Practice Essentials
Migraine is a complex disorder characterized by recurrent episodes of headache, most often unilateral and in some cases associated with visual or sensory symptoms—collectively known as an aura—that arise most often before the head pain but that may occur during or afterward (see the image below). Migraine is most common in women and has a strong genetic component.
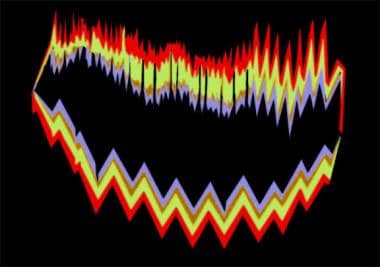 Migraine headache. Example of a visual migraine aura as described by a person who experiences migraines. This patient reported that these visual auras preceded her headache by 20-30 minutes.
Migraine headache. Example of a visual migraine aura as described by a person who experiences migraines. This patient reported that these visual auras preceded her headache by 20-30 minutes.
Signs and symptoms
Typical symptoms of migraine include the following:
-
Throbbing or pulsatile headache, with moderate to severe pain that intensifies with movement or physical activity
-
Unilateral and localized pain in the frontotemporal and ocular area, but the pain may be felt anywhere around the head or neck
-
Pain builds up over a period of 1–2 hours, progressing posteriorly and becoming diffuse
-
Headache lasts 4–72 hours
-
Nausea (80%) and vomiting (50%), including anorexia and food intolerance, and light-headedness
-
Sensitivity to light and sound
Features of migraine aura are as follows:
-
May precede or accompany the headache phase or may occur in isolation
-
Usually develops over 5–20 minutes and lasts less than 60 minutes
-
Most commonly visual but can be sensory, motor, or any combination of these
-
Visual symptoms may be positive or negative
-
The most common positive visual phenomenon is the scintillating scotoma, an arc or band of absent vision with a shimmering or glittering zigzag border
Physical findings during a migraine headache may include the following:
-
Cranial/cervical muscle tenderness
-
Horner syndrome (ie, relative miosis with 1–2 mm of ptosis on the same side as the headache)
-
Conjunctival injection
-
Tachycardia or bradycardia
-
Hypertension or hypotension
-
Hemisensory or hemiparetic neurologic deficits (ie, complicated migraine)
-
Adie-type pupil (ie, poor light reactivity, with near dissociation from light)
See Clinical Presentation for more detail.
Diagnosis
The diagnosis of migraine is based on patient history. International Headache Society diagnostic criteria are that patients must have had at least 5 headache attacks that lasted 4–72 hours (untreated or unsuccessfully treated) and that the headache must have had at least 2 of the following characteristics: [1]
-
Unilateral location
-
Pulsating quality
-
Moderate or severe pain intensity
-
Aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs)
In addition, during the headache the patient must have had at least 1 of the following:
-
Nausea and/or vomiting
-
Photophobia and phonophobia
Finally, these features must not have been attributable to another disorder. Classification of migraine is as follows:
-
Migraine without aura (formerly, common migraine)
-
Probable migraine without aura
-
Migraine with aura (formerly, classic migraine)
-
Probable migraine with aura
-
Chronic migraine
-
Chronic migraine associated with analgesic overuse
-
Childhood periodic syndromes that may not be precursors to or associated with migraine
-
Complications of migraine
-
Migrainous disorder not fulfilling above criteria
Migraine variants include the following:
-
Childhood periodic syndromes
-
Late-life migrainous accompaniments
-
Migraine with brainstem aura
-
Hemiplegic migraine
-
Status migrainosus
-
Retinal migraine
A migraine variant may be suggested by focal neurologic findings, such as the following, that occur with the headache and persist temporarily after the pain resolves:
-
Unilateral paralysis or weakness - Hemiplegic migraine
-
Dysarthria, vertigo, ataxia - Migraine with brainstem aura
Testing and imaging studies
Selection of laboratory and/or imaging studies to rule out conditions other than migraine headache is determined by the individual presentation (eg, erythrocyte sedimentation rate and C-reactive protein levels may be appropriate to exclude temporal/giant cell arteritis). Neuroimaging is not necessary in patients with a history of recurrent migraine headaches and a normal neurologic examination.
The American Headache Society released a list of 5 commonly performed tests or procedures that are not always necessary in the treatment of migraine and headache, as part of the American Board of Internal Medicine (ABIM) Foundation's Choosing Wisely campaign. The recommendations include: [2, 3]
-
Don't perform neuroimaging studies in patients with stable headaches that meet criteria for migraine.
-
Don't perform computed tomography imaging for headache when magnetic resonance imaging is available, except in emergency settings.
-
Don't recommend surgical deactivation of migraine trigger points outside of a clinical trial.
-
Don't prescribe opioid or butalbital-containing medications as first-line treatment for recurrent headache disorders.
-
Don't recommend prolonged or frequent use of over-the-counter pain medications for headache.
See Workup for more detail.
Management
Pharmacologic agents used for the treatment of migraine can be classified as abortive (ie, for alleviating the acute phase) or prophylactic (ie, preventive).
Acute/abortive medications
Acute treatment aims to reverse, or at least stop the progression of, a headache. It is most effective when given within 15 minutes of pain onset and when pain is mild. [4]
Abortive medications include the following:
-
Selective serotonin receptor (5-hydroxytryptamine–1, or 5-HT1) agonists (triptans)
-
Serotonin 5-HT1F agonists (ditans) (eg, lasmiditan)
-
Calcitonin gene-related peptide (CGRP) receptor antagonists (ie, rimegepant, ubrogepant)
-
Ergot alkaloids (eg, ergotamine, dihydroergotamine [DHE])
-
Analgesics
-
Nonsteroidal anti-inflammatory drugs (NSAIDs)
-
Combination products
-
Antiemetics
Preventive/prophylactic medications
The following may be considered indications for prophylactic migraine therapy:
-
Frequency of migraine attacks is greater than 2 per month
-
Duration of individual attacks is longer than 24 hours
-
The headaches cause major disruptions in the patient's lifestyle, with significant disability that lasts 3 or more days
-
Abortive therapy fails or is overused
-
Symptomatic medications are contraindicated or ineffective
-
Use of abortive medications more than twice a week
-
Migraine variants such as hemiplegic migraine or rare headache attacks producing profound disruption or risk of permanent neurologic injury [5]
Prophylactic medications include the following:
-
Antiepileptic drugs
-
Beta blockers
-
Tricyclic antidepressants
-
Calcium channel blockers
-
Selective serotonin reuptake inhibitors (SSRIs)
-
NSAIDs
-
Serotonin antagonists
-
Botulinum toxin
-
CGRP inhibitors
Other measures
Treatment of migraine may also include the following:
-
Reduction of migraine triggers (eg, lack of sleep, fatigue, stress, certain foods)
-
Nonpharmacologic therapy (eg, biofeedback, cognitive-behavioral therapy)
-
Integrative medicine (eg, butterbur, riboflavin, magnesium, feverfew, coenzyme Q10)
See Treatment and Medication for more detail.
Background
Migraine headache is a complex, recurrent headache disorder that is one of the most common complaints in medicine. In the United States, more than 30 million people have 1 or more migraine headaches per year. Approximately 75% of all persons who experience migraines are women (see Epidemiology).
The term migraine is derived from the Greek word hemikrania. This term was corrupted into low Latin as hemigranea, the French translation of which was migraine.
Causes of migraine
Migraine was previously considered to be a vascular phenomenon that resulted from intracranial vasoconstriction followed by rebound vasodilation. Currently, however, the neurovascular theory describes migraine as primarily a neurogenic process with secondary changes in cerebral perfusion associated with a sterile neurogenic inflammation (see Pathophysiology).
A genetic component to migraine is indicated by the fact that approximately 70% of patients have a first-degree relative with a history of migraine. In addition, a variety of environmental and behavioral factors may precipitate migraine attacks in persons with a predisposition to migraine (see Etiology).
Migraine characteristics and treatment
Migraine is characterized most often by unilateral head pain that is moderate to severe, throbbing, and aggravated by activity. It may also be associated with various visual or sensory symptoms, which occur most often before the headache component but which may occur during or after the headache; these are collectively known as an aura. Most commonly, the aura consists of visual manifestations, such as scotomas, photophobia, or visual scintillations (eg, bright zigzag lines) (see Presentation).
The head pain may also be associated with weakness. This form of migraine is termed hemiplegic migraine.
In practice, however, migraine headaches may be unilateral or bilateral and may occur with or without an aura. In the current International Headache Society categorization, the headache previously described as classic migraine is now known as migraine with aura, and the headache that was described as common migraine is now termed migraine without aura. Migraines without aura are the most common, accounting for more than 80% of all migraines.
The diagnosis of migraine is clinical in nature, based on criteria established by the International Headache Society. A full neurologic examination should be performed during the first visit, to exclude other disorders; the findings are usually normal in patients with migraine. Neuroimaging is not necessary in a typical case, but other diagnostic investigations may be indicated to guide management.
A screening tool called the ID-CM may be useful in diagnosis. The ID-CM is a 12-item screening tool for chronic migraine that has a sensitivity of 82% and a specificity of 87% compared with semi-structured clinical interviews. [6]
Migraine treatment involves acute (abortive) and preventive (prophylactic) therapy. Patients with frequent attacks usually require both. Measures directed toward reducing migraine triggers are also generally advisable.
Acute treatment aims to eliminate, or at least prevent the progression of, a headache. Preventive treatment, which is given even in the absence of a headache, aims to reduce the frequency and severity of migraine attacks, to make acute attacks more responsive to abortive therapy, and perhaps also to improve the patient's quality of life (see Treatment).
See Migraine in Children for a pediatric perspective on migraine. Also see Migraine Variants and Childhood Migraine Variants.
Migraine classification
The third edition of the International Classification of Headache Disorders (ICHD) [1] lists the following types of migraine:
-
Migraine without aura (formerly, common migraine)
-
Probable migraine without aura
-
Migraine with aura (formerly, classic migraine)
-
Probable migraine with aura
-
Chronic migraine
-
Chronic migraine associated with analgesic overuse
-
Childhood periodic syndromes that may not be precursors to or associated with migraine
-
Complications of migraine
-
Migrainous disorder not fulfilling above criteria
Diagnostic criteria
According to the International Headache Society, the diagnosis of migraine requires that the patient has experienced at least 5 attacks that fulfill the following 3 criteria and that are not attributable to another disorder. [1] First, the headache attacks must have lasted 4–72 hours (untreated or unsuccessfully treated). Second, the headache must have had at least 2 of the following characteristics:
-
Unilateral location
-
Pulsating quality
-
Moderate or severe pain intensity
-
Aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs)
Third, during the headache the patient experiences at least 1 of the following:
-
Nausea and/or vomiting
-
Photophobia and phonophobia
In January 2018, the International Classification of Headache Disorders, Third Edition was published.
Changes from the previous edition include the following: [7]
-
The addition of chronic migraines: Those that occur on at least 15 days of the month for more than 3 months
-
For a diagnosis of migraine with aura, the following criteria must be met: One or more visual, sensory, speech, motor, brainstem, or retinal symptoms, as well as at least 2 of the following 4 criteria: (1) at least 1 aura symptom spreading gradually over 5 or more minutes and/or 2 or more symptoms occurring in succession; (2) each aura symptom lasting 5–60 minutes; (3) at least 1 aura symptom being unilateral; and (4) the aura being accompanied by or followed shortly by headache
-
Under headaches associated with sexual activity, the subtypes of preorgasmic and orgasmic headache have been eliminated
-
For thunderclap headaches, the headache must last at least 5 minutes, but the criterion of not recurring regularly during subsequent weeks or months has been discarded
-
Hypnic headaches no longer have to first occur after age 50 years
-
A number of pain characteristics under the new daily persistent headaches section have been eliminated
-
For secondary headaches, it is not required that the causative agent be removed before a diagnosis
Migraine guidelines
In April 2000, the US Headache Consortium, a multispecialty group that includes the American College of Emergency Physicians, released evidence-based guidelines for the diagnosis, treatment, and prevention of migraine headaches. Guidelines are also available from the American Academy of Neurology, the National Headache Foundation, and the Canadian Association of Emergency Physicians. [4, 8, 9]
Pathophysiology
The mechanisms of migraine remain incompletely understood. However, new technologies have allowed formulation of current concepts that may explain parts of the migraine syndrome.
Vascular theory
In the 1940s and 1950s, the vascular theory was proposed to explain the pathophysiology of migraine headache. Wolff et al believed that ischemia induced by intracranial vasoconstriction is responsible for the aura of migraine and that the subsequent rebound vasodilation and activation of perivascular nociceptive nerves resulted in headache.
This theory was based on the following 3 observations:
-
Extracranial vessels become distended and pulsatile during a migraine attack
-
Stimulation of intracranial vessels in an awake person induces headache
-
Vasoconstrictors (eg, ergots) improve the headache, whereas vasodilators (eg, nitroglycerin) provoke an attack
However, this theory did not explain the prodrome and associated features. Nor did it explain the efficacy of some drugs used to treat migraines that have no effect on blood vessels and the fact that most patients do not have an aura. Moreover, with the advent of newer imaging technologies, researchers found that intracranial blood flow patterns were inconsistent with the vascular theory.
No consistent flow changes have been identified in patients suffering from migraine headache without aura. Regional cerebral blood flow (rCBF) remains normal in the majority of patients. However, bilateral decrease in rCBF, beginning at the occipital cortex and spreading anteriorly, has been reported. More recently, Perciaccante has shown that migraine is characterized by a cardiac autonomic dysfunction. [10]
As a result of these anomalous findings, the vascular theory was supplanted by the neurovascular theory.
Neurovascular theory
The neurovascular theory holds that a complex series of neural and vascular events initiates migraine. [11] According to this theory, migraine is primarily a neurogenic process with secondary changes in cerebral perfusion. [12]
At baseline, a migraineur who is not having any headache has a state of neuronal hyperexcitability in the cerebral cortex, especially in the occipital cortex. [13] This finding has been demonstrated in studies of transcranial magnetic stimulation and with functional magnetic resonance imaging (MRI).
This observation explains the special susceptibility of the migrainous brain to headaches. [14] One can draw a parallel with the patient with epilepsy who similarly has interictal neuronal irritability.
Cortical spreading depression
In 1944, Leao proposed the theory of cortical spreading depression (CSD) to explain the mechanism of migraine with aura. CSD is a well-defined wave of neuronal excitation in the cortical gray matter that spreads from its site of origin at the rate of 2-6 mm/min.
This cellular depolarization causes the primary cortical phenomenon or aura phase; in turn, it activates trigeminal fibers, causing the headache phase. The neurochemical basis of the CSD is the release of potassium or the excitatory amino acid glutamate from neural tissue. This release depolarizes the adjacent tissue, which, in turn, releases more neurotransmitters, propagating the spreading depression.
Oligemia
Positron emission tomography (PET) scanning demonstrates that blood flow is moderately reduced during a migrainous aura, but the spreading oligemia does not correspond to vascular territories. The oligemia itself is insufficient to impair function. Instead, the flow is reduced because the spreading depression reduces metabolism.
Although CSD is the disturbance that presumably results in the clinical manifestation of migraine aura, this spreading oligemia can be clinically silent (ie, migraine without aura). Perhaps a certain threshold is required to produce symptoms in patients having aura but not in those without aura. A study of the novel agent tonabersat, which inhibits CSD, found that the agent helped to prevent migraine attacks with aura only, suggesting that CSD may but not be involved in attacks without aura. [15]
Trigeminovascular system
Activation of the trigeminovascular system by CSD stimulates nociceptive neurons on dural blood vessels to release plasma proteins and pain-generating substances such as calcitonin gene-related peptide, substance P, vasoactive intestinal peptide, and neurokinin A. The resultant state of sterile inflammation is accompanied by further vasodilation, producing pain.
The initial cortical hyperperfusion in CSD is partly mediated by the release of trigeminal and parasympathetic neurotransmitters from perivascular nerve fibers, whereas delayed meningeal blood flow increase is mediated by a trigeminal-parasympathetic brainstem connection. According to Moulton et al, altered descending modulation in the brainstem has been postulated to contribute to the headache phase of migraine; this leads to loss of inhibition or enhanced facilitation, resulting in trigeminovascular neuron hyperexcitability. [16]
Metalloproteinases
In addition, through a variety of molecular mechanisms, CSD upregulates genes, such as those encoding for cyclo-oxygenase 2 (COX-2), tumor necrosis factor alpha (TNF-alpha), interleukin-1beta, galanin, and metalloproteinases. The activation of metalloproteinases leads to leakage of the blood-brain barrier, allowing potassium, nitric oxide, adenosine, and other products released by CSD to reach and sensitize the dural perivascular trigeminal afferent endings. [17]
Increased net activity of matrix metalloproteinase–2 (MMP-2) has been demonstrated in migraineurs. Patients who have migraine without aura seem to have an increased ratio of matrix metalloproteinase–9 (MMP-9) to tissue inhibitors of metalloproteinase–1 (TIMP-1), in contrast to a lower MMP-9/TIMP-1 ratio in patients who have migraine with aura. [18] Measured levels of MMP-9 alone are the same for migraine patients with or without aura. [19]
Hypoxia
In an experimental study, acute hypoxia was induced by a single episode of CSD. This was accompanied by dramatic failure of brain ion homeostasis and prolonged impairment of neurovascular and neurometabolic coupling. [20]
Vasoactive substances and neurotransmitters
Perivascular nerve activity also results in release of substances such as substance P, neurokinin A, calcitonin gene-related peptide, and nitric oxide, which interact with the blood vessel wall to produce dilation, protein extravasation, and sterile inflammation. This stimulates the trigeminocervical complex, as shown by induction of c-fos antigen by PET scan. Information then is relayed to the thalamus and cortex for registering of pain. Involvement of other centers may explain the associated autonomic symptoms and affective aspects of this pain.
Neurogenically induced plasma extravasation may play a role in the expression of pain in migraine, but it may not be sufficient by itself to cause pain. The presence of other stimulators may be required.
Although some drugs that are effective for migraine inhibit neurogenic plasma extravasation, substance P antagonists and the endothelin antagonist bosentan inhibit neurogenic plasma extravasation but are ineffective as antimigraine drugs. Also, the pain process requires not only the activation of nociceptors of pain-producing intracranial structures but also reduction in the normal functioning of endogenous pain-control pathways that gate the pain.
Migraine center
A potential "migraine center" in the brainstem has been proposed, based on PET-scan results showing persistently elevated rCBF in the brainstem (ie, periaqueductal gray, midbrain reticular formation, locus ceruleus) even after sumatriptan-produced resolution of headache and related symptoms. These were the findings in 9 patients who had experienced spontaneous attack of migraine without aura. The increased rCBF was not observed outside of the attack, suggesting that this activation was not due to pain perception or increased activity of the endogenous antinociceptive system.
The fact that sumatriptan reversed the concomitant increased rCBF in the cerebral cortex but not the brainstem centers suggests dysfunction in the regulation involved in antinociception and vascular control of these centers. Thalamic processing of pain is known to be gated by ascending serotonergic fibers from the dorsal raphe nucleus and from aminergic nuclei in the pontine tegmentum and locus ceruleus; the latter can alter brain flow and blood-brain barrier permeability.
Because of the set periodicity of migraine, linkage to the suprachiasmatic nucleus of the hypothalamus that governs circadian rhythm has been proposed. Discovering the central trigger for migraine would help to identify better prophylactic agents.
Brainstem activation
PET scanning in patients having an acute migraine headache demonstrates activation of the contralateral pons, even after medications abort the pain. Weiler et al proposed that brainstem activation may be the initiating factor of migraine.
Once the CSD occurs on the surface of the brain, H+ and K+ ions diffuse to the pia mater and activate C-fiber meningeal nociceptors, releasing a proinflammatory soup of neurochemicals (eg, calcitonin gene–related peptide) and causing plasma extravasation to occur. Therefore, a sterile, neurogenic inflammation of the trigeminovascular complex is present.
Once the trigeminal system is activated, it stimulates the cranial vessels to dilate. The final common pathway to the throbbing headache is the dilatation of blood vessels.
Cutaneous allodynia
Burstein et al described the phenomenon of cutaneous allodynia, in which secondary pain pathways of the trigeminothalamic system become sensitized during a migrainous episode. [21] This observation demonstrates that, along with the previously described neurovascular events, sensitization of central pathways in the brain mediates the pain of migraine.
Dopamine pathway
Some authors have proposed a dopaminergic basis for migraine. [22] In 1977, Sicuteri postulated that a state of dopaminergic hypersensitivity is present in patients with migraine. Interest in this theory has recently been renewed.
Some of the symptoms associated with migraine headaches, such as nausea, vomiting, yawning, irritability, hypotension, and hyperactivity, can be attributed to relative dopaminergic stimulation. Dopamine receptor hypersensitivity has been shown experimentally with dopamine agonists (eg, apomorphine). Dopamine antagonists (eg, prochlorperazine) completely relieve almost 75% of acute migraine attacks.
Magnesium deficiency
Another theory proposes that deficiency of magnesium in the brain triggers a chain of events, starting with platelet aggregation and glutamate release and finally resulting in the release of 5-hydroxytryptamine, which is a vasoconstrictor. In clinical studies, oral magnesium has shown benefit for preventive treatment and intravenous magnesium may be effective for acute treatment, particularly in certain subsets of migraine patients. [23]
Endothelial dysfunction
Vascular smooth muscle cell dysfunction may involve impaired cyclic guanosine monophosphate and hemodynamic response to nitric oxide. [24] Nitric oxide released by microglia is a potentially cytotoxic proinflammatory mediator, initiating and maintaining brain inflammation through activation of the trigeminal neuron system.
Nitric oxide levels continue to be increased even in the headache-free period in migraineurs. [25] In premenopausal women with migraine, particularly in those with migraine aura, increased endothelial activation, which is a component of endothelial dysfunction, is evident. [26]
Serotonin and migraine
The serotonin receptor (5-hydroxytryptamine [5-HT]) is believed to be the most important receptor in the headache pathway. Immunohistochemical studies have detected 5-hydroxytryptamine–1D (5-HT1D) receptors in trigeminal sensory neurons, including peripheral projections to the dura and within the trigeminal nucleus caudalis (TNC) and solitary tract, while 5-HT1B receptors are present on smooth muscle cells in meningeal vessels; however, both can be found in both tissues to some extent and even in coronary vessels.
All the currently available triptans (see Medication) are selective 5-HT1B/D full agonists. These agents may decrease headache by abolishing neuropeptide release in the periphery and blocking neurotransmission by acting on second-order neurons in the trigeminocervical complex.
Migraine risk factors
Predisposing vascular risk factors for migraine include the following [27] :
-
Increased levels of C-reactive protein
-
Increased levels of interleukins
-
Increased levels of TNF-alpha and adhesion molecules (systemic inflammation markers)
-
Oxidative stress and thrombosis
-
Increased body weight
-
High blood pressure
-
Hypercholesterolemia
-
Impaired insulin sensitivity
-
High homocysteine levels
-
Stroke
-
Coronary heart disease
Transformed migraine/medication overuse headache
In some patients, migraine progresses to chronic migraine. Acute overuse of symptomatic medication is considered one of the most important risk factors for migraine progression. Medication overuse headache can occur with any analgesic, including acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, naproxen, and aspirin. In addition, Bigal and Lipton identified the following associations of medication with progression to chronic migraine [28] :
-
Opiates - Critical dose of exposure is around 8 days per month; the effect is more pronounced in men
-
Barbiturates - Critical dose of exposure is around 5 days per month; the effect is more pronounced in women
-
Triptans - Migraine progression is seen only in patients with high frequency of migraine at baseline (10-14 days/mo)
In the study, the effect of anti-inflammatory medications varied with headache frequency. These agents were protective in patients with fewer than 10 days of headache at baseline but induced migraine progression in patients with a high frequency of headaches at baseline. [28]
Etiology
Migraine has a strong genetic component. Approximately 70% of migraine patients have a first-degree relative with a history of migraine. The risk of migraine is increased 4-fold in relatives of people who have migraine with aura. [29]
Nonsyndromic migraine headache with or without aura generally shows a multifactorial inheritance pattern, but the specific nature of the genetic influence is not yet completely understood. Certain rarer syndromes with migraine as a clinical feature generally show an autosomal dominant inheritance pattern. [30]
However, recent genome-wide association studies have suggested 4 regions in which single-nucleotide polymorphisms influence the risk of developing migraine headache. [31, 32, 33] Other associations have been found in individual studies but could not be replicated in other populations.
Familial hemiplegic migraine
Familial hemiplegic migraine (FHM) is a rare type of migraine with aura that is preceded or followed by hemiplegia, which typically resolves. FHM may be associated with cerebellar ataxia, which is also linked to the 19p locus. Evidence suggests that the 19p locus for FHM may also be involved in patients with other forms of migraine. Three genes have thus far been identified as being causative for FHM.
FHM type 1 is characterized clinically by episodes that commonly include nystagmus and cerebellar signs. This disorder is caused by mutations in the CACNA1A gene located on 19p13, which codes for a brain-specific calcium channel. Mutations in CACNA1A were previously thought to account for 50% of cases of FHM, [34] but a Danish study showed that only 7% of patients with a clinical diagnosis of FHM had a mutation in that gene. [35]
FHM type 2 occurs in patients who also have a seizure disorder. This condition has been attributed to mutations in the ATP1A2 gene, located on 1q21q23, which encodes a sodium/potassium pump. [36, 37] However, the Danish study found mutations in ATP1A2 in only 7% of patients with a clinical diagnosis of FHM. [35]
FHM type 3 is caused by mutations in the SCN1A gene, located on 2q24. Mutations in SCN1A are also known to cause familial febrile seizure disorders and infantile epileptic encephalopathy. [38] Although SCN1A mutation has been reported in several unrelated families, it is felt to be a rare cause of FHM. [39]
Migraine in other inherited disorders
Migraine occurs with increased frequency in patients with mitochondrial disorders, such as MELAS (mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes). CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy) is a genetic disorder that causes migraine with aura, strokes before the age of 60, progressive cognitive dysfunction, and behavioral changes.
CADASIL is inherited in an autosomal dominant fashion, and most patients with the disorder have an affected parent. Approximately 90% of cases result from mutations of the < INOTCH3< I>gene, located on chromosome 19. Patients with CADASIL have significant morbidity from their ailment, and life expectancy is approximately 68 years. [40]
Migraine is also a common symptom in other genetic vasculopathies, including 2 autosomal dominant disorders: (1) RVCL (retinal vasculopathy with cerebral leukodystrophy), which is caused by mutations in the TREX1 gene, [41] and (2) HIHRATL (hereditary infantile hemiparesis, retinal arteriolar tortuosity, and leukoencephalopathy), which is suggested to be caused by mutations in the COL4A1 gene. [42] The mechanisms by which these genetic vasculopathies give rise to migraine are still unclear. [43]
Migraine precipitants
Various precipitants of migraine events have been identified, as follows:
-
Hormonal changes, such as those accompanying menstruation (common), [44] pregnancy, and ovulation
-
Stress
-
Excessive or insufficient sleep
-
Medications (eg, vasodilators, oral contraceptives [45] )
-
Smoking
-
Exposure to bright or fluorescent lighting
-
Strong odors (eg, perfumes, colognes, petroleum distillates)
-
Head trauma
-
Weather changes
-
Motion sickness
-
Cold stimulus (eg, ice cream headaches)
-
Lack of exercise
-
Fasting or skipping meals
-
Red wine
Certain foods and food additives have been suggested as potential precipitants of migraine, including the following:
-
Caffeine
-
Artificial sweeteners (eg, aspartame, saccharin)
-
Monosodium glutamate (MSG)
-
Citrus fruits
-
Foods containing tyramine (eg, aged cheese)
-
Meats with nitrites
However, large epidemiologic studies have failed to substantiate most of these as triggers, [46] and no diets have been shown to help migraine. Nevertheless, patients who identify particular foods as triggers should avoid these foods.
Although chocolate has been considered a migraine trigger, data from the PAMINA study do not support this contention. [46] Instead, it has been hypothesized that ingestion of chocolate may be in response to a craving brought on at the start of a migraine, as a result of hypothalamic activation.
Migraine and other vascular disease
People who suffer from migraine headaches are more likely to also have cardiovascular or cerebrovascular disease (ie, stroke, myocardial infarction). [47] Reliable evidence comes from the Women's Health Study, which found that migraine with aura raised the risk of myocardial infarction by 91% and ischemic stroke by 108% and that migraine without aura raised both risks by approximately 25%. [48] Migraines during pregnancy are also linked to stroke and vascular diseases. [49] A 2017 analysis of the Women's Health Study found that women who experience migraine headaches, particularly migraine without aura, may be at increased risk for hypertension. Compared with women without a history of migraine, those who experienced migraine with aura had about a 9% increased risk for hypertension while those who experienced migraine without aura had about a 21% increased risk. [50]
Migraine with aura for women in midlife has a statistically significant association with late-life vascular disease (infarcts) in the cerebellum. This association is not seen in migraine without aura. [51]
Results of a large, prospective cohort study in women indicate a consistent link between migraine and cardiovascular disease events, including cardiovascular mortality. Researchers analyzed data from more than 115,000 women, 15.2% (17,531) of whom reported a diagnosis of migraine. Over 20 years of follow-up, 1329 major cardiovascular disease events occurred and 223 women died from cardiovascular disease. After adjusting for the known risk factors, women with migraine had a significantly elevated risk for developing major cardiovascular disease (hazard ratio 1.50, 95% CI 1.33-1.69). The greatest increase in risk was for stroke (HR 1.62) and for angina/coronary revascularizations (HR 1.73). [52]
Migraine and iron
In a population-based MRI study by Kruit et al, migraineurs had increased local iron deposits in the putamen, globus pallidus, and red nucleus, compared with controls. [53] This increase in iron deposits may be explained as a physiologic response induced by repeated activation of nuclei involved in central pain processing or by damage to these structures secondary to the formation of free radicals in oxidative stress (possibly the cause of the disease becoming chronic). [54]
Migraine and sensory perception
In a study by Nguyen et al, quantitative sensory testing found significant differences in the perception of vibrotactile stimulation in patients with migraine compared with controls, including stimulus amplitude discrimination, temporal order judgment, and duration discrimination. [55]
Epidemiology
In the United States, more than 30 million people have 1 or more migraine headaches per year. This corresponds to approximately 18% of females and 6% of males. [56] Migraine accounts for 64% of severe headaches in females and 43% of severe headaches in males.
Approximately 75% of all persons who experience migraines are women. Currently, 1 in 6 American women has migraine headaches. (The reported incidence of migraine in females of reproductive age has increased over the last 20 years, but this change probably reflects greater awareness of the condition.)
The incidence of migraine with aura peaks in boys at around age 5 years and in girls at around age 12–13 years. The incidence of migraine without aura peaks in boys at age 10-11 years and in girls at age 14–17 years. [57]
Before puberty, the prevalence and incidence of migraine are higher in boys than in girls. After age 12 years, the prevalence increases in males and females, reaching a peak at age 30–40 years. The female-to-male ratio increases from 2.5:1 at puberty to 3.5:1 at age 40 years. Attacks usually decrease in severity and frequency after age 40 years, except for women in perimenopause. A study by Hsu et al suggests that women aged 40–50 years are also more susceptible to migrainous vertigo. [58] Onset of migraine after age 50 years is rare.
Race-related differences in prevalence
The prevalence of migraine appears to be lower among African Americans and Asian Americans than among whites. One study showed that among women, 20.4% of whites, 16.2% of African Americans, and 9.2% of Asian Americans met International Classification of Headache Disorders (ICHD) criteria for migraine. Similarly, in males, 8.6% of whites, 7.2% of African Americans, and 4.8% of Asian Americans were considered to have migraine.
Economic impact of migraine
The economic cost resulting from migraine-related loss of productive time in the US workforce is more than $13 billion per year, most of which is in the form of reduced work productivity. In the American Migraine Study, more than 85% of women and 82% of men with severe migraine had some headache-related disability. Migraineur men required 3.8 bed-rest days per year, whereas women required 5.6 bed-rest days per year. [59]
International statistics
The World Health Organization (WHO) estimates the worldwide prevalence of current migraine to be 10% and the lifetime prevalence to be 14%. The adjusted prevalence of migraine is highest in North America, followed by South and Central America, Europe, Asia, and Africa. [23]
Approximately 3000 migraine attacks per million persons worldwide occur every day. According to the WHO, migraine is 19th among all causes of years lived with disability.
In the United States, migraine prevalence is inversely correlated with household income and level of education. Internationally, however, a relationship between migraine and socioeconomic status is not present.
Prognosis
Migraine is a chronic condition, but prolonged remissions are common. One study showed that among persons who had migraine during childhood, 62% were migraine free for more than 2 years during puberty and as young adults but that only 40% were still migraine free at age 30 years. [60]
The severity and frequency of migraine attacks tend to diminish with increasing age. After 15 years of suffering migraines, approximately 30% of men and 40% of women no longer have migraine attacks.
Migraine and vascular disorders
Migraine and ischemic strokes reportedly occur in 1.4-3.3 per 100,000 population and account for 0.8% of total strokes. Milhaud et al showed that in young patients (< 45 y) with active migraine who had suffered ischemic stroke, risk factors such as patent foramen ovale, female gender, and oral contraceptive use were much more likely to be present; posterior circulation stroke was characteristic. Surprisingly, older patients characteristically lacked vascular risk factors (ie, previous hypertension, ischemic heart disease, cigarette smoking). [61]
Even in patients older than 45 years, women with migraine are more likely to suffer from ischemic stroke.
Migraineurs, male and female, have a 2.5-fold increased risk of subclinical cerebellar stroke and those with migraines with aura and increased headache frequency are at the highest risk. [62]
Migraineurs also have a higher incidence of adverse cardiovascular profiles (including diabetes and hypertension), and they are more likely to be smokers, have a family history of early heart attacks, and have an unfavorable cholesterol profile. The odds of an elevated Framingham risk score of coronary artery disease are doubled with migraine with aura, and women who have migraine with aura are more likely to be using oral contraceptives. [63, 64]
The Women's Health Study, which included professional women older than 45 years, showed that any history of migraine is associated with a higher incidence of major cardiovascular disease and that the highest risk is associated with migraine with aura, with a 2.3-fold risk of cardiovascular death and a 1.3-fold risk of coronary vascularization. [65] However, those who have migraine without aura have the same risks as the general population.
These findings have been confirmed in a population-based study by Bigal et al. [66] Similarly, a study by Gudmundsson et al found that men and women who have migraine with aura are at a higher risk for cardiovascular and all-cause mortality than are those without headache. [67]
Patient Education
Patient education is key to successful long-term management. Migraine is a chronic neurologic disorder that requires a lifestyle change at some level.
For patient education information, see the Headache and Migraine Center, as well as the following:
-
Migraine headache. Example of a visual migraine aura as described by a person who experiences migraines. This patient reported that these visual auras preceded her headache by 20-30 minutes.
-
Migraine headache. Example of a central scotoma as described by a person who experiences migraines. Note the visual loss in the center of vision.
-
Migraine headache. Example of a central scotoma as described by a person who experiences migraine headaches. Again note the visual loss in the center of vision.
-
Migraine headache. Example of visual changes during migraine. Multiple spotty scotomata are described by a person who experiences migraines.
-
Migraine headache. Frank visual field loss can also occur associated with migraine. This example shows loss of the entire right visual field as described by a person who experiences migraines.
-
International Headache Society criteria for migraine without aura.
-
Overview of migraine treatment. Five steps.
-
International Headache Society (IHS) classification of secondary headaches.
Tables
Moderate |
Severe |
Extremely Severe |
NSAIDs |
Naratriptan |
DHE (IV) |
Isometheptene |
Rizatriptan |
Opioids |
Ergotamine |
Sumatriptan (SC,NS) |
Dopamine antagonists |
Naratriptan |
Zolmitriptan |
Lasmiditan |
Rizatriptan |
Almotriptan |
|
Sumatriptan |
Frovatriptan |
|
Zolmitriptan |
Eletriptan |
|
Almotriptan |
DHE (NS/IM) |
|
Frovatriptan |
Ergotamine |
|
Eletriptan |
Dopamine antagonists |
|
| Zavegepant intranasal | Zavegepant intranasal | |
Dopamine antagonists |
Lasmiditan |
|
DHE=Dihydroergotamine; NSAIDs=nonsteroidal anti-inflammatory drugs |
||
First line |
High efficacy |
Beta blockers Tricyclic antidepressants Divalproex Topiramate |
Low efficacy |
Verapamil |
|
Second line |
High efficacy |
Methysergide Flunarizine MAOIs CGRP inhibitors Botulinum toxin |
Unproven efficacy |
Cyproheptadine Gabapentin |
|
MAOIs = monoamine oxidase inhibitors |
||
Comorbid Condition |
Medication |
Hypertension |
Beta blockers |
Angina |
Beta blockers |
Stress |
Beta blockers |
Depression |
Tricyclic antidepressants, SSRIs |
Overweight |
Topiramate, protriptyline |
Underweight |
Tricyclic antidepressants (nortriptyline, protriptyline) |
Epilepsy |
Valproic acid, topiramate |
Mania |
Valproic acid |
SSRIs = selective serotonin reuptake inhibitors |
|

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Approach Considerations
- Emergency Department Considerations
- Reduction of Migraine Triggers
- Nonpharmacologic Therapy
- Abortive Therapy
- Prophylactic Therapy
- Status Migrainosus Treatment
- Treatment of Menstrual Migraine
- Complementary and Alternative Treatments
- Surgical Care
- Diet
- Activity
- Novel Treatments and Future Drugs
- Show All
- Guidelines
- Medication
- Medication Summary
- Serotonin 5-HT1F Agonists (Ditans)
- Serotonin 5-HT-Receptor Agonists (Triptans)
- Ergot Derivatives
- Analgesics, Other
- Opioid Analgesics
- NSAIDs
- Analgesics, Opioid Combos
- Analgesics, Other Combos
- Analgesics, Barbiturates Combos
- Antipsychotics, Phenothiazine
- Anticonvulsants
- Antihistamines, 1st Generation
- Beta Blockers, Beta-1 Selective
- CGRP Monoclonal Antibodies
- CGRP Receptor Antagonists
- Tricyclic Antidepressants
- Calcium Channel Blockers
- Antidepressants, SSRIs
- Antiemetic Agents
- Neuromuscular Blocker, Botulinum Toxins
- Show All
- Questions & Answers
- Media Gallery
- Tables
- References





