm but who satisfy all other criteria (including the clinical profile commonly observed with MAT) be considered to have multifocal atrial rhythm, or multifocal atrial bradycardia if the rate is less than 60 bpm. There is controversy about whether this condition should be referred to as a MAT variant or a wandering atrial pacemaker, although patients with wandering atrial pacemaker usually do not have serious underlying illnesses.
The requirement that 3 different P waves should exist has been applied since early descriptions of the arrhythmia were recorded, but whether this should be interpreted as 2 ectopic P waves and 1 sinus P wave or 3 ectopic P waves has been a matter of controversy. The consensus favors a minimum of 3 different waveforms in addition to sinus P waves.
Baseline noise on the ECG can mimic atrial fibrillation and can obscure differences in P wave morphology. Conversely, coarse atrial fibrillation on short recordings may appear to show discrete P waves prior to each QRS complex. Longer ECG recordings are therefore useful.
Laboratory Studies
Laboratory testing mainly consists of the following:
-
Serum chemistry panel to exclude electrolyte disorders
-
Blood hemoglobin level and red blood cell (RBC) counts to seek evidence of anemia
-
Arterial blood gases to define pulmonary status
Any further testing depends on the underlying disease process (eg, cardiac biomarkers in patients with coronary artery disease, or a theophylline level if patient has been prescribed, or has access to, this medication).
Other Tests
Consider a portable anteroposterior (AP) chest radiograph to evaluate for pulmonary and cardiac findings, particularly in the unstable patient. All patients should be placed on pulse oximetry and a cardiac monitor.
Treatment of MAT
Prehospital care
The following measures should be taken in the prehospital setting:
-
Assess for potential pulmonary causes of the arrhythmia
-
Stabilize the acute situation as necessary
-
Provide oxygen, cardiac monitoring, and pulse oximetry
-
Establish IV access without delaying transport
-
Collect medications that the patient may be taking or may have access to
Emergency department care
Rapidly assess and stabilize the ABCs while providing simultaneous treatment. An upright sitting position usually is most appropriate. Obtain IV access with a large-bore catheter and give isotonic sodium chloride solution at a to-keep-open (TKO) rate.
Administer oxygen to maintain the saturation greater than 90%, but avoid excessive oxygen in patients with known significant chronic obstructive pulmonary disease (COPD). This will avoid the theoretical problem of removing the hypoxic drive for ventilation, which can result in increased carbon dioxide retention.
The need for tracheal intubation is dictated by the standard clinical indications.
Establish cardiac monitor, blood pressure monitor, and pulse oximetry.
Assess for and treat the underlying cardiopulmonary process, theophylline toxicity, or metabolic abnormality. Administer bronchodilators and oxygen for treatment of decompensated COPD; activated charcoal and/or charcoal hemoperfusion is the therapy for theophylline toxicity. When magnesium sulfate is administered to correct hypokalemia, most patients convert to normal sinus rhythm. Avoid sedatives.
Treatment and/or reversal of the precipitating cause may be all that is required for patients with multifocal atrial tachycardia (MAT); however, the arrhythmia may recur if the underlying condition worsens. Moreover, treatment of underlying diseases may sometimes have arrhythmia-promoting effects; for example, theophylline and beta-agonist drugs used in patients with COPD produce an increased catecholamine state. These therapies should be used judiciously.
Calcium channel blockers
Diltiazem [5] and verapamil [6, 7, 8, 9, 10, 11] decrease the atrial activity and slow atrioventricular (AV) nodal conduction, thereby decreasing ventricular rate, but they do not return all patients to normal sinus rhythm. Transient hypotension is the most common adverse effect, which may often be avoided by pretreating the patient with 1 g of intravenous calcium gluconate (10 mL of 10% calcium gluconate).
Diltiazem may be used as a 20-45 mg intravenous bolus and then as a 10-25 mg/h continuous infusion. Verapamil may worsen hypoxemia by negating the hypoxic pulmonary vasoconstriction in underventilated alveoli; this is usually not clinically significant.
Beta-blockers
More patients convert to a normal sinus rhythm when treated with beta-blockers. However, the use of beta-blockers is limited by transient hypotension and by bronchospastic adverse effects, since lung disease is commonly associated with MAT.
Metoprolol [8, 10, 12, 13, 14] has been used to lower the ventricular rate. Both oral and intravenous dosage forms have been used. The oral dosage is 25 mg q6h until the desired effects are obtained. Intravenous bolus dosing has been administered to as much as 15 mg over 10 minutes.
Although no controlled studies have evaluated the use of short-acting beta-blockers in treatment of MAT, esmolol can also be used to control the ventricular rate as an intravenous infusion. It has a very short half-life and can be terminated quickly in the event of an adverse reaction.
Magnesium
In a small number of patients, high-dose magnesium [8, 15, 16, 17, 18] causes a significant decrease in the patient's heart rate and conversion to normal sinus rhythm. The dosage is 2 g intravenously over 1 minute, followed by 2 g/h infusion over 5 hours.
Antiarrhythmics
Amiodarone [19, 20, 21] (300 mg PO tid or 450-1500 mg IV over 2-24 h) has been used and has been reported to be associated with conversion to normal sinus rhythm. The success rate was 40% at 3 days with oral dosing and 75% on day 1 with intravenous dosing; however, this has been evaluated in a very small number of patients. Recent data support the use of amiodarone prophylactically postoperatively in patients with COPD. Case reports have also supported the use of ibutilide [22] and flecainide [23] for cardioversion.
Digitalis
Despite the urge to use digoxin, it has not been found to be effective in controlling the ventricular rate or restoring normal sinus rhythm. Digoxin promotes afterdepolarizations, which may promote the arrhythmia. Ventricular arrhythmias, AV block, and death have been reported when excessive digoxin has been administered to patients who were incorrectly diagnosed with atrial fibrillation.
Cardioversion
Cardioversion is contraindicated in MAT. Due to the multiple atrial foci, direct current (DC) cardioversion is not effective in restoring normal sinus rhythm and can precipitate more dangerous arrhythmias.
Surgical care
In patients who have persistent and recurrent episodes of MAT and problems with rate control, the AV node may be ablated using radiofrequency energy and a permanent pacemaker implanted. [24] This approach should be considered both for symptomatic and hemodynamic improvement and to prevent the development of tachycardia-mediated cardiomyopathy.
Consultations
A cardiologist may be of assistance with ECG interpretation and may be available for consultation if antiarrhythmic therapy is being considered.
Inpatient care
Most patients with MAT require admission to further manage their underlying cardiopulmonary diseases. These patients frequently are admitted to a monitored bed; however, the clinical scenario and the hemodynamic stability of the patient dictate disposition.
Further outpatient care
Patients who convert to normal sinus rhythm after treatment and stabilization of the underlying process or provision of specific antiarrhythmic therapy may be cautiously considered for discharge. In order to be discharged, the patient must be back to baseline condition, have no complicating factors, be able to accomplish activities of daily living, and be available for close follow-up care.
Deterrence/prevention
The best means of prevention of MAT is prevention of respiratory failure plus careful monitoring of all electrolyte disorders, namely, hypokalemia, hypomagnesemia, and drug therapy (mainly digoxin toxicity). In patients receiving theophylline, careful monitoring of drug levels is important in order to avoid toxicity.
Patient education
Education about the causes of this arrhythmia may be beneficial. In the case of a pulmonary source, education about prevention and recognition of developing pulmonary conditions may be helpful. In the case of MAT related to medication use, education regarding the correct use and how to monitor such medications should be considered.
-
ECG showing multifocal atrial tachycardia (MAT).





