Background
Although dysbarism includes problems associated with high altitude and aerospace endeavors, dysbarism also relates to the increasing pressures of descending under water that are usually experienced in free or assisted dives. Exposure to the physiologic effects of pressure during descent also can be experienced in submarines during emergencies and in tunneling projects.
Since 4500 BCE, humans have engaged in free (breath-hold) diving to obtain food and substances from shallow ocean floors at depths of 100 ft or more. The 2007 record-setting breath-hold unlimited dive of Herbert Nitsch to 702 ft (214 m) (21.7 ATM) attests to this human feat. [1] At this depth, the lungs are only 4.6% of their normal size. To emphasize the extreme nature of this record, Mr. Nitsch attempted to break his own record on June 6, 2012. He descended to a depth of 819 ft (250 m) (25.2 ATM). However, on ascent, he blacked out due to narcosis and had an uncontrolled ascent to 33 ft (10 m), where rescue divers were prepositioned. He suffered severe neurologic decompression sickness. [2]
Humans began experimenting with crude diving bells as early as 330 BCE. These bells were submerged containing only air. In 1690, the first diving bell with a replenishing air supply was tested. The first crude underwater suit dates back to 1837, and helium was first used in place of nitrogen in 1939.
All of these early diving methods required a physical connection to a support platform or boat. The Aqua-Lung, developed by Cousteau and Gagnan in 1943, and the submarine escape appliances, developed by Momsen and Davis in the 1930s, were the forerunners of today's self-contained underwater breathing apparatus (SCUBA) that frees divers from the limitations of tethering.
The increasing popularity of scuba diving and growth of commercial diving is increasing the incidence of exposures to deep pressures. Moreover, even far from the coasts, more individuals are diving in quarries, lakes, rivers, and caves. Add to this the ability to travel rapidly from anywhere in the world in a matter of hours (and the exacerbation of dysbarism caused by decreased pressures in flight), and the potential for dysbaric events can be appreciated. For these reasons, all physicians, especially emergency physicians, worldwide should maintain an expectation and knowledge of the physiologic effects and management of dysbaric injuries.
Pathophysiology
The effects of increasing pressure occur only on compressible substances in the body. The human body is made primarily of water, which is noncompressible. The gases of hollow spaces and viscous organs and those dissolved in the blood, however, are at the mercy of pressure changes. The physical characteristics of gases are described by the 4 gas laws. It is these laws that quantify the physics and problems involved in descending under water.
The Boyle law
PV = K
(P = pressure, V = volume, K = a constant)
At a constant temperature, the volume of a perfect gas varies inversely with the pressure. Similarly, the pressure varies inversely with the volume. Simply stated, this means that if the pressure is doubled, the volume is halved and vice versa.
Boyle's problem
Every 33 ft of descent increases the pressure by 1 atm. Therefore, lung volume during a breath-hold dive at 33 ft is one half that at the surface. At 66 ft, it is one third that at the surface; at 99 ft, it is one quarter; and, at 132 ft, it is one fifth. Similarly, going from 99 ft to the surface without venting (exhaling) would cause the lungs, with minimal ability to expand further, to increase pressure to three times normal, with the greatest change occurring in the last 33 ft, where it would double. This is the key law explaining the pressurization issues and injuries described in this article. [3] Also see the images below.
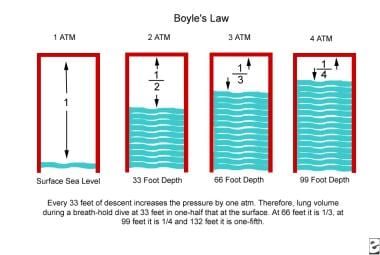 The Boyle gas law. Every 33 ft of descent increases the pressure by 1 atm. Therefore, lung volume during a breath-hold dive at 33 ft is one half that at the surface. At 66 ft, it is one third that at the surface; at 99 ft, it is one quarter; and at 132 ft, it is one fifth.
The Boyle gas law. Every 33 ft of descent increases the pressure by 1 atm. Therefore, lung volume during a breath-hold dive at 33 ft is one half that at the surface. At 66 ft, it is one third that at the surface; at 99 ft, it is one quarter; and at 132 ft, it is one fifth.
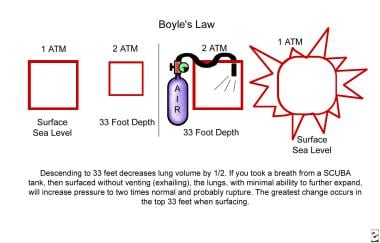 The Boyle gas law. Descending to 33 ft decreases lung volume by one half. If an individual takes a breath from a SCUBA tank, then surfaces without venting (exhaling), pressure in the lungs, with minimal ability to further expand, increases to twice normal, which probably causes rupture. The greatest change occurs in the top 33 ft when surfacing.
The Boyle gas law. Descending to 33 ft decreases lung volume by one half. If an individual takes a breath from a SCUBA tank, then surfaces without venting (exhaling), pressure in the lungs, with minimal ability to further expand, increases to twice normal, which probably causes rupture. The greatest change occurs in the top 33 ft when surfacing.
The Dalton law
For an in-depth discussion on the Dalton law, please see the article on Decompression Sickness (DCS).
The Henry law
For an in-depth discussion on the Henry law, please see the article on Decompression Sickness.
The Charles law
V1/V2 = T1/T2 (for a gas at constant pressure)
P1/P2 = T1/T2 (for a gas at constant volume)
(V = volume of gas, P = pressure, T = temperature, 1 = initial, 2 = final)
At a constant pressure, the volume of a given mass of a perfect gas varies directly with the absolute temperature. Simply stated, this means that decreasing temperature decreases pressure.
Charles's problem
A closed diving bell descending will have a decrease in pressure due to a decrease in temperature. An open diving bell will have a decrease in volume as it descends due to pressure and decreased temperature.
Organ involvement
The areas affected by the Boyle law can be divided into compressible and noncompressible spaces. Compressible spaces include the lungs, the hollow viscera of the gastrointestinal system, and the space behind the facemask. Examples of noncompressible spaces include the sinuses, air spaces in tooth fillings, middle ear canals, and occluded external ear canals.
Neurologic
Although less common, several case reports have noted patients presenting to the ED with cervical artery dissections secondary to diving. [4] Focal neurologic findings on examination may warrant further imaging and evaluation.
For more information, see the Medscape Reference articles Carotid Artery Dissection and Veterbral Artery Dissection.
Concomitant decompression sickness (DCS)
The same situations that may cause overpressurization injury also may result in DCS. Therefore, any diver who experiences ringing or roaring in the ears, loss of hearing, vertigo, dizziness, nausea, or vomiting during or shortly after a decompression dive or a dive near the no-decompression limits should be presumed to have inner-ear DCS.
Any symptom that occurs after diving (from minutes to days) should be presumed to be related to diving. Other symptoms of DCS include paresis, paralysis, paresthesia, joint pain, dyspnea, and rash. For more information on this topic, please see the article on Decompression Sickness.
Pulmonary
As an individual descends, the lungs decrease in size according to the Boyle law. This is true only if the diver is holding his or her breath. When former breath-hold record-holder Ferreras-Rodriguez went to 417 ft, his 50-inch chest decreased to 20 inches. In the process, hemoptysis can occur when the lung volume decreases below the residual volume. Since a scuba diver breathes from a compressed air source, the loss of volume from depth is negated.
Early diving instruction recommended a rate of ascent no faster than 60 ft (18 m) per minute. The more recent recommendation was to ascend no faster than 30 ft (10 m) per minute and to make a 3-5 minute safety stop at 15-20 ft. [5] Normally, divers are taught to ascend no faster than a rate of 1 ft per second, with newer recommendations being even slower (one half ft/s or slower). They also are instructed to breathe normally during ascent. This slow rate of ascent allows for a gradual offloading of nitrogen and emptying of air-filled spaces (eg, the lungs).
One or more additional stops at deeper level(s) are likely needed to lengthen ascent time adequately and thus protect against decompression sickness (DCS). Research has shown that a safety stop at 50 ft (15 m) of 2.5-5 minutes in addition to another stop at 20 ft (6 m) for 3-5 minutes will decrease venous bubble formation at least for a no-decompression dive of 82 ft (25 m). The supposition here is that this can decrease the risk of DCS. [5] Obviously, this requires that more of the air reserve is allotted for the ascent. In addition, premeasured weighted ropes attached to the diving platform for the set safety stops can help maintain the desired depth and prevent drifting away from the surface vessel. Additional scuba tanks could be added at each safety level in case diver air supplies reach a critical level.
A too-rapid ascent, especially if emptying of the lungs is incomplete, causes the lung volume to expand rapidly. The musculoskeletal cage limits expansion, which then causes overpressurization of the lungs, known as pulmonary overinflation syndrome. A limit is reached beyond which damage will occur. Resulting injuries include pneumothorax, pneumomediastinum, subcutaneous emphysema, and rupture into the pulmonary vein causing a large arterial gas embolism (AGE). [6, 7] A pulmonary arteriovenous malformation allows a dysbaric injury to cause a cerebral air embolism. Air embolism and the effects of nitrogen bubble embolization are discussed in the article on Decompression Sickness.
It has been found that during training, there is a higher incidence of pulmonary barotrauma when compared to normal nontraining dives. This risk is even further exacerbated by practice of an emergency free ascent, a maneuver only used if there is a sudden interruption in air supply (eg, run out of air). [8]
Training is essential to avoid injuries caused by overpressurization. In one study, more than 41,000 simulated submarine escape ascents were performed from 30 ft and 60 ft. No pulmonary barotrauma occurred, and a low (4%) incidence of middle ear barotrauma occurred. Of the 4% who experienced middle ear barotrauma, only 2.1% experienced tympanic membrane rupture. The authors of the study note that medical screening and quality training are essential for the program's success. [9]
Pulmonary edema is an uncommon complication associated with cold water diving, especially in combination with heavy exertion. [10] Pulmonary edema has also been described in warm water scuba diving. [11]
People who have asthma are susceptible to pulmonary complications from extremes in atmospheric pressure because of the lung's ability or inability to release the air it contains. [12] In one survey, 10% of participants in scuba diving reported a history of asthma. Forced vital capacity and forced expiratory volume have both been shown to be adversely affected in people with asthma. Decreased forced vital capacity and forced expiratory volume can lead to air-trapping and increases the risk of barotrauma and arterial gas embolism (see Decompression Sickness). [13] Decreased peak expiratory flow (PEF) has been documented in recreational divers in tropical waters who had a history of asthma. [14, 15] If sudden bronchospasm, ie, constriction of the bronchiole tubes, were to occur while diving, the sudden shortness of breath could cause aspiration and the possibility of an uncontrolled panic ascent. The constriction can also make it difficult for distal airways to offload pressure. On ascent, this could lead to rupture of the alveoli, which can result in pneumothorax, collapse of a lung, which worsens the shortness of breath. The worst cases can culminate in a tension pneumothorax, which interferes with blood flow, or AGE. For more information on AGE, see the article Decompression Sickness. There are a number of reasons why bronchospasm can occur. Instigating factors can be the stress or exercise involved with diving, dry air supply, concentration of pollens in the tanks during filling, aspiration of sea water, or cold stimulation. [16] Another risk in asthmatics is that over the long term, chronic inflammation of the airways can cause a loss of the elasticity. This stiffer lung is more prone to over pressurization and subsequent injury. Individuals with significant history of childhood asthma, for similar reasons, can have smaller than chest-size lungs. These stiff lungs can then expand within the chest and succumb to pressure injuries. [17]
Sports may cause long-term exacerbation of asthma. Still, the percentage of divers with asthma is comparable to the general population, and the frequency of complications from asthma remains low. Although the risk of pulmonary barotrauma is increased, this risk appears to be small. [18] While many individuals with asthma do dive without problems worldwide, to decrease the risk, the individuals should be cleared for diving by a physician knowledgeable in both asthma and the unique environment and challenges of SCUBA diving. Before diving, a thorough history and physical, along with spirometry and allergy testing, should be performed. A particular search should be done for asthma with triggers of inducement by exercise, cold, or stress, which could disqualify a diver. Consideration can be made for bronchial provocation challenge testing with methacholine and mannitol, understanding the limitations of this type of testing. Clearly, common sense would dictate that any diver, not just asthmatic persons, should not dive with upper or lower respiratory symptoms. [19] An additional recommendation is for asthmatic individuals not to dive if they have had to use their rescue albuterol inhaler within 48 hours of a scheduled dive. [16] People with well-controlled asthma and normal airway function and reactivity are not likely to be at an increased risk. [20] Under the right circumstances, patients with asthma can safely participate in recreational diving without any apparent increased risk of an asthma-related event. [18]
One of the concerns about children and SCUBA diving relates to the need to follow strict guidelines and protocols and to stay focused on the activity. Too rapid an ascent and/or failure to exhale properly can lead to the pulmonary barotrauma mentioned above. In addition, statistically significant decreases in pulmonary function have been documented in children with cold-air breathing and with diving. This change appeared to be most significant in lower-body-weight/BMI children. [21]
As with the potential for air-trapping in asthmatic persons, individuals with pulmonary blebs (bullae) also have reasons to be concerned. Upon descending, the blebs are compressed, but once at depth, they return to the predive size. However, during ascent the air does not easily leave the bleb, which causes an increase in size. Upon repeated dives, the size of the bleb gradually increases. When the wall of the bleb is thin enough, a rupture and subsequent pneumothorax can occur. [22]
Because of the risks involved with scuba diving, everyone with a history of pulmonary conditions should have an evaluation by a healthcare provider specializing in diving medicine, and they should heed the specialist's recommendations.
Ear squeeze
Dysbarism most commonly affects the ears. Ear barotrauma is the most common barotrauma complaint of SCUBA divers. [23] The eustachian tube functions to equalize middle ear and ambient environment pressures. Rapid descent increases external pressure on the tympanic membrane and requires the diver to increase air pressure in the pharynx to equalize. Most people have experienced discomfort with a breath-hold dive to the bottom of a pool of just 4-6 ft (1.5-2 m). Deeper descent without equalizing (see Deterrence/Prevention) causes barotrauma. [24] Middle-ear barotitis occurs from failure to equalize pressures adequately and results in pain. Large pressure differences can stretch the tympanic membrane excessively and cause hemorrhage or rupture. Large variances can also damage the ossicles and round window. [25]
It has also been hypothesized that excessive nasopharyngeal air pressure (from equalizing) can cause damage to not only the middle ear and adjacent structures, but also the eustachian tube itself. This effect was more prevalent when in unilateral equalization issues causing excessive positive pressure in the normal ear. [26]
On ascent, if air is not allowed to pass from the middle ear through the eustachian tube, a pressure imbalance occurs. At extremes, a hemorrhagic tympanum, or even rupture, can result. Too-rapid ascent and descent or preexisting infection or inflammation are the most common causes of internal ear injuries.
If the tympanic membrane develops extreme bulging, without rupture, a facial palsy can occur. One exception to paresis post dive being considered for DCS is facial nerve baroparesis. It is a rare condition that results in unilateral palsy (paralysis) of the facial muscles. [27] It occurs from prolonged overpressurization of the middle ear due to eustachian tube dysfunction and a deficient facial nerve canal. [28] Normally, a very thin bone wall separates the facial nerve from the middle ear. This can undergo spontaneous dehiscence. Dehiscence of the facial nerve in its intramastoid portion occurs in 0.5-57% of temporal bone, though a lower incidence is found intraoperatively. As the pressure increases, blood flow through the capillaries of the vasa nervorum to the facial nerve decreases, causing neurapraxia in the nerve. If there is no issue with the facial nerve canal, it may also occur from pressure transmitted through the fenestra of the chorda tympani. [29, 30, 31] In one report, it was associated with pain and decreased hearing on the same side. [32] Symptoms that can accompany the facial paralysis include same-side pressure, otalgia, loss of hearing, tinnitus, altered sensation of the tongue, or alternobaric vertigo from asymmetric middle ear pressures. [29] This same presentation could also result from decompression sickness, arterial gas embolism, stroke, or Bell palsy. However, a persistent palsy should be investigated and treated as DCS. To help differentiate facial baroparesis from DCS, the dive profile should be considered for the potential of DCS, or uncontrolled ascent. [29, 33]
Middle-ear barotitis usually is self-limited in that when the middle ear pressure is relieved, the pressure on the nerve resolves and the symptoms reverse. However, since the symptoms could also be caused by the serious causes already mentioned, timely medical care is advised. An isolated facial palsy due to a DCS is unlikely to occur without any other symptoms or signs. If it is from over-pressurization of the middle ear, it occurs on ascent. Clinical examination could reveal a tympanic membrane that is injected, bulging, hemorrhagic, or with an effusion, or a hemotympanum or perforation. [29] The palsy resolves quickly after the pressure is relieved with myringotomy. [33]
External ear issues also can occur. External ear squeeze also can occur if cerumen or other obstruction (eg, tight-fitting hood) occludes the canal. The most common ENT (ear-nose-throat) complaint in divers is external otitis. This can occur from prolonged water contact and the epithelial changes and/or from contaminants in the water. Exostosis of the external auditory canal has also been described from prolonged dives in cold water, as would be common in commercial divers. [23]
Frequent scuba dives (4 dives per day on 5 consecutive days) have been shown to cause damage to ear structures when evaluated with tympanometry and otoscopic examination. These cumulative effects were not seen when surface intervals exceeded 11 hours. Therefore, extending surface intervals may offer protection against middle-ear barotrauma in recreational scuba diving. [34] Another study found no statistical differences between divers and the nondiver controls. They implied the existence of a transient effect that diminishes the longer the elapsed time since the dive. [35] After 6 days of diving in the Red Sea, tympanic membrane injury was found in 36.5% of 28 divers. The incidence increased with the total number of dives per day, not depth or duration of the dive. Experienced divers (more than 200 lifetime dives) showed less evidence of injury. [36] Lack of experience, and perhaps condensed training, as a risk factor for middle-ear barotrauma has been additionally confirmed. [37] Injury can be experienced not just on ascent, but also on descent, due to overpressurization if the pressure is not frequently equalized using Valsalva-type maneuvers. [38]
Similar evidence of tympanic membrane injury (mild-to-severe hemorrhage or rupture) from barotrauma has also been found in patients receiving repeated hyperbaric oxygen (HBO) treatments. Examination of the tympanic membrane via otoscopy immediately following an HBO "dive" is recommended to determine the need for prophylaxis or discontinuation of the activity. [39] A similar recommendation appears reasonable after scuba diving.
If the round window membrane is ruptured, inner ear barotrauma is the result. Inner ear barotrauma is frequently associated with middle ear over-pressurization on ascent, but has been documented on descent. [38] This causes rupture of the round window and resultant trauma to the inner ear structures. The injuries can include perilymph fistula formation, intralabyrinthine membrane tear, and hemorrhage. [40] The leading symptom is a sudden loss of hearing. Tinnitus and vertigo are less common. However, hearing loss or vertigo may not be present. Tinnitus may be the only symptom and can occur hours or even days after a dive. [41] Inner ear barotrauma can be difficult to distinguish from inner ear DCS. It requires a detailed approach that considers the events of the dive, physical assessment, pure tone audiometry, a fistula test, and electronystagmography (which tests the vestibular system). Obviously, this approach takes time. If there is any thought that it might be DCS, a diagnostic, and potentially therapeutic, HBO treatment should be rapidly pursued. Limited study data suggest that undergoing HBO treatment does not worsen inner ear barotrauma, if the diagnosis is wrong. [40, 42]
In the past, inner ear barotrauma was believed to disqualify an individual from future diving. However, individuals who completely recover from ear barotrauma may return to diving with extreme caution. [43, 44] Patients who experience inner ear barotrauma could be considered for return to diving if their symptoms are stable, without evidence of vestibular issues, and normal imaging tests (CT or MRI). [40]
As opposed to sudden hearing loss, a progressive hearing loss in the 4000- to 8000-Hz range has been described in active divers. This hearing loss is believed to result from inner ear barotrauma, DCS, or noise-induced deafness. In one survey, approximately one fourth of responding divers reported problems with hearing or tinnitus. [45] However, a more recent investigation of hearing acuity in active recreational divers failed to identify any statistically significant hearing loss with the exception of a change in air conduction at 6000 Hz. Whether this was related to diving was not clear. [46] Hearing loss associated with professional diving is believed to be related to noise or inner ear damage and not related to middle ear barotrauma. No statistical hearing changes were found in a group of sport divers.
Vertigo can result for several reasons. On descent, an obstruction of one ear canal (eg, by cerumen or a tight-fitting hood) can allow cold water to enter unilaterally, causing caloric stimulation. The inability to properly equalize middle ear pressures can cause the round window to implode and rupture. This vertigo persists even after ascending and usually is accompanied by sensorineural hearing loss and tinnitus. On ascent and, occasionally, on descent, when the differences in middle ear pressures on each side are greater, the unbalanced stimulation may cause alternobaric vertigo. This vertigo can persist for several days. Finally, vertigo may be caused by inner ear DCS. In inner ear DCS, vertigo was the major presenting complaint. In contrast to this, in dysbaric barotrauma, vertigo was not found to be the presenting complaint or a significant problem. [47] Instead, those patients complained of tinnitus and hearing loss.
For more on inner ear DCS, please see the article on Decompression Sickness.
Divers who experience inner ear DCS or barotrauma require detailed ENT diagnostic evaluation at follow-up. [48] Many divers with inner ear DCS are asymptomatic but still have significant cochleovestibular deficits. Inner ear barotrauma has a better short- and long-term outcome than inner ear DCS. [49] Alternobaric vertigo occurs more frequently in divers who have a history of otitis media or eustachian tube dysfunction at the time of diving. [50]
Divers with a history of otitis media or eustachian tube dysfunction may experience difficulty clearing their ears during diving. Otitis media dysfunction, eustachian tube dysfunction, or both can be considered risk factors for developing alternobaric vertigo. Differentiating inner ear barotrauma from inner ear DCS is difficult. Consequently, all divers who experience vertigo or tinnitus postdive should be considered for HBO therapy. Failure to treat inner ear DCS can lead to permanent disability. One study recommended bilateral tympanic paracentesis (needle through the tympanic membrane) before HBO therapy. Should barotrauma occur to the middle ear and adjacent structures, it is important to add prophylactic antibiotics to anti-inflammatory treatment to prevent infection that has penetrated adjacent boney confines causing meningitis. [51]
Sinus squeeze
The sinuses, being air-filled spaces, also have the need to equalize. Preexisting illness such as polyps or infection can interfere with the free exchange of gas. Sinus squeeze can be painful and disabling. The pressure may cause blood vessel rupture with resultant epistaxis. However, more serious can be the violation of the thin bone surrounding the sinuses. The results have included severe sinusitis extending into the boney structures, [52] orbital wall fracture, [53] pneumocephalus, [54, 55] and periorbital emphysema without radiographic etiology. [56] These cases presented with progressive, unremitting headaches. Another reported issue has been optic neuropathy from sphenoidal sinusitis due to barotrauma. [57] These cases highlight the importance of thorough evaluations for any neurologic symptoms post dive.
Trigeminal nerve baroesthesia has also been reported. Two separate branches of the maxillary division of the trigeminal nerve traverse the walls of the maxillary sinus. These are the infraorbital and posterior alveolar nerves. Overpressurization of the maxillary sinus on ascent can affect these nerves, due to decreased blood flow to them. Symptoms can include numbness, pain, or sensitivity. For the infraorbital nerve, this would be localized to the cheek. With the posterior alveolar nerve, the symptoms would be located in the upper teeth or gums. In addition, dysfunction of the sphenoid sinus can result in involvement of any of the divisions of the trigeminal nerve. The two other divisions go to the forehead and the jaw with the same symptoms. [28]
Tooth squeeze
When considering barodontalgia (tooth squeeze), it is important to recognize that many of the head and neck issues discussed before and after this section can cause referred pain leading the affected individual to believe that it is dental in origin. This is classified as indirect barodontalgia and is related to disease, such as upper respiratory tract infection or chronic sinusitis, in the air spaces such as the sinuses or ears. As these are above the oral cavity, the sensation of pain usually involves the upper teeth and as it is frequently due to an equalization issue, it is noticed on initial decent. Indirect barodontalgia from barosinusitis was reported in 9.7% of the cases of barodontalgia. [58] Clinically, there may be tenderness on percussion (tapping) of the affected sinus.
Direct barodontalgia involves the dental structures directly and results from the pressure exposure, and not pain present before, but worsened by, diving. It is most commonly related to pulp disease or issues with restorations, including fillings in cavities and crowns. Barodontalgia is more likely to occur in older or temporary fillings, leaking restorations, or in fillings with surrounding caries. Caries allow air under pressure to be forced under the filling or restoration. On ascent, the same defect does not allow air to flow out, and the expanded air puts pressure on the sensitive dentine, causing pain. This same pressure buildup has caused fracturing of teeth or restorations. [59, 60] When there is a fracture, it many times is related to a leaking restoration that allows air to get underneath it. A history of recent dental work, or tooth sensitivity, can be found.
The causes of the direct barodontalgia are classified as to the type of pain experienced, though this does not have bearing on underlying pathology. Class I, irreversible pulpitis, exhibits a sharp momentary pain on ascent. Class II, reversible pulpitis, is characterized by a dull throbbing pain on ascent. Class III, necrotic pulp, has the dull throbbing pain on descent. Class IV, periradicular (in the associated nerve), is persistent severe pain on both descent and ascent. Dental barotrauma can be also be stratified by incidence. Faulty restorations and dental caries without pulp involvement were the cause in 29.2%. Necrotic pulp or periradicular inflammation was present in 27.8%. Vital pulp pathology accounted for 13.9% of the events. Finally, recent postoperative dental treatment was the cause 11.1% of the time. [58]
The type of cement used in crown fixation is thought to contribute to the potential for loosening, dislodgement, or fracture of the involved tooth. Micro air bubbles in the cement, along with the pressure cycling of repeated dives, is thought to be the cause. The preparation of two types of cement, zinc phosphate cement and glass-ionomer cement, have porosities that allow for the trapping of the microscopic air bubbles. [58] This frequently allowed for leakage, loosening, and potential loss. The use of resin cement did not exhibit this effect, though it is very irritating to use. There are other types of cement, so it becomes important to discuss this topic with your dental professional. Methods exist to decrease the likelihood of these issues during dental work, but that discussion is beyond the scope of this article. Interested readers are referred to the References. [58, 61, 62]
The sudden suffering of dental barotrauma can lead to distraction and anxiety due to pain or gagging with possible aspiration due to the loose restoration. The barotrauma disrupted diving over a third of the time in one study. [63]
Temporomandibular joint dysfunction
SCUBA diving requires a regulator with a mouthpiece for breathing. There can be a tendency to clench your teeth during the dive due to stress or anxiety about keeping your "lifeline" in your mouth. With poor-fitting mouthpieces, possibly in conjunction with a poor bite occlusion, the abnormal forces can cause or exacerbate temporomandibular joint (TMJ) dysfunction. There also can be a tendency to shift your mandible forward with the clenching force primarily on the canines and premolars, also resulting in abnormal force on the TMJs. The clenching can stress and strain the mastication (chewing) muscles attached to the jaw. [58] A poor-fitting regulator mouthpiece and excessive teeth clenching during a dive both have caused dental fractures, which can result in TMJ dysfunction. [64]
The prevalence of TMJ dysfunction in the diving population has been reported in 24-68%, with it more common in women. It is also more prevalent when diving in cold water owing to difficulty of the lips in sealing the regulator in the mouth. [58] This leads to more forceful teeth clenching. TMJ symptoms can be localized to the joint or can radiate to the ears, teeth, or temples. Among New Zealand divers, TMJ dysfunction was the second most prevalent head and neck disorder and comprised 24% of these disorders (with ear pathology the most common disorder, comprising 65%, and nasal and sinus disorders comprising only 10% of disorders). [58] A semicustomized mouthpiece required less muscle activity for retention than commercial types, and fully customized mouthpieces are reported to cause the least mandibular displacement from the normal resting position. Thus, usage results in the least discomfort, muscle pain, fatigue, and effort. [61] However, an excessively customized mouthpiece could preclude its use in an emergency by another diver.
Headache
In a larger context, many causes of headache can be associated with scuba diving. Ear, sinus, and tooth squeeze are potential etiologies of headache caused by scuba diving. [65] However, the diving environment can lead to other causes of headache. For example, inadequate ventilation can cause retention of carbon dioxide. Contamination of the pressurized air from exhaust fumes can produce carbon monoxide toxicity. Pressure on the face from the mask or hood can irritate the facial or scalp nerves. Prolonged extension at the neck can cause impingement on the occipital nerve and result in a muscle tension headache. It has also caused neck artery dissections, as mentioned earlier. Rapid cold temperature change can also cause a headache.
Excessive exertion coupled with resultant dehydration, hypoglycemia, or both may cause a headache. The pressure environment can also trigger a migraine in patients with a prior history of migraines. Finally, the constant clenching of the regulator mouthpiece can stress the temporomandibular joint (TMJ) and cause pain that may be interpreted as earache or headache.
Etiologies covered in the article on DCS include arterial gas embolism and DCS (see Decompression Sickness). Because of the wide variety of etiologies of headache and the difficulty in differentiating them clinically, all divers with postdive headache should complete a thorough examination by a health care provider and be considered for HBO. Consideration for HBO is particularly appropriate in the presence of any focal neurologic issues.
Mask squeeze
The space between the mask and face is compressible and requires equalizing on descent.
Failure to equalize pressure creates a vacuum effect that can cause discomfort, a ring around the face that can persist for hours, frank petechiae of the face or hemorrhage into the sclerae from capillary rupture, or all of the above. Diplopia has also resulted from orbital hematoma due to mask barotrauma. [66, 67]
Eye problems
The use of hard contact lenses by divers has been found to cause the development of small bubbles in the precorneal tear film under the contact lens when going from 149 ft to 70 ft. The bubbles increase in number and size as decompression progresses. [68]
Symptoms include soreness, decreased visual acuity, and seeing halos around lights. These symptoms start at the time of bubble formation and persist for about 2 hours after returning to sea level. No bubbles were noted under the same decompression conditions when soft membrane lenses were worn. The lack of permeability of the hard lens was presumed to be the reason for bubble formation. Divers who elect to wear contact lenses while diving are advised to use soft membrane lenses.
Isolated diplopia, without other neurologic or ocular symptoms, is not consistent with decompression sickness. Mask barotrauma has been reported to cause an orbital hematoma in one diver. Physical examination and CT scan of the orbits confirmed the diagnosis. [66] In a breath-hold free diver, subcutaneous orbital emphysema has been reported with trauma or preexistent facial injuries/surgery. [69]
Gastrointestinal problems
Diving does not usually pose a major problem in the GI tract because gas present at the surface is compressed and then reexpanded to the same volume as before the dive. Occasionally, however, gas is added to the GI system during a dive. Small amounts of air may be swallowed during a dive due to the unnatural breathing from a regulator and ear and sinus pressure-equalization techniques. Certain dietary practices can add gas to the GI system. However, the amount of pressure added from dietary conditions should not be significant during an average length dive.
Bowel gas volume changes usually only cause discomfort. Preventing gas from decompressing or diffusing can lead to an overdistended pocket and the potential for rupture. Excessive amounts of gastric air or intestinal air trapped by constipated stool or external issues, such as adhesions or a too tight weight belt, can yield rupture. Cases of pneumoperitoneum and of gastric rupture specifically associated with scuba diving have been reported. [70] Pneumoperitoneum is usually the result of a ruptured hollow viscus in the abdomen. [71] In one case report, the degree of pneumoperitoneum was so great that it created tension and abdominal compartment syndrome. The patient was in shock with marked abdominal distention due to free air. The patient improved rapidly after needle decompression of the abdomen. [72]
Failure to treat in a timely manner can result in serious illness. In the pressurized environment, air can enter the abdomen from other routes such as the lung or female genital systems. Therefore, the finding of pneumoperitoneum postdiving does not always indicate a ruptured hollow viscus. A detailed workup should be performed to identify an area of rupture to avoid unnecessary surgery. Strong consideration should be given to HBO therapy during workup or prior to surgery.
Etiology
Anything that prevents free flow of air out of air-filled spaces and allows overpressurization on ascent is a cause, such as the following:
-
Asthma - Bronchospasm from breathing dry compressed air, aspirating salt water or cold water, exertion, and anxiety, anything that permits local air trapping
-
Emphysema - Air trapping disease, air blebs, abnormal gas exchange
-
Infections - Mucus plugging (localized air trapping), coughing on ascent
-
Environmental allergies - Mucosal inflammations (impeded air flow), sneezing on ascent
-
Structural lesions, pathology, obstruction, or inflammation (eg, polyps, tumors) - Nasal or sinus, external auditory canal, lungs
-
Poor training or experience and panic or anxiety - Diving when conditions listed above are present, too-rapid an ascent or inadequate pressure-equalization techniques
The principle cause of dysbarism or DCS injuries is from too-rapid an ascent. The most common cause of too-rapid ascent is panic and subsequent loss of control. With scuba diving being an unfamiliar environment, beginners are more likely to panic and less experienced to deal with urgencies that occur during a dive. A diver's tendency toward stress or panic should be of concern to instructors and dive masters. [73] During instruction, major efforts should be directed toward making the students feel comfortable in the unfamiliar environment. Anxiety or panic disorders can develop in experienced divers. Poor control of anxiety or panic disorders may disqualify the individual from continued participation in diving.
Epidemiology
Frequency
United States
Between 1987 and 2003, the Sporting Goods Manufacturers Association estimated the number of scuba divers who dive at least once a year in the United States to have risen 32.1% from 2.4 to 3.2 million participants. The peak year was 1998 at 3.5 million. However, possibly due to economic reasons, a steady decrease to 2.8 million occurred by 2012. [74] Of equal importance is the breakdown of those divers. Only about one third of divers were active or regular participants. Approximately two thirds of divers were casual divers, with many as little as a single dive in a year. [75, 76, 77, 78, 79, 80] Experience yields a safer diver, though at the other extreme over confidence can lead to pushing too close to limits.
Due to variability in reporting and collection of information, there is inconsistency in the mainstream medical journal publication of diving-related injury statistics. To improve statistical collection of information, the Divers Alert Network (DAN), based in North Carolina in the United States, acts as a medical information and referral service for diving-related injuries. In addition to this role, it provides education, acts as a clearinghouse for reports of diving-related injuries from around the world, and participates in studies related to diving injuries and illnesses. Their efforts to be the clearinghouse and repository of injury reports has been hampered in recent years, from 2003 and on, in the United States due to a change in federal law that makes medical confidentiality more stringent and thus their abilities to obtain reports and follow-up that much more difficult. They also have sponsored ongoing long-term research including a study entitled Project Dive Exploration (PDE).
According to DAN, the overall rate of diving-related injury in 2011 was 3.02 cases per 100 dives, self-reported DCS symptoms was 1.55 cases per 1,000 dives, and treated DCS was 5.72 cases per 100,000 dives. Diving-related injury and self-reported DCS symptom rates decreased for higher diver certification levels, increasing age, and increasing number of average annual dives. For men, the rates increased for increasing BMI. Diving injury rates may be higher than previously thought, indicating a greater burden on the diving community. Self-reported DCS-like symptoms are a small fraction of all dive-related injuries, and those receiving treatment for DCS are an even smaller fraction. The small number of divers seeking treatment may suggest the mild nature and a tendency towards natural resolution for most injuries. [81]
International
See Mortality/Morbidity below.
Age
Many scuba divers start out in the sport young and relatively healthy. With time, they develop medical conditions. Likewise, other divers have significant medical issues upon entering the sport. An Australian study identified that a significant prevalence of medical conditions existed in experienced divers. [82] Many conditions would be considered to disqualify these divers from future participation in scuba diving.
DAN data also notes a steadily aging trend in their data.
Prognosis
With early recognition of diving-related injuries, most individuals have good outcomes and minimal residual problems.
ENT disorders, even inner ear barotrauma, do not automatically contraindicate future diving when proper education is given and followed.
A common misconception exists that there are no efficacious treatment options for inner ear barotrauma. The first step is a full neurotological evaluation, including high-resolution CT of the temporal bones, by an ENT specialist with experience with diving-related cochleovestibular (middle and inner ear) dysbaric injuries. [83] Treatment options can range from conservative, to acute high-dose steroid administration (started within 3 wk of the injury), to surgery for perilymphatic fistula repair. [84]
The diver commonly asks when he or she can return to scuba diving. The decision is partly dictated by the presence of a significant residual sensorineural hearing loss, evidence for noncompensated vestibular damage, and CT findings of possible enhanced cerebrospinal fluid–perilymph connection. The decision is not an easy one and requires a specialist with the appropriate experience in treating diving injuries to determine the risk for recurrent inner ear injury and to communicate that adequately to the scuba diver. In addition, animal studies suggest that the use of a free radical scavenger greatly decreases symptoms.
Mortality/Morbidity
Separating mortality data for DCS from those for barotrauma is impossible. Pathologists demonstrated little knowledge of diving accidents while performing autopsies and missed the more subtle diving injuries. [85, 86]
No known data are available on the incidence of dysbaric injuries. However, the distribution of ear, nose, and sinus disorders indicates that, of 1001 disorders found in 650 divers, 64.6% were ear problems. Approximately 23.9% were related problems of the lower jaw, teeth, temporomandibular joint (TMJ), and related muscles. Finally, 3.1% of these complaints were related to the nose, 6.6% to sinuses, and 1.8% to miscellaneous problems. [87]
Dysbarism can produce some long-term morbidity, primarily in the form of hearing loss. This may be the result of tympanic membrane rupture, ear ossicle dislocation, or round window rupture. The incidence of these complications is unknown.
In a study of 709 experienced US and Australian divers, mild barotrauma was common. Findings include ear squeeze, 52.1%; sinus squeeze, 34.6%; tooth squeeze, 9.2%; tympanic membrane rupture, 5.4%; round/oval window rupture, 1.1%; subcutaneous emphysema, 0.7%; pneumothorax, 0%; arterial gas embolism, 0%; decompression sickness, 4.4%; and permanent disabilities (hearing loss, tinnitus, balance disorder), 2.3%. [88]
Several studies have tried to quantify the frequency of dental barotrauma. The German navy found increased issues with missing teeth and crown dislodgement in divers and submariners, though more so in the divers as they are exposed to greater pressure changes more frequently. Studies involving American and Australian civilians and Saudi/Kuwaiti military, divers reported incidences ranging from 9.2% to 21.6%. [58] However, in French military divers, it was found to be 5.3%. [63, 89] An additional 17-27% of divers also experienced jaw or sinus pain. In the Saudi/Kuwaiti military divers, 75% of the incidence of pain was on descent, while about 25% was on ascent. [58]
Mortality rates are as follows:
-
In South Africa, the mortality rate was found to be as low as 0.016%. [90]
-
The US military in Okinawa reported fatalities in 0.0013% (1.3 per 100,000) dives. [91]
-
A New Zealand report states that the most common cause of death was drowning, but pathologists were frequently imprecise. [86]
-
In Western Australia, the recreational diving injury morbidity rate ranges from 5-350 incidents per 100,000 dives. The mortality rate for all causes is 0.013%. The most common cause leading to death from drowning is running out of air. [92]
-
In the United States, 3-9 deaths per 100,000 dives annually occur. The most common cause of dive-related death is drowning (60%), followed by pulmonary-related illnesses.
-
Diving fatalities in the United States and Canada have fluctuated year to year but have averaged around 83 deaths over the past two decades.
-
The mortality rate is around 10-20 diving fatalities per 100,000 DAN members and increases by about one case per year.
-
In the breath-hold free-diving group, fatalities have steadily increased worldwide over the past decade to 45 in 2007. Note that only 5 or less were related to free-diving competitive activities, either training or competition. Most fatalities were during snorkeling, spear fishing, or collecting of marine specimens.
The Divers Alert Network (DAN) has reviewed diving deaths reported to them between 1992 and 2003. They look at a 4-step sequence to death that starts with a trigger, then disabling agent, followed by the disabling injury, and finally the cause of death. In the trigger category, running out of gas, entrapment, and equipment issues were the most common. Next under disabling injury, the most common were uncontrolled ascent, running out of gas, and buoyancy issues. For disabling injuries, asphyxia was the most common, followed closely by arterial gas embolism and cardiac issues. Finally, the most common listed cause of death by far was drowning. However, they remark that this is the final step and not usually the cause. The failure to be more exact is due to lack of knowledge by the pathologists doing the autopsies. Only about a quarter of the cases had a more exact cause, mostly split between arterial gas embolism and cardiovascular pathology. [93] Diving accident investigators have modified procedures for data acquisition in diving fatalities. It is recommended that final reports be delayed until all relevant diving information is known. This should include all pathological data, access to dive computer information, reenactments of incidents, postmortem CT scans, and the evaluation of tissue gases. [94]
Patient Education
Improved instruction in equalization and control of ascent minimizes future problems.
For patient education resources, visit First Aid and Injuries Center. Also, see the patient education articles Barotrauma/Decompression Sickness, Scuba Diving: Ear Pain, and The Bends - Decompression Syndromes.
-
The Boyle gas law. Every 33 ft of descent increases the pressure by 1 atm. Therefore, lung volume during a breath-hold dive at 33 ft is one half that at the surface. At 66 ft, it is one third that at the surface; at 99 ft, it is one quarter; and at 132 ft, it is one fifth.
-
The Boyle gas law. Descending to 33 ft decreases lung volume by one half. If an individual takes a breath from a SCUBA tank, then surfaces without venting (exhaling), pressure in the lungs, with minimal ability to further expand, increases to twice normal, which probably causes rupture. The greatest change occurs in the top 33 ft when surfacing.



