Background
Electrical injuries, although relatively uncommon, are inevitably encountered by most emergency physicians. Adult electrical injuries usually occur in occupational settings, whereas children are primarily injured in the household setting. The spectrum of electrical injury is broad, ranging from minimal injury to severe multiorgan involvement to death.
Electrical injuries are shown in the images below.


Approximately 1000 deaths per year are due to electrical injuries in the United States, with a mortality rate of 3-5%. [1] Classifications of electrical injuries generally focus on the power source (lightning or electrical), voltage (high or low voltage), and type of current (alternating or direct), each of which is associated with certain injury patterns.
This article reviews the pathophysiology, diagnosis, and treatment of electrical injuries caused by manufactured electricity; for further information on lightning injuries, please see Lightning Injuries.
Medicolegal concerns
Litigation concerning occupational injuries is to be expected, but law suits against practitioners in such cases are rare. Detailed documentation of the presence of electrical burns, including diagrams, can be extremely helpful. Obtain photographic records of injuries, with proper consent, if possible.
Pathophysiology
Electricity is generated by the flow of electrons across a potential gradient from high to low concentration through a conductive material. The voltage (V) represents the magnitude of this potential difference and is usually determined by the electrical source. The type and extent of an electrical injury is determined by voltage, current strength, resistance to flow, the duration of contact with the source, the pathway of flow, and the type of current (ie, direct or alternating).
Voltage
Electrical injuries are typically divided into high-voltage and low-voltage injuries, using 500V or 1000V as the cutoff. High morbidity and mortality has been described in 600V direct current injury associated with railroad "third rail" contact. [2] In the United States and Canada, typical household electricity provides 110V for general use and 240V for high-powered appliances, while industrial electrical and high-tension power lines can have more than 100,000V. [3] Voltage is directly proportional to current and indirectly proportional to resistance, as expressed by Ohm's Law:
V = I X R; where I = current, V = voltage, R = resistance.
Current
The volume of electrons flowing across the potential gradient is the current, which is measured in amperes (I). It is a measure of the amount of energy that flows through a body. Energy is perceptible to the touch at a current as low as 1 mA. A narrow range exists between perceptible current and the "let go" current: the maximum current at which a person can grasp and then release the current before muscle tetany makes it impossible to let go. The "let go" current for the average child is 3-5 mA; this is well below the 15-30 A of common household circuit breakers. For adults, the "let go" current is 6-9 mA, slightly higher for men than for women. Skeletal muscle tetany occurs at 16-20 mA. Ventricular fibrillation can occur at currents of 50-100 mA. [4]
Resistance
The impedance to flow of electrons across a gradient is the resistance (R) and varies depending on the electrolyte and water content of the body tissue through which electricity is being conducted. Blood vessels, muscles, and nerves have high electrolyte and water content, and thus low resistance, and are good conductors of electricity–better than bone, fat, and skin. [5] Heavily calloused areas of skin are excellent resistors, whereas a moderate amount of water or sweat on the skin surface can decrease its resistance significantly.
Type of circuit
Electrical current can flow in 1 of 2 types of circuits: direct current (DC) or alternating current (AC), in which the flow of electrons changes direction in rhythmic fashion. AC is the most common type of electricity in homes and offices, standardized to a frequency of 60 cycles/sec (Hz).
High-voltage DC often causes a large single muscle contraction that throws the victim away from the source, resulting in a brief duration of contact with the source flow. In contrast, AC of the same voltage is considered to be approximately 3 times more dangerous than DC, because the cyclic flow of electrons causes muscle tetany that prolongs victims' exposure to the source. Muscle tetany occurs when fibers are stimulated at 40-110 Hz; the standard 60 Hz of household current is within that range. If the source contact point is the hand, when tetanic muscle contraction occurs the extremity flexors contract, causing the victim to grasp the current and resulting in prolonged contact with the source.
Table. Physiologic Effects of Different Electrical Currents (Open Table in a new window)
Effect |
Current (milliamps) |
Tingling sensation/perception |
1-4 |
Let-go current – Children |
3-4 |
Let-go current - Women |
6-8 |
Let-go current – Men |
7-9 |
Skeletal muscle tetany |
16-20 |
Respiratory muscle paralysis |
20-50 |
Ventricular fibrillation |
50-120 |
Types of electrical burns
Depending on the voltage, current, pathway, duration of contact, and type of circuit, electrical burns can cause a variety of injuries through several different mechanisms.
A histologic picture of an electrical burn is shown below.
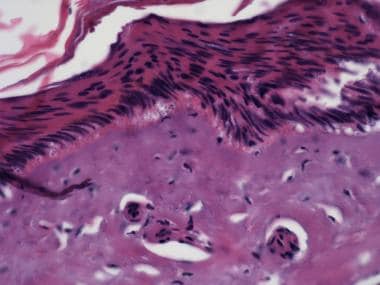 A histologic picture of an electrical burn showing elongated pyknotic keratinocyte nuclei with vertical streaming and homogenization of the dermal collagen (40X). Courtesy of Elizabeth Satter, MD.
A histologic picture of an electrical burn showing elongated pyknotic keratinocyte nuclei with vertical streaming and homogenization of the dermal collagen (40X). Courtesy of Elizabeth Satter, MD.
Direct contact
Current passing directly through the body will heat the tissue causing electrothermal burns, both to the surface of the skin as well as deeper tissues, depending on their resistance. It will typically cause damage at the source contact point and the ground contact point. Contact burns are shown in the image below.
 Contact electrical burns, 120-V alternating current nominal. The right knee was the energized side, and the left was ground. These are contact burns and are difficult to distinguish from thermal burns. Note entrance and exit are not viable concepts in alternating current.
Contact electrical burns, 120-V alternating current nominal. The right knee was the energized side, and the left was ground. These are contact burns and are difficult to distinguish from thermal burns. Note entrance and exit are not viable concepts in alternating current.
Electrical arcs
Current sparks are formed between objects of different electric potential that are not in direct contact with each other, most often a highly charged source and a ground. The temperature of an electrical arc can reach 2500-5000o C, resulting in deep thermal burns where it contacts the skin. These are high-voltage injuries that may cause both thermal and flame burns in addition to injury from direct current along the arc pathway.
Flame
Ignition of clothing causes direct burns from flames. Both electrothermal and arcing currents can ignite clothing.
Flash
When heat from a nearby electrical arc causes thermal burns but current does not actually enter the body, the result is a flash burn. Flash burns may cover a large surface area of the body but are usually only partial thickness.
Etiology
Electrical injury occurs when a person becomes part of an electrical circuit or is affected by the thermal effects of a nearby electrical arc. Injuries are caused by high-voltage AC, low-voltage AC, or DC.
High-voltage AC
High-voltage injuries most commonly occur from a conductive object touching an overhead high-voltage power line. In the United States, most electric power is distributed and transmitted by bare aluminum or copper conductors, which are insulated by air. If the air is breached by a conductor, (eg, an aluminum pole, antenna, sailboat mast, crane), any person touching the conductor can be injured. Occupational injuries may include direct contact with electrical switching equipment and energized components.
Low-voltage AC
Generally, 2 types of low-voltage injury occur: children biting into electrical cords producing lip, face, and tongue injuries, or the adult who becomes grounded while touching an appliance or other object that is energized. The latter type of injury is decreasing with the increasing use of ground fault circuit interrupters (GFCIs) in circuits where people might easily become grounded. GFCIs stop current flow in the event of a leakage current (ground fault) if the ground fault is greater than 0.005 amps (0.6 W at 120V).
Direct current (DC)
DC injuries are generally encountered when the third energized rail of an electrical train system is contacted while the person is grounded. This sets up a circuit of electric current through the victim, causing severe electrothermal burns and myonecrosis. [2]
Epidemiology
US frequency
Electrical injuries are estimated to cause approximately 500-1000 deaths per year in the United States. [3, 4] They are responsible for 3-5% of all burn unit admissions and cause 2-3% of emergency department burn visits in the pediatric population.
Some evidence exists that the incidence of low-voltage injuries among children is declining, perhaps because of widespread use of ground fault circuit interrupters (GFCIs), but rates of high-voltage injuries, usually involving power lines or rail sources, has remained steady. [6] Due to the nature of occupational hazards with electricity, electrical injuries represent the fourth leading cause of work-related traumatic death (5-6% of all workers' deaths). [7]
Race
No racial susceptibility to electrical burns exists. Occupational trends indicate that tradespeople in high-risk occupations are disproportionately white; therefore, this group may be more likely than other races in the United States to experience occupation-related electrical injuries.
Sex
Rates of childhood electrical injury are higher among boys than girls [6] ; rates of adult injury are significantly higher in men than in women, likely because of occupational predisposition. Most series show more than 80% of electrical injuries occur in men. [8, 9, 10, 11, 12]
Age
A bimodal distribution of electrical injuries exists among the very young (children < 6 y) and among young and working-aged adults. [13] Patterns of electrical injury vary by age (eg, low-voltage household exposures among toddlers and high-voltage exposures among risk-taking adolescents and via occupational exposure). [12, 13, 14]
Prognosis
For those without prolonged unconsciousness or cardiac arrest, the prognosis for recovery is excellent. Burns and traumatic injuries continue to cause the majority of the morbidity and mortality from electrical injuries.
Morbidity and mortality are largely affected by the particular type of electrical contact involved in each exposure. Overall mortality is estimated to be 3-15%. [1, 8] Flash burns have a better prognosis than arc or conductive burns. [5]
Persons who experience low-voltage injuries without immediate cardiac or respiratory arrest have low mortality, but there may be significant morbidity from oral trauma in children who bite electrical cords [15] or adults who suffer burns to the hand.
Persons who experience low-voltage injuries with cardiac or respiratory arrest may recover completely with immediate CPR on scene; however, prolonged CPR and transport time may result in permanent brain damage.
High-voltage injuries often produce severe burns and blunt trauma. Patients are at high risk of myoglobinuria and renal failure. Burns are often ultimately much worse than they initially appear in the ED.
Patient Education
For patient education resources, see the patient education article Thermal (Heat or Fire) Burns.
-
Arcing electrical burns through the shoe around the rubber sole. High-voltage (7600 V) alternating current nominal. Note cratering.
-
Contact electrical burn. This was the ground of a 120-V alternating current nominal circuit. Note vesicle with surrounding erythema. Note thermal and contact electrical burns cannot be distinguished easily.
-
Contact electrical burns, 120-V alternating current nominal. The right knee was the energized side, and the left was ground. These are contact burns and are difficult to distinguish from thermal burns. Note entrance and exit are not viable concepts in alternating current.
-
Electrical burns to the hand.
-
Electrical burns to the foot.
-
High-voltage electrical burns to the chest.
-
Superficial electrical burns to the knees (flash/ferning).
-
Energized site of low-voltage electrical burn in a 50-year-old electrician.
-
Grounded sites of high-voltage injury on the chest of a 16-year-old boy who climbed up an electric pole.
-
Energized site of the high-voltage injury depicted in Media File 9 (16-year-old boy who climbed up an electric pole).
-
Entrance site of a low-voltage injury.
-
Grounded sites of a low-voltage injury in a 33-year-old male suicide patient.
-
Grounded site of a low-voltage injury in the same 33-year-old male patient depicted in Media File 12.
-
Grounded sites of low-voltage injury on the feet.
-
A histologic picture of an electrical burn showing elongated pyknotic keratinocyte nuclei with vertical streaming and homogenization of the dermal collagen (40X). Courtesy of Elizabeth Satter, MD.
Tables
Effect |
Current (milliamps) |
Tingling sensation/perception |
1-4 |
Let-go current – Children |
3-4 |
Let-go current - Women |
6-8 |
Let-go current – Men |
7-9 |
Skeletal muscle tetany |
16-20 |
Respiratory muscle paralysis |
20-50 |
Ventricular fibrillation |
50-120 |








