Background
Labyrinthitis is an inflammatory disorder of the inner ear, or labyrinth. Clinically, this condition produces disturbances of balance and hearing to varying degrees and may affect one or both ears. Bacteria or viruses can cause acute inflammation of the labyrinth in conjunction with either local or systemic infections. Autoimmune processes may also cause labyrinthitis. Vascular ischemia may result in acute labyrinthine dysfunction that mimics labyrinthitis. (See Etiology and Presentation.)
Etiology
The anatomic relationships of the labyrinth, middle ear, mastoid, and subarachnoid space are essential to understanding the pathophysiology of labyrinthitis. The labyrinth is composed of an outer osseous framework surrounding a delicate, membranous network that contains the peripheral sensory organs for balance and hearing. (See the image below.)
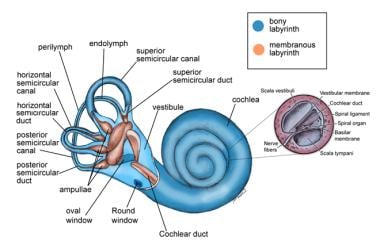 Anatomy of the labyrinth.
Anatomy of the labyrinth.
These sensory organs include the utricle, saccule, semicircular canals, and cochlea. Symptoms of labyrinthitis occur when infectious microorganisms or inflammatory mediators invade the membranous labyrinth and damage the vestibular and auditory end organs.
The labyrinth lies within the petrous portion of the temporal bone adjacent to the mastoid cavity and connects with the middle ear at the oval and round windows. The labyrinth maintains connections with the central nervous system (CNS) and subarachnoid space by way of the internal auditory canal and cochlear aqueduct. Bacteria may gain access to the membranous labyrinth by these pathways or through congenital or acquired defects of the bony labyrinth. Viruses may spread to labyrinthine structures hematogenously or by way of the aforementioned preformed pathways.
Viral and bacterial labyrinthitis are sufficiently different to warrant discussing them as separate disease processes.
Viral labyrinthitis
Viral infections can cause congenital and acquired hearing loss. Rubella and cytomegalovirus are the best-recognized viral causes of prenatal hearing loss. Virally induced hearing loss in the postnatal period is usually due to mumps or measles. Viral infections are also implicated in idiopathic, sudden sensorineural hearing loss (SNHL). Experimental evidence suggests that inflammatory proteins play a critical role in the pathogenesis of cytomegalovirus-induced hearing loss. [1]
A unique form of viral labyrinthitis is herpes zoster oticus, or Ramsay-Hunt syndrome. The cause of this disorder is reactivation of a latent varicella-zoster virus infection occurring years after the primary infection. Evidence suggests that the virus may attack the spiral and vestibular ganglion in addition to the cochlear and vestibular nerves. [2] Auditory and vestibular symptoms develop in approximately 25% of patients with herpes oticus, in addition to the facial paralysis and vesicular rash that characterize the disease. [3]
Bacterial labyrinthitis
Bacterial labyrinthitis is a potential consequence of meningitis or otitis media and may occur by either direct bacterial invasion (suppurative labyrinthitis) or through the passage of bacterial toxins and other inflammatory mediators into the inner ear (serous labyrinthitis). Labyrinthitis is the most common complication of otitis media, accounting for 32% of all intracranial and extracranial complications in one study. [4]
Although bacterial labyrinthitis is rare in the postantibiotic era, bacterial meningitis remains a significant cause of hearing loss. [5] Auditory symptoms, vestibular symptoms, or both may be present in as many as 20% of children with meningitis. [6] Meningitis typically affects both ears, whereas otogenic infections typically cause unilateral symptoms.
Suppurative labyrinthitis
In patients with meningitis, bacteria can spread from the cerebrospinal fluid to the membranous labyrinth by way of the internal auditory canal or cochlear aqueduct. Bacterial infections of the middle ear or mastoid most commonly spread to the labyrinth through a dehiscent horizontal semicircular canal. [7] Usually, the dehiscence is the result of erosion by a cholesteatoma. Suppurative labyrinthitis resulting from otitis media is uncommon in the postantibiotic era. When suppurative labyrinthitis occurs, it is almost always associated with cholesteatoma. Profound hearing loss, severe vertigo, ataxia, and nausea and vomiting are common symptoms of bacterial labyrinthitis.
Labyrinthitis ossificans, the deposition of bone in the fluid-filled spaces of the inner ear, often follows suppurative labyrinthitis; therefore, decisions regarding cochlear implantation must be made early. Meningitis may also result in progressive hearing loss secondary to necrosis and fibrosis of the membranous cochlea and labyrinth. [8]
Serous labyrinthitis
Serous labyrinthitis occurs when bacterial toxins and host inflammatory mediators, such as cytokines, enzymes, and complement, cross the round window membrane, causing inflammation of the labyrinth in the absence of direct bacterial contamination. [9] This condition is associated with acute or chronic middle ear disease and is believed to be one of the most common complications of otitis media.
Toxins, enzymes, and other inflammatory products infiltrate the scala tympani, forming a fine precipitate just medial to the round window membrane. Penetration of the inflammatory agents into the endolymph at the basilar turn of the cochlea results in a mild to moderate, high-frequency SNHL.
Audiometric testing reveals a mixed hearing loss when a middle ear effusion is present. Vestibular symptoms may occur but are less common. Treatment is aimed at eliminating the underlying infection and clearing the middle ear space of effusion. The hearing loss is usually transient but may persist if the otitis is left untreated.
Causative viruses and bacteria
Little direct evidence suggests a viral cause for labyrinthitis; however, a wealth of epidemiologic evidence implicates a number of viruses as potentially causing inflammation of the labyrinth. Viral labyrinthitis is often preceded by an upper respiratory tract infection and occurs in epidemics. The histologic finding of axonal degeneration in the vestibular nerve suggests a viral etiology for vestibular neuritis. [10]
The bacteria that cause labyrinthitis are the same bacteria responsible for meningitis and otitis. Gram-negative organisms are found more commonly when cholesteatoma is the inciting factor.
Potential viral causes of labyrinthitis include the following:
-
Cytomegalovirus
-
Mumps virus
-
Varicella-zoster virus
-
Rubeola virus
-
Influenza virus
-
Parainfluenza virus
-
Rubella virus
-
Herpes simplex virus 1
-
Adenovirus
-
Coxsackievirus
-
Respiratory syncytial virus
Potential bacterial causes of labyrinthitis include the following:
-
Streptococcus pneumoniae
-
Haemophilus influenzae
-
Moraxella catarrhalis
-
Neisseria meningitidis
-
Streptococcus species
-
Staphylococcus species
-
Proteus species
-
Bacteroides species
-
Escherichia coli
-
Mycobacterium tuberculosis
Autoimmune labyrinthitis
Autoimmune labyrinthitis is an uncommon cause of sensorineural hearing loss and may occur as a local, inner ear process or as part of a systemic autoimmune disease such as Wegener granulomatosis or polyarteritis nodosa. [11, 12]
Epidemiology
Occurrence in the United States
Although definitive epidemiologic data are lacking, viral labyrinthitis is the most common form of labyrinthitis observed in clinical practice. The prevalence of sudden SNHL is estimated at 1 case in 10,000 persons, with up to 40% of these patients complaining of vertigo or dysequilibrium. [13] One study reported that 37 of 240 patients presenting with positional vertigo had viral labyrinthitis. [14]
Age-related demographics
Viral labyrinthitis is usually observed in adults aged 30-60 years and is rarely observed in children. Meningogenic suppurative labyrinthitis is usually observed in children younger than 2 years, which is the population most at risk for meningitis. Otogenic suppurative labyrinthitis can be observed in persons of any age in the presence of cholesteatoma or as a complication of untreated acute otitis media. [9] Serous labyrinthitis is more common in the pediatric age group, in which the vast majority of acute and chronic otitis media cases are observed.
Prognosis
The acute symptoms of vertigo and nausea and vomiting resolve after several days to weeks in all forms of labyrinthitis; however, hearing loss is more variable.
Suppurative labyrinthitis nearly always results in permanent and profound hearing loss, whereas patients with viral labyrinthitis may recover from hearing loss. Dysequilibrium and/or positional vertigo also may be present for weeks following resolution of the acute infection.
Morbidity and mortality
Deaths associated with labyrinthitis are not reported except in cases of meningitis or overwhelming sepsis. The morbidity of labyrinthitis, especially bacterial labyrinthitis, is significant.
Bacterial labyrinthitis, regardless of etiology, accounts for one third of all cases of acquired hearing loss.
In the pediatric population, the risk of hearing loss secondary to meningitis is estimated to be 10-20%. [6, 15] Permanent hearing loss occurs in 10-20% of children with meningitis. [6, 15] One study reported dizziness following pneumococcal meningitis in 23% of patients. [16]
Permanent SNHL occurs in approximately 6% of patients with herpes zoster oticus who present with hearing loss. [7] S pneumoniae appears to be the agent most likely associated with meningitis-associated hearing loss. [17]
Ménière disease may follow an episode of suppurative or serous labyrinthitis and is most likely due to fibrosis of the endolymphatic sac and altered Na+/K+ transport.
Patient Education
Counsel patients regarding the potential for injury to themselves or others if they operate heavy machinery or drive a vehicle while vertiginous or while taking certain medications to control symptoms. (See Treatment and Medication.)
For patient education information, see the Ear, Nose and Throat Center, as well as Labyrinthitis and Vertigo.
-
Anatomy of the labyrinth.





