Background
First described in detail by Henri Mondor in 1939, this condition is a rare entity characterized by a sclerosing thrombophlebitis of the subcutaneous veins of the anterior chest wall, as diagrammed in the image below. Fage in 1870 has been credited with delineating cording as a sign of superficial thrombophlebitis.}
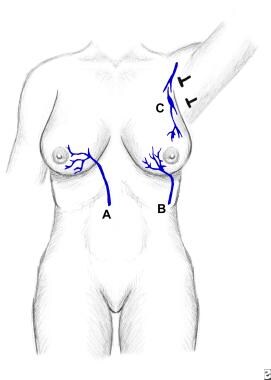 Illustration of the venous channels involved in Mondor disease. A is superior epigastric vein. B is thoracoepigastric vein. C is lateral thoracic vein.
Illustration of the venous channels involved in Mondor disease. A is superior epigastric vein. B is thoracoepigastric vein. C is lateral thoracic vein.
The sudden appearance of a subcutaneous cord, which is initially red and tender and subsequently becomes a painless, tough, fibrous band that is accompanied by tension and skin retraction, is characteristic. The condition, though benign and self-limited, has been associated with breast cancer. It requires only symptomatic therapy. However, the physician must be aware of its existence to properly diagnose it and to rule out the presence of systemic disorders, especially breast cancer. [1]
Subcutaneous penile vein thrombosis (penile Mondor disease) has also been described. [2, 3] Its pathogenesis is unknown. It appears suddenly as almost painless indurations on the penile dorsal surface. Rarely, it may be evident as induration on the ventral penile aspect. [4] Similar cording may rarely occur in the groin, abdomen, arm, and axilla. [5] In the latter site, it has been termed the axillary web syndrome and may be evident after axillary lymph node dissection and sentinel lymph node biopsy.
A related article is Superficial Thrombophlebitis.
Pathophysiology
The pathophysiology has been explained as pressure on the vein with stagnation of blood or as direct trauma to the vein itself. In cases that do not show such evidence, the most reasonable explanation is on the basis of repeated movement of the breast along with the contracting and relaxing pectoral muscles, which causes stretching and relaxing of the veins. [6] . An tight bra may be implicated by causing direct trauma. [7] Bodybuilders using intense thoracoabdominal exercise training may also develop it. [8]
Mondor disease may only involve one or more of three venous channels: the thoracoepigastric vein, the lateral thoracic vein, and the superior epigastric vein. The upper, inner portions of the breast are never involved. Mondor disease can also occur on the penis, groin, antecubital fossa, and posterior cervical region. [9, 10] It may involve the thoracoepigastic, lateral thoracic, or the superior epigastric vein. [11]
Although most often linked with breast cancer surgery and anesthetic mammaplasties, [12] it may also occur as a result of excision of axillary nodes after gel silicone breast implant rupture. [13] It may also be a complication of ultrasound-guided core needle biopsy. [14] Trauma from breast augmentation was described as a predisposing factor. [15] Hypersensitivity reactions may also predispose, with penile Mondor disease rarely linked with scabies [16] and with excessive masturbation. [17]
Epidemiology
Frequency
Fewer than 400 cases have been described worldwide. [18] However, its incidence after breast cancer surgery and aesthetic mammaplasties has been estimated at 1%. [13]
Race
No racial or ethnic predilection is evident.
Sex
Mondor disease is 3 times more common in women than in men. [19]
Age
The disease can occur in persons of any age, but most patients are aged 30-60 years. [19]
Prognosis
Mondor disease has proven to be self-limited and benign. Its significance lies in the clinician's recognition and differentiation of it from primary, recurrent, or metastatic carcinoma, or an abscess of the breast. As are other forms of migratory thrombophlebitis, Mondor disease may be an indication of an occult carcinoma elsewhere in the body. Patients with this condition should continue to be observed.
Patient Education
Explaining to the patient that no instance of Mondor disease has reportedly preceded or eventuated in breast cancer may be beneficial. However, patients with a history of Mondor disease should have periodic breast examinations, mammography, and additional tests searching for cancer elsewhere.
For patient education resources, see the Cancer Center, as well as Phlebitis, Breast Cancer, and Breast Self-Exam.
-
Illustration of the venous channels involved in Mondor disease. A is superior epigastric vein. B is thoracoepigastric vein. C is lateral thoracic vein.






