Practice Essentials
Acute adrenal crisis is a potentially fatal condition resulting from a lack of the adrenal gland hormone cortisol. Adrenal crisis and severe acute adrenocortical insufficiency are often elusive diagnoses that may result in severe morbidity and mortality when undiagnosed or ineffectively treated. [1, 2, 3]
Although it is thought by experts that more than 50 steroids are produced within the adrenal cortex, [4] cortisol and aldosterone are by far the most abundant and physiologically active. Regulation of the adrenal cortex is illustrated in the image below.
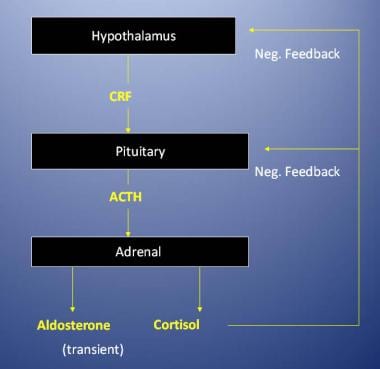 Regulation of the adrenal cortex.
Regulation of the adrenal cortex.
In primary adrenocortical insufficiency, glucocorticoid and mineralocorticoid properties are lost; however, in secondary adrenocortical insufficiency (ie, secondary to disease or suppression of the hypothalamic-pituitary axis), mineralocorticoid function is preserved.
Although suppression of the hypothalamic-pituitary axis from chronic exogenous steroid use is the most common cause of secondary adrenal insufficiency, the possibility of hypopituitarism due to hypothalamic-pituitary disease must be considered. With acute hypopituitarism, other hormone deficiencies must be identified and treated in addition to treating adrenal insufficiency with corticosteroids. For instance, if a patient with panhypopituitarism due to Sheehan syndrome (postpartum pituitary infarction) is only treated for adrenal crisis, severe cardiovascular compromise from the untreated associated hypothyroidism likely occurs. Death can result if the hypothyroid state is not diagnosed.
Every emergency physician should be familiar with adrenocortical insufficiency, which is a potentially life-threatening entity. The initial diagnosis and decision to treat are presumptive and are based on history, physical examination, and, occasionally, laboratory findings. Delay in treatment while attempting to confirm this diagnosis can result in poor patient outcomes.
Signs and symptoms of adrenal crisis
The following are important elements in the history of patients with adrenal crisis or adrenal insufficiency [5, 6] :
-
Weakness (99%)
-
Pigmentation of skin (98%)
-
Weight loss (97%)
-
Abdominal pain (34%)
-
Salt craving (22%)
-
Diarrhea (20%)
-
Constipation (19%)
-
Syncope (16%)
-
Vitiligo (9%)
Workup in adrenal crisis
The following should be assessed in patients with suspected adrenal crisis or adrenal insufficiency:
-
Complete blood count (CBC)
-
Electrolyte levels
-
Blood urea nitrogen (BUN) level
-
Creatinine level
-
Cortisol level [7] /adrenocorticotropic hormone (ACTH)
-
Serum calcium level
-
Thyroid function - Possibly performed in the emergency department [ED] but unlikely to influence immediate management
A computed tomography (CT) scan of the abdomen may show hemorrhage in the adrenals, calcification of the adrenals (seen with tuberculosis), or metastasis.
Management of adrenal crisis
Emergency department care includes the following:
-
Maintain airway, breathing, and circulation in patients with adrenal crisis
-
Use coma protocol (ie, glucose, thiamine, naloxone)
-
Use aggressive volume replacement therapy (dextrose 5% in normal saline solution [D5NS])
-
Correct electrolyte abnormalities
-
Use dextrose 50% as needed for hypoglycemia
-
Administer hydrocortisone 100 mg intravenously (IV) every 6 hours; during ACTH stimulation testing, dexamethasone (4 mg IV) can be used instead of hydrocortisone to avoid interference with testing of cortisol levels
-
Administer fludrocortisone acetate (mineralocorticoid) 0.1 mg every day as needed; mineralocorticoid administration is usually not necessary for treatment of secondary adrenocortical insufficiency
-
Once the patient stabilizes, usually by the second day, the corticosteroid dose may be reduced and then tapered; oral maintenance can usually be achieved by the fourth or fifth day
-
Always treat the underlying problem that precipitated the crisis; infectious etiologies commonly precipitate adrenal crisis
Pathophysiology
Adrenal medullae normally secrete 80% epinephrine and 20% norepinephrine. Sympathetic stimulation results in secretion.
The adrenal cortex produces cortisol, aldosterone, and androgens. Cortisol is produced from 2 hydroxylations of 17alpha-hydroxyprogesterone. Cortisol, also known as hydrocortisone, is 90-93% protein bound (primarily by corticosteroid-binding globulin).
Physiologic effects of glucocorticoids
Glucocorticoids are nonspecific cardiac stimulants that activate release of vasoactive substances. In the absence of corticosteroids, stress results in hypotension, shock, and death. Glucocorticoids act as follows to:
-
Stimulate gluconeogenesis and decrease cellular glucose use
-
Mobilize amino acids and fatty acids
-
Inhibit the effects of insulin
-
Give rise to ketone bodies in metabolism (ketogenesis)
-
Elevate RBC and platelet levels
-
Exhibit anti-inflammatory effects, including the following:
Maintenance of normal vascular response to vasoconstrictors
Opposition to increases in capillary permeability
Inhibition of interleukin-2 (IL-2) production by macrophages
Stimulation of polymorphonuclear neutrophil (PMN) leukocytosis
Reduction of adherence of macrophages to endothelium
Depletion of circulating eosinophils and lymphocytes
Reduction of circulating lymphocytes (primarily T cells)
Physiologic effects of aldosterone
Aldosterone is produced by multiple hydroxylations of deoxycorticosterone and is normally 60% protein bound. The renin-angiotensin system stimulates aldosterone release. Increased potassium stimulates aldosterone production, and decreased potassium inhibits production. Chronic adrenocorticotropic hormone (ACTH) deficiency may inhibit production.
The primary actions of aldosterone cause the kidneys, gut, and salivary/sweat glands to affect electrolyte balance. The primary targets are the kidneys; where it stimulates reabsorption of sodium and secretion of potassium and hydrogen ions. The kidneys' effect on sodium and potassium depend on the intake of these cations (ie, increased sodium intake = increased potassium secretion). The effects on hydrogen probably can occur independently.
Persistent aldosterone excess results in atrial natriuretic factor release and renal hemodynamic changes for compensation. Congestive heart failure (CHF) and cirrhosis with ascites are exceptions that cause progressive sodium retention. Excess aldosterone results in sodium retention, hypokalemia, and alkalosis. Aldosterone deficiency results in sodium loss, hyperkalemia, and acidosis. Hyperkalemia stimulates aldosterone release to improve potassium excretion. Aldosterone is the first-line defense against hyperkalemia.
Primary adrenal insufficiency
Primary adrenal insufficiency, which can be acute or chronic, may be caused by the anatomic destruction of the gland. This destruction can have various causes, including tuberculosis or fungal infection, other diseases infiltrating the adrenal glands, and hemorrhage. However, the most frequent cause is idiopathic atrophy, which is probably autoimmune in origin.
Primary adrenal insufficiency also may be caused by metabolic failure (eg, insufficient hormone production). This failure may be a result of congenital adrenal hyperplasia (CAH), enzyme inhibitors (eg, metyrapone), or cytotoxic agents (eg, mitotane).
Primary adrenocortical insufficiency is rare and occurs at any age. The male-to-female ratio is 1:1.
A retrospective study by Rushworth et al indicated that in pediatric patients with CAH, adrenal crises occur mostly in younger children. The study, which evaluated 573 admissions for medical problems in youngsters with CAH, found that 21 of 37 adrenal crises occurred in patients aged 1-5 years, with another six in children aged up to 1 year. [8]
A Japanese study reported that in children under age 7 years with 21-hydroxylase deficiency, a cause of CAH, the incidence of adrenal crisis was 10.9 cases per 100 person-years. [9]
Secondary adrenal insufficiency
Secondary adrenal insufficiency may be caused by hypopituitarism due to hypothalamic-pituitary disease or may result from suppression of the hypothalamic-pituitary axis by exogenous steroids or endogenous steroids (ie, tumor).
Secondary adrenocortical insufficiency is relatively common. Extensive therapeutic use of steroids has greatly contributed to increased incidence.
Acute adrenocortical insufficiency
Adrenal crisis may result from an acute exacerbation of chronic insufficiency, [10] usually caused by sepsis or surgical stress. Acute adrenal insufficiency also can be caused by adrenal hemorrhage (eg, usually septicemia-induced Waterhouse-Friderichsen syndrome [fulminant meningococcemia]) and anticoagulation complications. Steroid withdrawal is the most common cause of acute adrenocortical insufficiency and almost exclusively causes a glucocorticoid deficiency.
Epidemiology
Frequency
United States
Primary adrenocortical insufficiency is an uncommon disorder with an incidence in Western populations near 50 cases per 1,000,000 persons. With the advent of widespread corticosteroid use, however, secondary adrenocortical insufficiency due to steroid withdrawal is much more common. Approximately 6,000,000 persons in the United States are considered to have undiagnosed adrenal insufficiency, which is clinically significant only during times of physiologic stress.
Primary adrenocortical insufficiency has multiple etiologies; however, 80% of cases in the United States are caused by autoimmune adrenal destruction. Glandular infiltration by tuberculosis is the second most frequent etiology.
In patients with primary adrenocortical insufficiency due to idiopathic autoimmune lymphocytic infiltration, the presence of other associated endocrine disorders must be entertained. Consider polyglandular autoimmune disorders (PGAs) such as Schmidt syndrome.
Schmidt syndrome (PGA type II) includes adrenal insufficiency, autoimmune thyroid disease, and, occasionally, insulin-dependent diabetes mellitus. Adrenal insufficiency usually occurs in these patients when they are older than 20 years. In approximately 40-50% of patients with PGA II, the first manifestation of the syndrome is adrenal insufficiency.
PGA type I includes hypoparathyroidism and mucocutaneous candidiasis in conjunction with adrenal insufficiency. The full triad may manifest in approximately 30% of patients with PGA type I.
International
In a study from the Netherlands, Smans et al found evidence that in primary and secondary adrenal insufficiency, the incidence rate of adrenal crisis per 100 person-years is 5.2 and 3.6, respectively. [11]
A study by Notter et al found that among Swiss patients with primary or secondary adrenal insufficiency, 4.4 adrenal crises per 100 disease-years occurred. [12]
Mortality/Morbidity
Acute adrenocortical insufficiency is a difficult diagnosis to make. The disorder rarely occurs without concomitant injury or illness. Many of the presenting signs and symptoms are nonspecific. For instance, a postoperative fever may presumptively be treated as infection or systemic inflammatory response syndrome when it may be a subtle indicator of adrenal insufficiency.
Left untreated, a patient with acute adrenal insufficiency has a dismal prognosis for survival. Therefore, treatment upon clinical suspicion is mandatory. Any delay in management while waiting for diagnostic confirmation cannot be justified. [13]
A Japanese study, by Ono et al, indicated that among patients with adrenal crisis, the risk of death is relatively high in those who are older and have impaired consciousness and diabetes mellitus. In the study, of 799 patients with adrenal crisis and concomitant primary or secondary adrenal insufficiency at hospital admission, 2.4% (19) suffered in-hospital mortality, including 15 who were older than 60 years, 12 who had impaired consciousness at admission, and 13 who received insulin therapy. [14]
Sex
Although primary adrenocortical insufficiency affects men and women equally, women are affected 2-3 times more often by the idiopathic autoimmune form of adrenal insufficiency.
Age
In idiopathic autoimmune adrenal insufficiency, the diagnosis is most often discovered in the third to fifth decades of life; however, it is particularly important to recognize that adrenocortical insufficiency is not limited to any specific age group.
-
Regulation of the adrenal cortex.


