Uncontrolled Blood Pressure
Hypertensive emergencies encompass a spectrum of clinical presentations in which uncontrolled blood pressures (BPs) lead to progressive or impending end-organ dysfunction. In these conditions, the BP should be lowered aggressively over minutes to hours.
Neurologic end-organ damage due to uncontrolled BP may include hypertensive encephalopathy, cerebral vascular accident/cerebral infarction, subarachnoid hemorrhage, and/or intracranial hemorrhage. [1] Cardiovascular end-organ damage may include myocardial ischemia/infarction, acute left ventricular dysfunction, acute pulmonary edema, and/or aortic dissection. Other organ systems may also be affected by uncontrolled hypertension, which may lead to acute renal failure/insufficiency, retinopathy, eclampsia, or microangiopathic hemolytic anemia. [1]
With the advent of antihypertensive agents, the incidence of hypertensive emergencies in the United States has declined from 7% to approximately 1% of patients with hypertension. [2] In addition, the 1-year survival rate associated with this condition has increased from only 20% (prior to 1950) to a survival rate of more than 90% with appropriate medical treatment. [3] Nonetheless, despite its relative rarity, the number of US emergency department (ED) visits for hypertensive emergency and the rate per million adult ED visits increased more than two-fold between 2006 and 2013. [4]
History and physical examination
The history and the physical examination determine the nature, severity, and management of the hypertensive event. The history should focus on the presence of end-organ dysfunction, the circumstances surrounding the hypertension, and any identifiable etiology.
The most common clinical presentations of hypertensive emergencies are cerebral infarction (24.5%), pulmonary edema (22.5%), hypertensive encephalopathy (16.3%), and congestive heart failure (12%). Other clinical presentations associated with hypertensive emergencies include intracranial hemorrhage, aortic dissection, and eclampsia, [5] as well as acute myocardial infarction, and retinal and renal involvement. [6]
In pregnant patients, acute hypertensive crisis usually results from underlying hypertensive disease or severe preeclampsia [7] and can lead to maternal stroke, cardiopulmonary decompensation, fetal decompensation caused by reduced uterine perfusion, abruption, and stillbirth. [8] Preeclampsia may also complicated by pulmonary edema. [9]
The duration and severity of the patient’s preexisting hypertension (including the degree of BP control) should be evaluated, as well as the patient's medication history. Details of antihypertensive drug therapy and compliance, intake of over-the-counter (OTC) preparations such as sympathomimetic agents, and use of illicit drugs such as cocaine are important elements of the medication history. In addition, it is important to elicit information about the presence of previous end-organ dysfunction, particularly renal and cerebrovascular disease, and any other medical problems (eg, thyroid disease, Cushing disease, systemic lupus). In female patients, determine the date of their last menstrual period.
Patients may complain of specific symptoms that suggest end-organ dysfunction may be present. Chest pain may indicate myocardial ischemia or infarction, back pain may denote aortic dissection; and dyspnea may suggest pulmonary edema or congestive heart failure. The presence of neurologic symptoms may include seizures, visual disturbances, and altered level of consciousness and may be indicative of hypertensive encephalopathy.
The physical examination should assess whether end-organ dysfunction is present. BP should not only be measured in both the supine position and the standing position (assess volume depletion), but it should also be measured in both arms (a significant difference may suggest aortic dissection).
The presence of new retinal hemorrhages, exudates, or papilledema suggests a hypertensive emergency. Evaluate for the presence of heart failure, which may be indicated by jugular venous distention, crackles on auscultation, and peripheral edema. Central nervous system (CNS) findings may include changes in the patient's level of consciousness and visual fields, and/or the presence of focal neurologic signs. Abdominal masses or bruits may be noted.
Evaluation of uncontrolled hypertension
Obtain electrolyte levels, as well as measurements of blood urea nitrogen (BUN) and creatinine levels to evaluate for renal impairment. A dipstick urinalysis to detect hematuria or proteinuria and microscopic urinalysis to detect red blood cells (RBCs) or RBC casts should also be performed
A complete blood cell (CBC) count and peripheral blood smear should be obtained to exclude microangiopathic anemia, and a toxicology screen, pregnancy test, and endocrine testing may be obtained, as needed.
Imaging should be directed by the clinical presentation. If there is clinical evidence of pulmonary edema or the patient has chest pain, chest radiography and electrocardiography are indicated. Patients with neurologic signs should be evaluated with a head computed tomography scan initially, with more advanced imaging studies determined by the clinical presentation.
Malignant hypertension
Malignant hypertension and accelerated hypertension are both hypertensive emergencies (ie, systolic BP [SBP] >180 mm Hg or diastolic BP [DBP] >120 mm Hg, and acute target organ damage [10] ), with similar outcomes and therapies. Malignant hypertension may or may not be associated with clinical conditions present in hypertensive urgency (ie, SBP >180 mm Hg or DBP >120 mm Hg, but no evidence of acute target organ damage [10, 11] ; thus, hypertensive urgency occurs in the absence of acute end-organ damage, whereas hypertensive emergencies include the presence of acute end-organ damage [11, 12] ).
A patient with malignant hypertension always has retinal papilledema (as seen in the image below), [13] as well as flame-shaped hemorrhages and exudates. Other clinical features of malignant hypertension may include encephalopathy, confusion, left ventricular failure, intravascular coagulation, and impaired renal function, with hematuria and weight loss.
The pathologic hallmark of malignant hypertension is fibrinoid necrosis of the arterioles, which occurs systemically, but specifically in the kidneys. These patients develop fatal complications if untreated, and more than 90% will not survive beyond 1-2 years. See Malignant Hypertension.
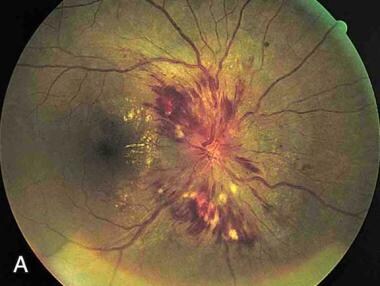 Papilledema. Note the swelling of the optic disc, with blurred margins
Papilledema. Note the swelling of the optic disc, with blurred margins
A study by Amraoui et al found a higher all-cause mortality rate in patients with malignant hypertension than in persons who were normotensive or hypertensive, even though the cardiovascular risk profile for the malignant hypertension patients was more favorable than that for the hypertensive controls. [14] The study, which compared 120 patients with a history of malignant hypertension with 120 normotensive and 120 hypertensive persons, found that the malignant hypertension patients had lower total cholesterol, low-density lipoprotein cholesterol, and body mass index values than did the hypertensive controls. However, the median estimated glomerular filtration rate was higher in the normotensive and hypertensive controls than in the malignant hypertension group. Annual all-cause mortality per 100 patient-years was 2.6 for the patients with malignant hypertension, compared to 0.2 and 0.5 for the normotensive and hypertensive controls, respectively. [14]
To see complete information on hypertension, please go to the main article by clicking here.
Management of Hypertensive Emergencies
Approximately 3%-45% of adult patients have at least one incident of increased blood pressure (BP) during their stay in the emergency department (ED). The fundamental principle in determining the necessary ED care of the hypertensive patient is the presence or absence of end-organ dysfunction. [12] Many patients present to the ED with elevated BPs; however, only a small proportion of patients will require emergency treatment. An important point to remember in the management of the patient with any degree of BP elevation is to "treat the patient and not the number."
The primary goal of the emergency physician is to determine which patients with acute hypertension are exhibiting symptoms of end-organ damage and require immediate intravenous (IV) parenteral therapy. [15] In contrast, patients presenting with acutely elevated BP (systolic BP [SBP] >200 mm Hg or diastolic BP [DBP] >120 mm Hg) without symptoms and whose BP stays significantly elevated to this level on discharge should have initiation of medical therapy and close follow-up in the outpatient setting, with BP reduction over hours or days. [12, 15, 16]
Thus, optimal control of hypertensive situations balances the benefits of immediate decreases in BP against the risk of a significant decrease in target organ perfusion. The emergency physician must be capable of appropriately evaluating patients with an elevated BP, correctly classifying the hypertension, determining the aggressiveness and timing of therapeutic interventions, and making disposition decisions.
Acutely lowering BP in the ED for clinical situations other than those listed below is controversial and generally should be avoided.
In pediatric hypertension, in the absence of hypertensive target organ damage, diet and exercise are used to treat stage I hypertension, followed by the addition of drug therapy if the initial strategy is unsuccessful. [17] In the presence of stage I hypertension with end-organ damage and stage II hypertension, management includes lifestyle changes and pharmacotherapy with angiotensin-converting enzyme inhibitors (ACEIs), calcium-channel blockers (CCBs), or thiazide diuretics. Hypertensive emergency with end-organ effects requires immediate, modest BP reduction with cardiac class IV medications. [17] Gradual lowering of the BP is crucial to preventing cerebral ischemia as a result of autoregulatory mechanisms. [18]
A retrospective study of 13 children aged 2 months to 16 years in a pediatric intensive care unit (PICU) found that an infusion of metoprolol is safe and effective for a hypertensive emergency in this population. [19] The symptomatic children all had an initial BP of 23-75 mm Hg above the 99th percentile for their age, height, and sex at presentation and received metoprolol infusion at a dose of 1-5 mcg/kg/min. At 1, 8, and 24 hours, mean BP fell by an average of 12.3%, 20.4%, and 27.1%, respectively; heart rate did not fall below the normal range for age, and no significant metoprolol infusion adverse effects were noted, including no neurologic sequelae as a consequence of their hypertension. [19]
Severe hypertension in pregnant women should be treated immediately to prevent maternal end-organ damage. [20] Hypertensive women who become pregnant or plan to become pregnant should be transitioned to methyldopa, nifedipine, and/or labetalol during pregnancy. [21] Hypertensive women who become pregnant should not be treated with ACEIs, angiotensin-receptor blockers (ARBs), or direct renin inhibitors. [21]
In a study that evaluated the efficacy of IV hydralazine (doses of 5, 10, 10, and 10 mg) and oral nifedipine (10 mg up to 4 doses) for acute hypertensive emergency in 60 pregnant patients, investigators noted both agents were equally effective in lowering BP in this setting. [22] Although no serious adverse maternal or perinatal side effects were noted in both groups, there was a significantly higher incidence of vomiting in the women receiving IV hydralazine.
The long-term prognosis for patients with hypertensive emergencies or urgencies is not good. In a retrospective study of 670 adults who presented with acute severe hypertension, short-term mortality was primarily due to neurovascular emergencies, but cardiovascular emergencies were severe and had high 12-month mortality. [23] Of the 670 patients, 57.5% had hypertensive emergencies; 98% of those with hypertensive emergencies and 23.2% of those with hypertensive urgencies were hospitalized. Median survival was 14 days for those with neurovascular emergencies and 50 days for those with cardiovascular emergencies. [23]
Pharmacotherapy
Optimal pharmacotherapy is dependent upon the specific organ at risk (see the individual sections below). In patients presenting with hypertensive emergencies, antihypertensive drug therapy has been shown to be effective in acutely decreasing BP. [24]
Sodium nitroprusside is a commonly used medication. It is a short-acting agent, and the BP response can be titrated from minute to minute. However, patients must have constant monitoring in an ICU. The potential exists for thiocyanate and cyanide toxicity with prolonged use or if the patient has renal or hepatic failure.
Labetalol, an alpha- and beta-blocking agent, has proven to be quite beneficial in the treatment of patients with hypertensive emergencies. Labetalol is particularly preferred in patients with acute dissection and those with end-stage renal disease. Boluses of 10-20 mg may be administered, or the drug may be infused at 1 mg/min until the desired BP is obtained. Once an adequate BP level is obtained, oral hypertensive therapy should be initiated, and patients are gradually weaned from parenteral agents.
Fenoldopam, a peripheral dopamine-1-receptor agonist is given as initial IV dose of 0.1 µg/kg/min titrated every 15 minutes.
Clevidipine, a dihydropyridine CCB, is administered IV for rapid and precise BP reduction. [25] It is rapidly metabolized in the blood and tissues and does not accumulate in the body. Initiate IV infusion of clevidipine at 1-2 mg/hour; titrate the dose at short intervals (ie, 90 seconds) initially by doubling the dose.
As the BP approaches its goal, increase the clevidipine dose by less than double, and lengthen the time between dose adjustments to every 5-10 minutes. An approximately 1-2 mg/hour increase produces an additional 2-4 mm Hg decrease in SBP. Typically, the therapeutic response is achieved with 4-6 mg/hour, although severe hypertension may require higher doses. Most patients have received maximum doses of 16 mg/hour or less; experience is limited with short-term dosing as high as 32 mg/hour. Because of lipid load restrictions, do not exceed 1000 mL or an average of 21 mg/hour within a 24-hour period; experience is limited with use beyond 72 hours.
Guidelines recommendations
The 2017 American College of Cardiology/American Heart Association (ACC/AHA) guidelines recommendations for hypertensive crises and emergencies include the following [21] :
-
Admit adults with a hypertensive emergency to an ICU for continuous monitoring of BP and target organ damage, as well as for parenteral administration of an appropriate medication.
-
For adults with a compelling condition (ie, aortic dissection, severe preeclampsia or eclampsia, or pheochromocytoma crisis), lower SBP to below 140 mm Hg during the first hour and to below 120 mm Hg in aortic dissection.
-
For adults without a compelling condition, reduce the SBP to a maximum of 25% within the first hour; then, if the patient is clinically stable, lower the BP to 160/100 -110 mm Hg over the next 2-6 hours, and then cautiously to normal over the following 24-48 hours.
Neurologic emergencies
BP reduction is indicated in neurologic emergencies, such as hypertensive encephalopathy, acute ischemic stroke, acute intracerebral hemorrhage, and subarachnoid hemorrhage.
Hypertensive encephalopathy
In hypertensive encephalopathy, the treatment guidelines are to reduce the MAP 25% over 8 hours. [26] Labetalol, nicardipine, esmolol are the preferred medications; nitroprusside and hydralazine should be avoided.
Acute ischemic stroke
For acute ischemic stroke, the preferred medications are labetalol and nicardipine. Withhold antihypertensive medications unless the SBP is above 220 mm Hg or the DBP is over 120 mm Hg, UNLESS the patient is eligible for IV tissue plasminogen activator (tPA); then, the goal is a gradual reduction of BP with a goal SBP of less than 185 mm Hg and a DBP below 110 mm Hg before initiating thrombolitic therapy. [21] After initiating drug therapy but before administering tPA, the SBP should be maintained at less than 180 mm Hg and the DBP below 105 mm Hg for 24 hours. [21, 26]
Acute intracerebral hemorrhage
For acute intracerebral hemorrhage, the preferred medications are labetalol, nicardipine, and esmolol; avoid nitroprusside and hydralazine. The treatment is based on clinical/radiographic evidence of increased intracranial pressure (ICP). If there are signs of increased ICP, maintain the MAP just below 130 mm Hg (or SBP < 180 mm Hg) for the first 24 hours after onset. In patients without increased ICP, maintain the MAP below 110 mm Hg (or SBP < 160 mm Hg) for the first 24 hours after symptom onset. [26]
In adults with acute intracerebral hemorrhage who present with an SBP above 220 mm Hg, continuous IV drug and close BP monitoring is reasonable to lower SBP. [21] Note that it may be harmful to immediately lower SBP to below 140 mm Hg in adults with spontaneous intracerebral hemorrhage who present within 6 hours of the acute event and have an SBP between 150 and 220 mm Hg. [21]
Subarachnoid hemorrhage
In subarachnoid hemorrhage, nicardipine, labetalol, and esmolol are also the preferred agents; again, nitroprusside and hydralazine should be avoided. Maintain the SBP below 160 mm Hg until the aneurysm is treated or cerebral vasospasm occurs. Although oral nimodipine is used to prevent delayed ischemic neurologic deficits, it is NOT indicated for treating acute hypertension. [26]
Cardiovascular emergencies
Rapid BP reduction is also indicated in cardiovascular emergencies, such as aortic dissection, acute coronary syndrome, and acute heart failure.
Aortic dissection
Beta blockers are the recommended antihypertensive agents in patients with hypertension and thoracic aortic disease. [21] In aortic dissection, the preferred medications are labetalol, nicardipine, nitroprusside (with beta-blocker), esmolol, and morphine sulfate. However, avoid beta-blockers if there is aortic valvular regurgitation or suspected cardiac tamponade.
For adults with aortic dissection, rapidly lower the SBP to below 120 mm Hg; the preferred agents are esmolol and labetalol. [21] Beta blockade should precede vasodilator administration, if needed for BP control or to prevent reflex tachycardia or inotropic effect; achieve SBP up to 120 mm Hg within 20 minutes. [21]
Maintain the SBP below 110 mm Hg, unless signs of end-organ hypoperfusion are present. The preferred treatment includes a combination of narcotic analgesics (morphine sulfate), beta blockers (labetalol, esmolol), and vasodilators (nicardipine, nitroprusside). CCBs (verapamil, diltiazem) are an alternative to beta blockers. [27]
Acute coronary syndrome
For acute coronary syndrome, beta blockers and nitroglycerin are the preferred drugs. Treatment is indicated if the SBP is above 160 mm Hg and/or the DBP is over 100 mm Hg. Reduce the BP by 20%-30% of baseline. Note that thrombolytics are contraindicated if the BP is above 185/100 mm Hg. [28] In addition, note that nitrates administered in the presence of phosphodiesterase type 5 (PDE-5) inhibitors may induce profound hypotension. [21]
Acute heart failure
In acute heart failure, the preferred medications are IV nitroglycerin or sublingual nitroglycerin and IV enalaprilat. Treat with vasodilators (in addition to diuretics) for a SBP of 140 mm Hg. [28]
In adults with hypertension at an increased risk of heart failure, the optimal BP should be below 130/80 mm Hg. [21]
In hypertensive adults with reduced ejection fraction (HFrEF), prescribe guideline-directed medical therapy (GDMT) to achieve a BP below 130/80 mm Hg. [21] Note that nondihydropyridine CCBs are not recommended for treatment in this patient population.
In hypertensive adults with preserved ejection fraction (HFpEF) and symptoms of volume overload, prescribe diuretics to control BP. [21] For those with persistent hypertension after management of volume overload, prescribe ACEIs or ARBs and beta blockers titrated to achieve an SBP below 130 mm Hg.
Cocaine toxicity/pheochromocytoma
Diazepam, phentolamine, and nitroglycerin/nitroprusside are the preferred drugs. However, avoid beta-adrenergic antagonists before administering phentolamine.
Hypertension and tachycardia from cocaine toxicity rarely require specific treatment. Alpha-adrenergic antagonists (phentolamine) are the preferred agents for cocaine-associated acute coronary syndromes. [29]
Pheochromocytoma treatment guidelines are similar to that of cocaine toxicity. The ACC/AHA recommends lowering the SBP to below 140 mm Hg during the first hour, with phentolamine IV bolus dose of 5 mg. Additional bolus doses may be given every 10 minutes as needed to achieve target BP. [21] Only after alpha blockade can beta blockers be added for BP control.
Preeclampsia/eclampsia
The preferred medications are hydralazine, labetalol, and nicardipine. Avoid nitroprusside, ACEIs, ARBs, and renin inhibitors. [21] In women with eclampsia or preeclampsia, the SBP should lowered to below 140 mm Hg during the first hour. [21]
If the platelet count is less than 100,000 cells mm3, the BP should be maintained below 150/100 mm Hg. Patients with eclampsia or preeclampsia should also be treated with IV magnesium sulfate to avoid seizures. [30]
Perioperative hypertension
The ACC/AHA defines perioperative hypertension as a BP of 160/90 mm Hg or higher or an SBP elevation of at least 20% of the preoperative value that persists for longer than 15 minutes. [21]
Nitroprusside, nitroglycerin, clevidipine, nicardipine, and esmolol are preferred. Target the perioperative BP to within 20% of the patient's baseline pressure, except if there is the potential for life-threatening arterial bleeding. Perioperative beta blockers are the first choice in patients undergoing vascular procedures or in patients with an intermediate or high risk of cardiac complications. [27]
Preoperative
In patients with preoperative hypertension undergoing major surgery who have been taking chronic beta blockers, continue the beta blockers. [21] In those with preoperative hypertension undergoing major surgery, consider perioperative discontinuation of ACEIs or ARBs.
In patients with preoperative hypertension undergoing planned elective major surgery, continuing medical therapy for hypertension until surgery is reasonable. [21] In patients with planned elective major surgery and an SBP of 180 mm Hg or higher or a DBP of 110 mm Hg or higher, consider deferring surgery.
Note that abrupt preoperative discontinuation of beta blockers or clonidine in patients undergoing surgery may be harmful. [21] In addition, avoid the initiation of beta blockers on the day of surgery in beta blocker-naïve patients.
Intraoperative
Manage patients with intraoperative hypertension with IV agents until oral medications can be resumed. [21]
Questions & Answers
Overview
What is a hypertensive emergency?
What neurologic end-organ damage can occur in a hypertensive emergency?
How common are hypertensive emergencies in the US?
What is the role of the history and the physical exam in hypertensive emergencies?
What are the most common clinical presentations of hypertensive emergencies?
What causes hypertensive emergencies in pregnancy?
Which symptoms of hypertensive emergencies may indicate end-organ damage?
What should be evaluated in the physical exam of hypertensive emergency?
Which symptoms are associated with a hypertensive emergency?
Which lab testing is indicated in the evaluation of a hypertensive emergency?
Which imaging studies are indicated in the workup of a hypertensive emergency?
What is the pathologic hallmark of a malignant hypertensive emergency?
Which features of malignant hypertensive emergencies contribute to increased mortality?
What is the ED physician’s primary goal in treating hypertensive emergencies?
What are the treatment approaches to pediatric hypertension?
What are the treatment approaches to severe hypertension in pregnancy?
What is the long-term prognosis of patients with hypertensive emergency or urgency?
What drug treatment is indicated for hypertensive emergencies?
How is sodium nitroprusside used to treat hypertensive emergencies?
How is labetalol used to treat hypertensive emergencies?
How is fenoldopam used to treat hypertensive emergencies?
How is clevidipine used to treat hypertensive emergencies?
What are the 2017 ACC/AHA guidelines for hypertensive crises and emergencies?
What is the role of BP reduction in neurologic hypertensive emergencies?
What are the treatment guidelines for hypertensive encephalopathy emergency?
Which medications are used to treat acute ischemic stroke associated with a hypertensive emergency?
When is rapid BP reduction indicated in hypertensive emergencies?
What is the recommended treatment for hypertension with thoracic aortic disease?
How are hypertensive emergencies managed in adults with aortic dissection?
What is the target BP in adults with hypertension and an increased risk of heart failure?
How is medication used to treat hypertensive adults with reduced ejection fraction (HFrEF)?
How is medication used to treat hypertensive adults with preserved ejection fraction (HFrEF)?
What are the treatment guidelines for hypertensive emergencies associated with pheochromocytoma?
Which medications are used in the treatment of hypertensive emergencies in pregnancy?
Which medications are used in the treatment of perioperative hypertension?
-
Papilledema. Note the swelling of the optic disc, with blurred margins








