Practice Essentials
Actinic prurigo is a photodermatosis that involves the skin, lips, and conjunctival mucosa mainly found in native and admixed populations of Latin America. In 1954, Escalona first described it in Mexico. [1] Lesions appear hours or days following sun exposure, contrary to what happens in solar urticaria, in which skin lesions appear minutes after ultraviolet (UV) exposure. Note that lesions may also appear on areas not typically subjected to sun exposure, such as the buttocks. [2] Actinic prurigo is commonly associated with cheilitis and conjunctivitis. [3, 4] Usually, it is diagnosed during childhood following extended solar exposure. It has a chronic course where pruriginous papules, nodules, and excoriated plaques on photoexposed skin areas are clearly evident. This morphology usually is accompanied by ocular pseudopterygium and cheilitis.
There is a lack of knowledge regarding its pathophysiology, but current histological and research findings suggest that it is an ongoing type IV hypersensitivity reaction with still unknown other immunopathogenic processes. They include the involvement of HLA-DR4 genes and the infiltration of CD4 lymphocytes, eosinophils, mast cells, and a serum increase of immunoglobulin E (IgE).
The prognosis is poor, with frequent relapses, especially during spring and summer. Actinic prurigo does not improve with time, contrary to what occurs in polymorphous light eruption (PLE).
Clinical manifestations are usually sufficient to diagnose this condition; however, phototesting can help diagnose undetermined or less severe cases. Although the presence of lymphoid follicles in the mucosa is not a frequent finding, its presence highly suggests a diagnosis of actinic prurigo.
Treatment includes intensive photoprotection, anti-inflammatories, and immunomodulators.
Patients affected by conjunctivitis or pseudopterygium should be evaluated by an ophthalmologist.
Patients affected by actinic prurigo should not have restrictions in any areas, such as employment and education. However, changing from outdoor to indoor occupations is important if the patient is not improving with treatment.
See the images below.
 Itchy plaques mainly on photoexposed areas of the face; these plaques are characteristic of actinic prurigo.
Itchy plaques mainly on photoexposed areas of the face; these plaques are characteristic of actinic prurigo.
 About 75% of patients have cheilitis, which can take the form of solid lesions or erosions.
About 75% of patients have cheilitis, which can take the form of solid lesions or erosions.
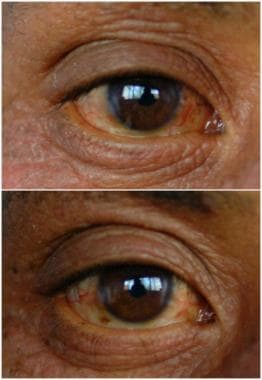 One half of patients have bilateral conjunctivitis. Eye protection is needed to avoid disease progression.
One half of patients have bilateral conjunctivitis. Eye protection is needed to avoid disease progression.
Pathophysiology
No systemic or local photosensitizer is known in patients with actinic prurigo, and a hypersensitivity-implicating immunoglobulin E (IgE) has not been demonstrated.
Actinic prurigo has many features of a type IV hypersensitivity reaction. Skin lesions associated with actinic prurigo are infiltrated with T lymphocytes, mostly CD4+, and some of the T-cells express activation markers. [5] Actinic prurigo falls in the category of autoimmune diseases because lymphocytes from patients have been proven to be stimulated in a thymidine incorporation assay when confronted with their own UV-irradiated keratinocytes or UV-irradiated epidermal homogenates. [6]
At this point, the antigen that provokes the inflammatory reaction is not clear, but an epidermal protein is believed to be transformed by UV exposure. In the series by Santos-Martinez et al, [7] the presence of transforming growth factor-beta interleukin 13 and interleukin 10 was demonstrated in a non–type-TH1, non–type-TH2 pattern, similar to what has been shown in lesions of psoriasis and in the synovial fluid of rheumatoid arthritis.
Another potentially important finding in the pathogenesis of actinic prurigo may be the fact that Langerhans cells in persons with actinic prurigo show resistance to UV exposure when compared with those in healthy individuals. [8, 9] This same finding has been shown in patients with a similar disease, polymorphous light eruption (PLE). Because these cells are resistant to their demise after UV exposure, they might handle and deliver UV-modified cutaneous antigens to T cells in larger amounts or in a more persistent way. This process could cause or augment the inflammatory phenomenon that is observed in the skin of patients with actinic prurigo. The apoptotic mechanism in these cells may be somewhat altered, facilitating their survival.
On the other hand, the polyclonal cellular immune response found in biopsy samples from Mexican patients may involve an imbalance linked to a specific hyperimmunity, in which the proportion of autoimmune cells is increased and the proportion of other cells is decreased. [10] This response is characterized by infiltration of CD4 lymphocytes, eosinophils, mast cells, and a serum increase of IgE. [11, 12]
Although different series are searching for a specific HLA, studies have shown associations with B40 and CW3 alleles in some populations, especially Amerindians. [13, 14] For instance, in the Chimila Indians from Colombia, [15] a high frequency of HLA-Cw4 was found. However, in Cree Indians from Saskatchewan, Canada, [16] the most common antigens were HLA-A24 and HLA-Cw4.
Other studies have shown a strong association with HLA-DR4. The more precise finding appears to be in the Mexican series, in which HLA-DR4 DRB1*0407 is found in more than 90% of patients with actinic prurigo. [17] Another series also found HLA-DR4 DRB1*0407 in Colombian patients. [18] Related alleles such as DRB*0407 have been found in British populations, [19] and DRB1*14 has been found in the Inuit Indians of Canada. [13]
Additional to the role of HLA-DR4 DRB1*0407 in the genetic susceptibility to develop actinic prurigo, HLA-DRB1*1406 could also be involved, and HLA-DRB1*0802 may possibly have a protective role. The existence of an HLA-B39-DRB1*0407 haplotype suggests a susceptibility region within the sixth human chromosome, at least among Amerindians affected by actinic prurigo. [20]
English patients with PLE [21] have not shown an association with any HLA, which suggests that HLA-DR4 (DRB1*0407) could be used as a marker to distinguish PLE from actinic prurigo. Therefore, the association with HLA in actinic prurigo but not in PLE suggests that actinic prurigo represents an immunologically mediated disease with strong genetic determinants for its expression. [15, 17]
Epidemiology
Actinic prurigo occurs in persons of all skin types, but its prevalence in the general population is unknown. It probably represents less than 5% of referrals to photodermatologic clinics. [22] Actinic prurigo is well known in the United States among Native Americans. [14, 15, 22, 23]
In Mexico, actinic prurigo represents 1.34% of consultations with pediatric dermatologists and 4% of consultations with general dermatologists. [1] Actinic prurigo is common in Mexico, Central America, and South America, and it is well known in Canada among Native Americans. [14, 15, 23] Actinic prurigo rarely occurs in Europe and Asia, where PLE (a disease with pathogenetic features similar to actinic prurigo) is more regularly seen. Isolated cases have been reported in France, [24] Germany, [25] Japan, [26] Singapore, [27] Thailand, [28] Norway, [29] and Australia. [30] However, the prevalence rate of actinic prurigo in photodermatology clinics around the world varies from 0-5%. [27]
Actinic prurigo frequently affects admixture populations (eg, mestizos) of Latin America and American Indians with skin phototypes IV or V. In children and adolescents, no differences in prevalence exist between the sexes. However, in adults, women are more frequently affected than men, with a female-to-male ratio of 2:1. [1, 22]
Actinic prurigo can occur at any age; however, one third of patients are children. [1] The impact on quality of life in this population is serious. By means of the children's dermatology life quality index (CDLQI), children with actinic prurigo show high scores and closer to those obtained in children with xeroderma pigmentosum. [31]
Patient Education
Patients should always avoid sun exposure. Daily activities should be performed before 9 am and after 6 pm in tropical areas. In these regions of the world, sunlight can cause lesions to flare even with minor exposures (15 minutes [5 J/cm2UVA]). [32] Therefore, when outdoors, patients must wear dark-colored protective clothing such as pants, long sleeves, high neck, big-brimmed hat, and sunglasses.
Sunscreens should be used with caution, particularly commercial ones composed mainly with chemical filters, as these can worsen irritation on excoriated areas of the exposed skin. Thus, mineral sunscreens are more suitable in these cases. Teaching patients how to apply sunscreen is important. In the early phases of treatment, patients may not apply it properly; they may spread the cream all over their skin without allowing it to fully absorb. Therefore, teach patients to try to reach at least a 2-mg/cm2 dose on the exposed areas. A full UV coverage (290-400 nm) sunscreen is necessary to avoid exacerbations.
The patient should be aware of the UV index. The UV index forecast is usually available on the Internet or through the media in many parts of the world.
Patients should know that actinic prurigo is not a dose-dependent disease, and, similar to all immune-mediated hypersensitivity disorders, a minor amount of the offensive agent may provoke outbreaks.
-
Itchy plaques mainly on photoexposed areas of the face; these plaques are characteristic of actinic prurigo.
-
Photodistribution of lesions over the body. Note the hypopigmented areas of the skin, which are very common after intense scratching in children.
-
Multiple itchy papules coalescing into plaques on the neck. These lesions are similar to lesions of polymorphous light eruption. Note the excoriations induced by scratching.
-
One third of patients are children. The nose is frequently affected. This clinical feature is useful in distinguishing it from other entities, such as atopic dermatitis.
-
One half of patients have bilateral conjunctivitis. Eye protection is needed to avoid disease progression.
-
About 75% of patients have cheilitis, which can take the form of solid lesions or erosions.
-
A phototest with UV-B light shows reproduction of lesions on the inner aspect of the arm. The result from the phototest with UV-A light was negative.
-
Histologic examination shows acanthosis, mild spongiosis, edema of the lamina propria, and a moderate-to-dense perivascular lymphocytic inflammatory infiltrate.
-
A close-up view shows edema of the lamina propria as well as a lymphocytic inflammatory infiltrate in the dermis.
-
Young girl with a history of atopic dermatitis and itchy, lichenified plaques on her face for the last 3 months. Atopic dermatitis with photosensitivity is the main differential diagnosis with actinic prurigo in children.
-
Actinic cheilitis resulting from actinic prurigo.
-
Erythematous and very itchy plaques on solar exposure areas of the face and pseudopterygium are commonly observed in actinic prurigo.
-
Lichenified plaques, excoriated nodules, and atrophic scars on the dorsal aspect of hands are frequently seen in children.
-
Contact dermatitis due to sunscreen in a patient with actinic prurigo.
-
Impetiginous area located on the right ear lobe due to intense scratching following an acute relapse.






