Historical Aspects of Biological Warfare Agents
Biological weapons include any organism or toxin found in nature that can be used to incapacitate, kill, or otherwise impede an adversary. Biological weapons are often characterized by low visibility, high potency, substantial accessibility, and relatively easy delivery.
The potential spectrum of bioterrorism ranges from hoaxes and actual use of agents by individuals or groups against others, to state-sponsored terrorism that employs biological warfare (BW) agents and delivery systems that can produce mass casualties. Such scenarios would present serious challenges for patient treatment and for prophylaxis of exposed persons. Environmental contamination could also pose continuing threats.
The use of biological agents is not a new concept, and history is replete with examples of biological weapons use. Before the 20th century, biological warfare took three main forms: (1) deliberate poisoning of food and water with infectious or toxic material, (2) use of microorganisms or toxins in some form of weapon system, and (3) use of biologically inoculated fabrics.
Attempts to use biological weapons date back to antiquity. As far back as 400 BC, Scythian archers infected their arrows by dipping them in decomposing bodies or in blood mixed with manure. Persian, Greek, and Roman literature from 300 BC quotes examples of the use of animal cadavers to contaminate wells and other sources of water. In 190 BC, at the Battle of Eurymedon, Hannibal won a naval victory over King Eumenes II of Pergamon by firing earthen vessels full of venomous snakes onto the enemy ships. [1]
In the 12th century AD, during the battle of Tortona, Barbarossa used the bodies of dead soldiers to poison wells. In the 14th century AD, during the siege of Kaffa (now Feodosia, Ukraine) the attacking Mongol force hurled the corpses of those who died of plague into the city to attempt to inflict a plague epidemic upon the enemy. This was repeated in 1422 during the Hussite wars in Bohemia at the seige of Karlstejn (now in the Czech Republic) when invading forces hurled plague-striken corpses, dead cows, and 2000 cartloads of excrement at enemy troops. [2]
In the 18th century AD, during the French and Indian War, British forces in North America gave blankets from smallpox patients to the Native Americans to transmit the disease to the immunologically naïve tribes. In 1863, a Confederate surgeon (Dr. Luke Blackburn, who later became governor of Kentucky) was arrested and charged with attempting to import smallpox and yellow fever–infected clothes into the northern United States during the Civil War, to be sold to Union troops. [2]
Biological warfare became more sophisticated against both animals and humans during the 20th century. During World War I, the Germans developed anthrax, glanders, cholera, and a wheat fungus for use as biological weapons. They allegedly spread plague in St. Petersburg, infected mules with glanders in Mesopotamia, and attempted to do the same with the horses of the French cavalry. The German-American physician Anton Dilger established a secret biological laboratory in Chevy Chase, Maryland, with the intent to grow the causative agents of anthrax and glanders. [3] These cultures were spread among horses being shipped to England from Baltimore, New York City, Newport News and Norfolk. [4]
In 1925, the Geneva Protocol was signed by 108 nations, including the five nations that would become the permanent members of the United Nations Security Council. This was the first multilateral agreement that extended prohibition of chemical agents to biological agents. No method for verification of compliance was addressed. [5]
During World War II, the Japanese operated a secret biological warfare research facility in Manchuria and carried out human experiments on Chinese prisoners. They exposed more than 3000 victims to plague, anthrax, syphilis, and other agents. Victims were observed for development of disease, and autopsies were performed. They also developed a plague biological weapon by breeding fleas fed on plague-infected rats, and releasing millions of fleas in aerial attacks on Chinese cities. [6]
In 1942, the United States formed the War Research Service. Anthrax and botulinum toxin initially were investigated for use as weapons, and sufficient quantities of botulinum toxin and anthrax cattle cakes were stockpiled by June 1944 to allow limited retaliation if the Germans first used biological agents. The British had tested anthrax bombs on Gruinard Island off the northwest coast of Scotland in 1942 and 1943 and then prepared and stockpiled anthrax-laced cattle cakes.
The United States continued research on various offensive biological weapons during the 1950s and 1960s. From 1951-1954, simulants (Bacillus globigii,Serratia marcescens) were released off both coasts of the United States to demonstrate the vulnerability of American cities to biological agent attacks. This vulnerability was tested again in 1966 when the simulant B globigii was released in the New York subway system. A US testing facility at Fort Detrick is shown in the photo below.
 The "eight ball" 1 million liter test sphere at Fort Detrick, Maryland. This aerobiology chamber was used before 1969 when the United States was performing offensive biological warfare research. Animals were tethered within the sphere while aerosolized agents were aerosolized.
The "eight ball" 1 million liter test sphere at Fort Detrick, Maryland. This aerobiology chamber was used before 1969 when the United States was performing offensive biological warfare research. Animals were tethered within the sphere while aerosolized agents were aerosolized.
In 1957, the British government decided to end its offensive biological warfare capabilities and destroy its weapon stockpiles.
The United States terminated its offensive biological weapons program in 1969 for microorganisms and in 1970 for toxins. The United States is a signatory nation of the Biological Toxin Weapons Convention of 1972. This convention addressed the prohibition of the development, production, stockpiling, and destruction of bacteriologic and toxin weapons. Signatories to this agreement are required to submit information annually to the United Nations concerning facilities where biological defense research is being conducted, scientific conferences that are held at specified facilities, exchanges of scientists or information, and disease outbreaks. American stockpiles of biological weapons were destroyed completely by 1973.
The Soviet Union (USSR) continued to develop biological weapons from the 1950's onward. In the 1970s, the USSR and its allies were suspected of having used "yellow rain" (trichothecene mycotoxins) during campaigns in Loas, Cambodia, and Afghanistan. In 1979, an accidental release of anthrax from a weapons facility in Sverdlovsk, USSR, killed at least 66 people. [7] The Russians denied this accident until 1992.
Since at least the 1980s, terrorist organizations have been users of biological agents. The most frequent bioterrorism episodes have involved contamination of food and water. In September and October of 1984, 751 persons were infected with Salmonella typhimurium after an intentional contamination of restaurant salad bars in Oregon by followers of the Bhagwan Shree Rajneesh. [8]
In 1985, Iraq began an offensive biological weapons program producing anthrax, botulinum toxin, and aflatoxin. During Operation Desert Shield, the coalition of allied forces faced the threat of chemical and biological agents. Following the Persian Gulf War, Iraq disclosed that it had bombs, Scud missiles, 122-mm rockets, and artillery shells armed with botulinum toxin, anthrax, and aflatoxin. They also had spray tanks fitted to aircraft that could distribute 2000 L over a target. [9]
More recent incidents indicate the need for enhanced buiosecurity. In 1992, 20 people were administered chemoprophylaxis after a Virginia man sprayed his roommates with a substance that he claimed was anthrax. In 1994, a Japanese sect of the Aum Shinrikyo cult attempted an aerosolized release of anthrax from the tops of buildings in Tokyo. In 1995, two members of a Minnesota militia group were convicted of possession of ricin, which they had produced themselves for use in retaliation against local government officials. In 1996, an Ohio man was able to obtain bubonic plague cultures through the mail. [10]
In 1997, the Defense Against Weapons of Mass Destruction Act directed the Department of Defense to establish a domestic preparedness program to improve the ability of local, state, and federal agencies to respond to biological incidents. During 1998 and 1999, multiple hoaxes occurred involving the threatened release of anthrax in the United States that resulted in decontamination and antibiotic prophylaxis for the intended victims. Nearly 6000 persons across the United States have been affected by these threats. According to a study by the Centers for Disease Control and Prevention (CDC), an intentional release of anthrax by a bioterrorist in a major US city would result in an economic impact of $477.8 million to $26.2 billion per 100,000 persons exposed. [11]
From September to November 2001, a total of 23 confirmed or suspected cases of bioterrorism-related anthrax (10 inhalation, 13 cutaneous) occurred in the United States. Most cases involved postal workers in New Jersey and Washington DC, and the rest occurred at media companies in New York and Florida, where letters contaminated with anthrax were handled or opened. As a result of these cases, approximately 32,000 persons with potential exposures underwent antibiotic prophylaxis to prevent anthrax infections. [12]
In 2011, researchers modified H5N1 influenza virus to spread with airborne transmissibility among ferrets. This experiment aroused global concern for the potential of gain of function (GOF) biological research. [13] Various genetic engineering technologies have become increasingly developed over the past decade and may be used for societal good or by those with other intent. These include genome sequencing that enabled publication of full genomes, recombinant DNA technology, reverse genetic manipulation, and clustered regularly interspaced short palindromic repeats (CRISPR) and other gene modification tools, all of which of which could be used for targeting humans, animals, or plants.
In December 2019, the first cases of coronavirus disease 2019 (COVID-19), caused by a novel SARS-CoV-2 virus, were reported in Hubei Province of the People's Republic of China, near Wuhan city and the Wuhan Institute of Virology (WIV), the first Biosafety Level 4 (BSL-4) laboratory in China. [14] The subsequent COVID-19 global pandemic, with over 543 million cases and 6 million deaths could have been caused by either natural zoonotic disease transmission or an inadvertent laboratory release of SARS-CoV-2 at the WIV, and its origin has never been completely resolved. [15]
The threat from biological agent use, whether on military forces or civilian populations, and whether deliberate or accidental, is arguably more likely at present than at any point in all of history. [16, 17]
Delivery, Dissemination, and Detection of Biological Warfare Agents
Biological agents are relatively easy to acquire, synthesize, and use. Because only small amounts of these agents would be capable of killing thousands of people in a metropolitan area, the concealment, transportation, and dissemination of biological agents is relatively easy. In addition, biological warfare (BW) agents are difficult to detect or protect against; they are invisible, odorless, and tasteless, and their dispersal can be performed silently.
Dissemination of BW agents may occur by various methods, including aerosol sprays, explosives (artillery, missiles, detonated bombs), or food or water contamination. Variables that can alter the effectiveness of a delivery system include particle size of the agent, stability of the agent under desiccating conditions, ultraviolet (UV) light exposure, wind speed, wind direction, and atmospheric stability.
The use of an explosive device to deliver and disseminate biological agents is not particularly effective, since such agents tend to be inactivated by the heat of the blast. Contamination of municipal water supplies requires an unrealistically large amount of agent and introduction into the water after it passes through a regional treatment facility.
To be an effective biological weapon, airborne pathogens must be dispersed as fine particles less than 5 μm in size. Infection with an aerosolized agent usually requires deep inspiration of an infectious dose. Advanced weapons systems (eg, warheads, missiles) are not required for the aerosolized delivery of biological agents. Low-technology aerosolization methods would suffice: these include agricultural crop-dusters; aerosol generators on small boats, trucks, or cars; backpack sprayers; and even purse-size perfume atomizers. Consequently, aerosolized dispersal of biological agents is the mode most likely to be used by terrorists and military groups.
Detection of biological agents involves either finding the agent in the environment or medical diagnosis of the agent's effect on human or animal victims. Early detection of a biological agent in the environment allows for early specific treatment and time during which prophylaxis would be effective. [18, 19] Detection systems for BW agents in the 21st century are undergoing changes to incorporate various data inputs. The US Departments of Defense and Homeland Security have placed a high priority on research and development of detector systems. Methods developed include those to detect a biological aerosol cloud using an airborne pulsed laser system to scan the lower altitudes upwind from a possible target area. Priorities include systems that will analyze air samples to provide particle sizes, detect and classify bacterial cells, measure DNA and adenosine triphosphate (ATP) content, and identify agents using immunoassays.
A BW agent attack is likely to be covert. Thus, detection of such an attack requires recognition of the clinical syndromes associated with various BW agents. The nature of bioterrorism threats requires collaboration across several sectors, including intelligence, police, forensics, customs, and other law enforcement organizations, who must work together with public and animal health organizations as well as environmental and social science organizations. [20] Physicians must be able to identify early victims and recognize patterns of disease. This requires integrated disease surveillance systems performing real-time monitoring with information shared at many levels of a health care system (eg, emergency department (ED) to ED, ED to public health officials). Preliminary criteria for suggestive outbreaks of disease that could provide indications of a possible BW event include the following [21] :
-
Disease (or strain) not endemic
-
Unusual antibiotic resistance patterns
-
Atypical clinical presentation or clinical presentation classic for that of a BW agent
-
Case distribution geographically and/or temporally inconsistent (eg, compressed time course)
-
Other inconsistent elements (eg, number of cases, mortality and morbidity rates, deviations from disease occurrence baseline)
Indications of possible BW agent attack include the following [21] :
-
Disease manifestations that are unusual or that do not occur naturally in a given geographic area, or combinations of unusual disease entities in the same patient population
-
Multiple disease entities in the same patients, indicating that mixed agents have been used in the attack
-
Large numbers of both military and civilian casualties when such populations inhabit the same area
-
Data suggesting a massive point-source outbreak
-
Apparent aerosol route of infection
-
High morbidity and mortality rates relative to the number of personnel at risk
-
Illness limited to fairly localized or circumscribed geographic areas
-
Low attack rates in personnel who work in areas with filtered air supplies or closed ventilation systems
-
Sentinel dead animals of multiple species
-
Absence of a competent natural vector in the area of outbreak (for a biological agent that is vector-borne in nature)
Protective Measures
Protective measures can be taken against BW agents. These should be implemented early (if warning is received) or later (once suspicion of BW agent use is made). Currently, available masks such as the military gas mask or high-efficiency particulate air (HEPA) filter masks used for tuberculosis (TB) exposure filter out most BW particles delivered by aerosol. Multilayered HEPA masks can filter 99.9% of 1- to 5-μm particles, but face-seal leaks may reduce the efficacy by as much as 10-20%. Individual face-fit testing is required to correct seal leak problems.
Most aerosolized biological agents do not penetrate unbroken skin, and few organisms adhere to skin or clothing. After an aerosol attack, simple removal of clothing eliminates a great majority of surface contamination. Thorough showering with soap and water removes 99.99% of the few organisms left on the victim's skin after disrobing. The use of sodium hypochlorite is not recommended over soap and water.
The use of special suits by health care providers is not necessary. Normal clothing provides a reasonable degree of protection against dermal exposure. Latex gloves and universal precautions provide sufficient protection when treating most infected patients. Place patients in a private negative-pressure room and practice proper sanitation with universal precautions. Proper disposal of corpses is essential. In the case of anthrax spores; this should be performed by incineration.
Of the classical BW diseases, plague, smallpox, and some viral hemorrhagic fevers are spread readily person to person by aerosol and require more than standard infection control precautions (gown, mask with eye shield, gloves). Regardless, place all potential victims of BW agents in isolation. Medical personnel caring for these patients should wear a HEPA mask in addition to standard precautions pending the results of a more complete evaluation.
Broad-spectrum intravenous antibiotic coverage is recommended initially for victims when a BW agent is suspected. Institute this even prior to the identification of the specific BW agent. Vaccinations currently are available for anthrax, botulinum toxin, tularemia, plague, Q fever, and smallpox. The widespread immunization of nonmilitary personnel has not been recommended by any governmental agency. Immune protection against ricin and staphylococcal toxins may be feasible in the near future. [22]
Bacterial Agents
Anthrax
Bacillus anthracis is a large, aerobic, gram-positive, spore-forming, nonmotile bacillus. The bacterium ordinarily produces a zoonotic disease in domesticated and wild animals such as goats, sheep, cattle, horses, and swine. Humans become infected by contact with infected animals or contaminated animal products. Infection occurs predominantly through the cutaneous route and only rarely via the respiratory or gastrointestinal (GI) route. There is no human-to-human transmission of anthrax.
Anthrax occurs worldwide. The organism exists in the soil as a spore. The "vegetative" form of the organism in infected animals is the bacillus. Sporulation occurs only when the organism in the carcass is exposed to air. Spores remain viable for decades.
The true incidence of human anthrax is unknown. Reporting of illness has been unreliable. In 1958, an estimated 20,000-100,000 cases occurred worldwide. In the United States, the annual incidence of naturally occurring human anthrax has declined steadily from approximately 127 cases in the early years of the 20th century to approximately one per year for the past 20 years.
Pathophysiology
B anthracis possesses three known virulence factors: an antiphagocytic capsule and two protein exotoxins (lethal and edema toxin). The role of the capsule in pathogenesis was demonstrated in the early 1900s when anthrax strains that lack a capsule were demonstrated to be nonvirulent. In more recent years, the genes encoding synthesis of the capsule were found to be encoded on a 110-kilobase plasmid. The capsule is composed of a polymer of poly-D-glutamic acid, which confers resistance to phagocytosis and may contribute to the resistance of anthrax to lysis by serum cationic proteins.
The anthrax toxins, like many bacterial and plant toxins, possess the following two components: a cell-binding B-domain and an active A-domain. The A-domain confers enzymatic activity and toxicity. Edema toxin, which consists of the same protective antigen together with a third protein, edema factor, causes edema when injected into the skin of experimental animals.
Infection begins when the spores are inoculated through skin or mucosa. The estimated infectious dose is 8,000-50,000 spores. It is believed that spores are ingested locally by tissue macrophages. Subsequently, spores germinate within macrophages to the vegetative bacilli, which produce capsules and toxins. Bacteria proliferate at these tissue sites and produce the edema and lethal toxins that impair host leukocyte function and lead to the distinctive and pathologic findings of edema, hemorrhage, tissue necrosis, and a relative lack of leukocytes.
In inhalation anthrax, the spores are ingested by alveolar macrophages, which transport them to the regional tracheobronchial lymph nodes, where germination occurs. In the tracheobronchial lymph nodes, the local production of toxins by extracellular bacilli gives rise to the characteristic pathologic picture of massive hemorrhagic, edematous, and necrotizing lymphadenitis and mediastinitis. The bacillus then can spread to the blood, leading to septicemia and frequently causing hemorrhagic meningitis. Death results from respiratory failure, overwhelming bacteremia, septic shock, and meningitis.
Clinical features of cutaneous anthrax
More than 95% of cases of naturally occuring anthrax are cutaneous. After inoculation, the incubation period is 1-12 days. The disease first appears as a small papule that progresses over 1-2 days to a vesicle containing serosanguineous fluid with many organisms and a paucity of leukocytes. This often has been referred to as a malignant pustule; however, that is a misnomer because no pustular lesions are found in patients with anthrax. The vesicle ruptures, leaving a necrotic ulcer.
The lesion usually is painless, and varying degrees of edema may be present around it. The edema occasionally may be massive, encompassing the entire face or limb, and is described as malignant edema. Patients generally experience fever, malaise, and headache, which may be severe in those with extensive edema. Local lymphadenitis also may be present.
The ulcer base develops a characteristic 1- to 5-cm black eschar. (The black appearance of the eschar gives anthrax its name [Greek anthrakos = coal].) After a period of 2-3 weeks, the eschar separates, often leaving a scar. Septicemia is rare. The mortality rate should be less than 1% with adequate treatment.
Clinical features of inhalation anthrax
Also known as woolsorter's disease, inhalation anthrax has a typical incubation period of 1-6 days, but a latent period as long as 60 days has been described. Initial manifestations are nonspecific and include headache, malaise, fatigue, myalgia, and fever. Associated nonproductive cough and mild chest discomfort may occur. These symptoms usually persist for 2-3 days, and, in some patients, a short period of improvement may occur. This is followed by the sudden onset of increasing respiratory distress with dyspnea, stridor, cyanosis, increased chest pain, and diaphoresis. Associated edema of the chest and neck may be present.
Chest radiographs usually show the characteristic widening of the mediastinum and, often, pleural effusion. Pneumonia is thought to be an uncommon finding. All 10 patients with inhalation anthrax in the United States in September and October 2001 had abnormal chest radiographs on initial presentation; seven had mediastinitis, seven had infiltrates, and eight had pleural effusions. Noncontrast CT scans of the chest may show hyperdense mediastinal adenopathy and diffuse mediastinal edema not evident on plain chest radiographs.
The onset of respiratory distress is followed by the rapid onset of shock and death within 24-36 hours. The mortality rate is 80-90% but may approach 100% when septic shock develops, despite appropriate treatment. In the inhalation anthrax cases that occurred in the United States in 2001, six of the 11 patients survived (65% survival rate).
Inhalation anthrax is the most likely form of disease to follow military or terrorist attack. Such an attack likely will involve the aerosolized delivery of anthrax spores.
Clinical features of oropharyngeal and gastrointestinal anthrax
These forms result from the ingestion of infected meat that has not been cooked sufficiently. After an incubation period of 2-5 days, patients with oropharyngeal disease present with severe sore throat or a local oral or tonsillar ulcer, usually associated with fever, toxicity, and swelling of the neck due to cervical or submandibular lymphadenitis or edema. Dysphagia and respiratory distress also may be present.
GI anthrax begins with nonspecific symptoms of nausea, vomiting, and fever. These symptoms are followed in most patients by severe abdominal pain. The presenting sign may be an acute abdomen, which may be associated with hematemesis, massive ascites, and diarrhea. Mortality rate in both forms may be as high as 50%, especially in the GI form.
Clinical features of anthrax meningitis
This may occur following bacteremia as a complication of any of the other clinical forms. Meningitis also may occur—rarely, without any of the other clinical forms of the disease. It often is hemorrhagic and is almost invariably fatal.
Diagnosis
The most critical aspect in making a diagnosis of anthrax is a high index of suspicion associated with a compatible history of exposure. Consider cutaneous anthrax in patients who develop a painless, pruritic papule, vesicle, or ulcer, often with surrounding edema. The lesion develops into a black eschar. With extensive or massive edema, such a lesion is almost pathognomonic. Gram stain or culture of the lesion confirms the diagnosis. A punch biopsy of the leading margin can be used for immunostaining. The differential diagnosis should include tularemia and staphylococcal or streptococcal infection.
The diagnosis of inhalation anthrax is extremely difficult because no rapid screening tests are available, but suspect the disease with a history of exposure to a B anthracis–containing aerosol. Early symptoms are entirely nonspecific. The development of respiratory distress in association with radiographic evidence of a widened mediastinum due to hemorrhagic mediastinitis and the presence of hemorrhagic pleural effusions or hemorrhagic meningitis should strongly suggest the diagnosis. Sputum Gram stain and culture usually are not helpful because pneumonia is an uncommon feature of illness. Gram stain of peripheral blood should be performed, as it may be positive for gram-positive bacilli, often seen in short and long chains.
GI anthrax also is exceedingly difficult to diagnose because of its rarity and nonspecific symptoms. Diagnosis usually is confirmed only with a history of ingesting contaminated meat in the setting of an outbreak. Once again, cultures generally are not helpful in making the diagnosis.
Meningitis from anthrax is clinically indistinguishable from meningitis due to other etiologies. A suggestive laboratory feature is that the cerebrospinal fluid (CSF) is hemorrhagic in as many as 50% of patients. Identification of the organism in the CSF by microscopy, culture, or both confirms the diagnosis.
Serology can be used to make a retrospective diagnosis. Antibody develops in 68-93% of reported cases of cutaneous anthrax and 67-94% of reported cases of oropharyngeal anthrax. A positive skin test result to anthracin also has been used to make a retrospective diagnosis of anthrax.
The most useful microbiologic test is the standard blood culture, which is almost always positive in patients with systemic illness. Blood cultures should show growth in 6-24 hours. If the laboratory has been alerted to the possibility of anthrax, biochemical testing and review of colony morphology should provide a preliminary diagnosis 12-24 hours later. However, if the laboratory has not been alerted to the possibility of anthrax, B anthracis may not be identified correctly.
Rapid diagnostic tests for B anthracis and its proteins include polymerase chain reaction (PCR), enzyme-linked immunoassay (ELISA), and direct fluorescent antibody (DFA) testing and can be utilized on blood and body fluid specimens. Currently, these tests are utilized throughout the reference labs of the national Laboratory Response Network (LRN). [23]
Treatment
The recommendations provided do not all represent antibiotic uses currently approved by the US Food and Drug Administration (FDA). Rather, they represent a consensus, based on best available information from recent studies.
Anthrax immune globulin (Anthrasil) or the monoclonal antibodies, obiltoxaximab (Anthim) or raxibacumab, may also be considered for inhalational anthrax in combination with appropriate antibiotics. Each of these biologic agents are approved by the FDA for treatment of inhalational anthrax. Additionally, obiltoxaximab and raxibacumab are approved for use as prophylaxis when alternative therapies are not available or not appropriate. [24]
Given the fulminant course of inhalation anthrax, early antibiotic treatment is essential to maximize patient survival. Given the difficulty in achieving timely microbiologic diagnosis of anthrax, all persons with fever or evidence of systemic disease in an area where anthrax cases are occurring should be treated empirically for anthrax until the disease is excluded.
No clinical studies exist of the treatment of inhalation anthrax in humans. Most naturally occurring strains of anthrax are sensitive to penicillin, and penicillin historically has been the preferred therapy for the treatment of anthrax. Penicillin and doxycycline are FDA-approved antibiotics for anthrax. Ciprofloxacin is also FDA approved for the treatment of inhalational anthrax. Doxycycline is the preferred option from the tetracycline class of antibiotics because of its proven efficacy in monkey studies. Other antibiotics to which naturally occurring strains of anthrax are susceptible include the following:
-
Other fluoroquinolones
-
Imipenem
-
Rifampin
-
Macrolides (erythromycin, azithromycin, clarithromycin)
-
First-generation cephalosporins
-
Aminoglycosides.
When anthrax susceptibilities are unknown, begin therapy with ciprofloxacin (400 mg IV bid) or doxycycline (200 mg IV loading dose followed by 100 mg IV bid). To either of these, add one or two other antibiotics effective against anthrax. Antibiotics can be changed over to oral therapy as clinically indicated for a total duration of therapy of at least 60 days.
Traditionally, ciprofloxacin and other fluoroquinolones are not recommended for use in children younger than 16-18 years because of a link to permanent arthropathy in adolescent animals and transient arthropathy in a small number of children. Balancing these small risks against the real risk of death and resistant strains of B anthracis, experts recommend that ciprofloxacin be given to pediatric patients for initial therapy or postexposure prophylaxis following an anthrax attack. In children, ciprofloxacin at 20-30 mg/kg/d IV in 2 daily doses (not to exceed 1 g/d) is recommended.
If antibiotic susceptibility testing allows, substitute intravenous penicillin for the fluoroquinolones. For adults and children older than 12 years, penicillin G at 4 million U IV q4h is recommended for 60 days. For children younger than 12 years, penicillin G is dosed 50,000 U/kg IV q6h for 60 days.
In experimental models, antibiotic therapy during anthrax infection has prevented development of an immune response. This suggests that even if the antibiotic-treated patient survives anthrax infection, risk of recurrence remains for at least 60 days. Oral therapy should replace intravenous therapy as soon as a patient's clinical condition improves.
Historically, the treatment of cutaneous anthrax has been with oral penicillin. Recent recommendations suggest that oral fluoroquinolones or tetracycline antibiotics, as well as amoxicillin, are suitable alternatives if antibiotic susceptibility is proven. Although previous guidelines have suggested treating cutaneous anthrax with 7-10 days of therapy, recent recommendations suggest treatment for 60 days in the setting of bioterrorism, given the presumed exposure to the primary aerosol. Treatment of cutaneous anthrax generally prevents progression to systemic disease, although it does not prevent the formation and evolution of the eschar.
There are currently two FDA approved monoclonal antibodies available for anthrax treatment via the CDC through the SNS: raxibacumab and obiltoxaximab. Both bind and neutralize the free protective antigen (PA) component of B anthracis toxin and are approved for the treatment of inhalational anthrax in combination with recommended antibiotic regimens. Neither cross the blood-brain barrier. Diphenhydramine should be given within 1 hour prior to infusion of both products to reduce the risk of infusion reactions. [25, 24]
In pregnant women, experts recommend giving ciprofloxacin for therapy and postexposure prophylaxis following an anthrax attack. Substitute intravenous penicillin for the fluoroquinolones if microbiologic testing confirms penicillin susceptibility.
Prophylaxis
For postexposure prophylaxis, experts recommend the same oral regimen as that recommended for treatment of mass casualties. For adults, administer ciprofloxacin 500 mg PO bid for 60 days. Ciprofloxacin may be changed to amoxicillin 500 mg PO tid or doxycycline 100 mg PO bid for 60 days if microbiologic testing confirms such antibiotic susceptibility. In children, administer ciprofloxacin at 20-30 mg/kg/d PO taken twice daily (not to exceed 1 g/d) for 60 days. If the strain is susceptible to penicillins and the patient’s weight is greater than 20 kg, amoxicillin may be given at 500 mg PO tid. For a child who weighs less than 20 kg, amoxicillin is administered at 40 mg/kg/d divided tid for 60 days.
Raxibacumab and obiltoxaximab are indicated for prophylaxis of inhalational anthrax due to B anthracis when alternative therapies are not available or not appropriate. [26] Obiltoxaximab is a monoclonal antibody that binds to the protective antigen of B anthracis and prevents the formation of the anthrax toxin that directly damages cells. It disrupts cell defense mechanisms that lead to organ injury, uncontrolled bacterial growth, and death. [24]
A licensed vaccine, anthrax vaccine adsorbed (AVA), an aluminum hydroxide–adsorbed preparation, is derived from culture fluid supernatant taken from an attenuated strain. The current pre-exposure vaccination series consists of a primary series of 3 intramuscular doses at 0, 1, and 6 months, with boosters at 6 and 12 months after completion of the primary series and then annually—or every 3 years, in persons not at high risk for exposure to B anthracis. [26]
For postexposure prophylaxis (PEP) in combination with antibiotics, the dosage is 0.5 mL administered subcutaneously at 0, 2, and 4 weeks. If a large-scale attack occurs, dose-sparing PEP regimens may be recommended if the anthrax vaccine supply is insufficient to vaccinate all potentially exposed persons. AVA is approved for PEP in adults aged 18–65 years; it would be available for PEP use for children, pregnant women, nursing mothers, and adults older than 65 years under appropriate emergency use regulatory provisions. [26] Insufficient data are available regarding efficacy against inhalation anthrax in humans, although studies in rhesus monkeys indicate that it is protective.
If information indicates that a BW attack is imminent or may have occurred, prophylaxis with ciprofloxacin (500 mg PO bid) or doxycycline (100 mg PO bid) is recommended. Patients currently immunized (including annual boosters) need only continue antibiotic prophylaxis for 30 days. In unimmunized individuals, initiate PEP, if possible; should an anthrax attack be confirmed, continue chemoprophylaxis for at least 60 days or for 1-2 weeks after persons exposed receive PEP. Anthrax vaccine (AVA, and potentially an investigative anthrax vaccine, AV7909, as well) is available through the CDC Strategic National Stockpile under Investigational New Drug (IND) protocols.
For patient education information, see the First Aid and Injuries Center, as well as Anthrax.
Plague
Plague is a zoonotic infection caused by Yersinia pestis, a gram-negative coccobacillus, which has been the cause of three great human pandemics in the Common Era, in the 6th, 14th, and 20th centuries. Throughout history, the oriental rat flea (Xenopsylla cheopis) has been largely responsible for spreading bubonic plague. After the flea ingests a blood meal on a bacteremic animal, bacilli can multiply and essentially block the flea's foregut with a fibrinoid mass of bacteria. When an infected flea with a blocked foregut attempts to feed again, it regurgitates clotted blood and bacteria into the victim's bloodstream and so passes the infection onto the next victim, whether rat or human. As many as 24,000 organisms may be inoculated into the host.
Although the largest outbreaks of plague have been associated with X cheopis, all fleas should be considered dangerous in plague-endemic areas. The most important vector in the United States is Diamanus montanus, the most common flea of rock squirrels and California ground squirrels. The black rat, Rattus rattus, has been most responsible worldwide for the persistence and spread of plague in urban epidemics.
Plague is characterized by the abrupt onset of high fevers, painful lymphadenopathy, and bacteremia. Septicemic plague sometimes can ensue from untreated bubonic plague or, de novo, after a fleabite. Patients with the bubonic form of the disease may develop secondary pneumonic plague. This complication can lead to human-to-human spread by the respiratory route and cause primary pneumonic plague. Pneumonic plague is the most severe form of disease, with a mortality rate approaching 100% if not treated. [27]
Mortality from endemic plague continues at low rates throughout the world despite the availability of effective antibiotics. People continue to die of plague, not because the bacilli have become resistant but, most often, because physicians do not include plague in their differential diagnosis and treatment is delayed.
Pathophysiology
Y pestis is a gram-negative, non–acid-fast, nonmotile, nonsporulating coccobacillus. The bacteria may remain viable for days to weeks in water, moist soil, grain, and buried bodies. Its bipolar appearance is best appreciated when Wright-Giemsa, Wayson, or Gram stains are used. Y pestis grows optimally at 28°C. Biochemically, the plague bacillus produces no hemolysins, is positive for catalase, and is negative for hydrogen sulfide, oxidase, and urease.
The known virulence factors of Y pestis are encoded on the chromosomes of its three plasmids. The pH6 antigen, a protein located on the surface of the bacterium, is necessary for complete virulence. It is induced in vivo at sites of inflammation and cellular necrosis and within phagocytic cells. The low calcium response (LCR) plasmid, which is homologous in Y pestis and the other two Yersinia pathogens, Y pseudotuberculosis and Y enterocolitica, codes for several secreted proteins and is also necessary for virulence.
As few as 1-10 organisms of Y pestis are sufficient to infect rodents and primates via the oral, intradermal, subcutaneous, or intravenous routes. After being introduced into the mammalian host by a flea, the organism is thought to be susceptible initially to phagocytosis and killing by neutrophils. However, some of the bacteria may grow and proliferate within tissue macrophages. Within the human host, several environmental signals (temperature of 37°C, contact with eukaryotic cells, location within mononuclear cells, pH) are thought to induce the synthesis and activity of a multitude of factors that contribute to virulence. Bacteria become resistant to phagocytosis and proliferate unimpeded extracellularly.
During the incubation phase, the bacilli most commonly spread to regional lymph nodes, where supportive lymphadenitis develops, producing the characteristic bubo (1-10 cm in diameter). Dissemination from the local site is thought to be related to the action of both plasminogen activator and Yop M. Infection progresses if untreated; septicemia develops, and the infection spreads to other organs. The endotoxin probably contributes to the development of septic shock, which is similar to the shock states observed in sepsis from other gram-negative bacteria.
Tissues most commonly infected include the spleen, liver, lungs, skin, and mucous membranes. Late infection of the meninges also occurs, especially if suboptimal antibiotic therapy has been administered.
Primary pneumonic plague, the most severe form of the disease, arises from inhalation of an infectious aerosol. Primary pneumonic plague is more rapidly fatal than the secondary form, because the inhaled droplets already contain phagocytosis-resistant bacilli, which have arisen from their growth in the vertebrate host.
Primary septicemia plague can arise from direct inoculation of bacilli into the bloodstream, bypassing initial multiplication in the lymph nodes.
Clinical features
Plague presents in three predominant forms. In the United States, 85-90% of patients present clinically with the bubonic form, 10-15% with the primary septicemia form, and 1% with the pneumonic form. Secondary septicemic plague occurs in 23% of patients who present with bubonic plague, and secondary pneumonic plague occurs in 9%. If Y pestis were used as a BW agent, it most likely would be inhaled as an infectious aerosol and result in primary pneumonic plague (epidemic pneumonia). If fleas were used as carriers of disease, bubonic or septicemic plague would result.
In bubonic plague, buboes manifest with a 1- to 8-day incubation period after infection via flea bite. Their appearance is associated with the onset of sudden fever, chills, and headache, often followed by nausea and vomiting several hours later. Presenting symptoms include the following:
-
Severe malaise (75%)
-
Headache (20-85%)
-
Vomiting (25-49%)
-
Chills (40%)
-
Altered mentation (26-38%)
-
Cough (25%)
-
Abdominal pain (19%)
-
Chest pain (13%)
Buboes occur in the groin (90% femoral, more frequent femoral than inguinal), axillary, or cervical regions, depending on the site of inoculation, 6-8 hours after the onset of symptoms. Buboes become visible within 24 hours and are characterized by severe pain. Untreated, mortality is 60%. Septicemia develops in 2-6 days in 25% of patients who are untreated. Approximately 5-15% of patients with bubonic plague develop secondary pneumonic plague.
Septicemia plague may occur primarily or secondarily as a result of hematogenous dissemination of bubonic plague. Presenting signs and symptoms of primary septicemic plague are essentially the same as those for any gram-negative septicemia and include fever, chills, nausea, vomiting, and diarrhea; later, purpura, disseminated intravascular coagulation (DIC), and acrocyanosis and necrosis occur. The mortality rate is nearly 100% without treatment, but 30-50% with treatment.
Pneumonic plague may occur primarily from inhalation of aerosols or secondarily from hematogenous dissemination. Humans contract this form from domestic cats in 28% of cases (25% of these patients are veterinarians or their assistants). Patients typically have a productive cough with blood-tinged sputum within 24 hours of symptom onset. The findings on chest radiographs are variable, but bilateral alveolar infiltrates appear to be the most common findings in pneumonic plague. Human-to-human spread is unusual; in fact, it has not occurred in the United States since 1925. Untreated, the mortality rate is nearly 100%.
Plague meningitis is observed in 6-7% of patients. The condition manifests itself most often in children after 9-14 days of ineffective treatment. Symptoms are similar to those of other forms of acute bacterial meningitis.
Diagnosis
The diagnosis of bubonic plague should be made readily on clinical grounds if a patient presents with a painful bubo, fever, prostration, and history of exposure to rodents or fleas in an endemic area. However, if the patient presents in a nonendemic area or without a bubo, then the diagnosis can be difficult to make. When a bubo is present, the differential diagnosis should include the following:
-
Tularemia
-
Chancroid
-
TB
-
Streptococcal adenitis
-
Scrub typhus
The differential diagnosis of septicemic plague also includes meningococcemia, other gram-negative sepsis, and rickettsioses. A presentation of systemic toxicity, a productive cough, and bloody sputum suggests a large differential diagnosis. However, demonstration of gram-negative coccobacilli in the sputum readily should suggest the correct diagnosis, because Y pestis is perhaps the only gram-negative bacterium that can cause extensive, fulminant pneumonia with bloody sputum in an otherwise healthy, immunocompetent host. In addition, Y pestis has unique bipolar, safety-pin morphology.
In patients with lymphadenopathy, perform a bubo aspiration. Air-dry the aspirate on a slide for Gram, Wright-Giemsa, or Wayson stain. If available, obtain a direct fluorescent antibody (DFA) stain of the aspirate for the presence of Y pestis capsular antigen. A positive DFA is more specific for Y pestis than the other stains listed.
Perform cultures of blood, bubo aspirate, sputum, and CSF. Tiny 1- to 3-mm beaten-copper colonies appear on blood agar in 48 hours. It is important to remember that colonies may be negative at 24 hours.
Complete blood cell counts (CBCs) often reveal leukocytosis with a left shift. Platelet counts may be normal or low, and activated partial thromboplastin times (aPTTs) may be increased. When DIC is present, fibrin degradation products are elevated. Because of liver involvement, alanine aminotransferase, aspartate aminotransferase, and bilirubin levels may be increased.
Most naturally occurring strains of Y pestis produce an F1-antigen in vivo, which can be detected in serum samples by immunoassay. Because fractional antigen and antibody do not occur early in the infection, perform titers for both on several sequential blood specimens. A 4-fold rise in antibody titer in patient serum is retrospectively diagnostic. Polymerase chain reaction (PCR) testing is very specific and sensitive but is not widely available.
Treatment
Because the risk of human-to-human transmission, isolate patients with plague for the first 48 hours after treatment initiation. If pneumonic plague is present, continue isolation for 4 days.
Since 1948, streptomycin has been the treatment of choice for bubonic, septicemic, and pneumonic plague. Administer it in a dose of 30 mg/kg/d IM divided bid. In patients with meningitis or hemodynamic instability, add intravenous chloramphenicol (50-75 mg/kg/d) divided qid. Gentamicin (5 mg/kg/d IM or IV) has had much less clinical usage but can be used as an alternative to streptomycin. Continue treatment for a minimum of 10 days or 3-4 days after clinical recovery. In patients with very mild bubonic plague who are not septic, tetracycline can be used orally at a dose of 2 g/d divided qid for 10 days. Doxycycline, ciprofloxacin, ofloxacin, chloramphenicol, andceftriaxone may be used as alternatives. [22]
In pregnant women, use streptomycin or gentamicin unless chloramphenicol specifically is indicated. Streptomycin is also the treatment of choice for newborns and children (15 mg/kg IM bid up to a maximum of 2 g/d). Doxycycline or ciprofloxacin are considered alternatives for both pregnant woman and children. Augmentin is also used during pregnancy and for children < 8 years old. [22]
With antibiotic treatment, buboes typically recede in 10-14 days and do not require drainage. Patients are unlikely to survive primary pneumonic plague if antibiotic therapy is not initiated within 18-24 hours of symptom onset.
Prevention and prophylaxis
All plague control measures must include insecticide use, public education, and reduction of rodent populations with agents such as cholecalciferol. Fleas always must be targeted before rodents, because killing rodents may release massive amounts of infected fleas.
Treat contacts of patients with pneumonic plague and individuals who have been exposed to aerosols with oral doxycycline or ciprofloxacin for 7 days. Chloramphenicol is an alternative. In addition, previously vaccinated individuals should also receive prophylactic antibiotics if they have been exposed to a plague aerosol.
No vaccine for plague has been available in the US since 1998; however, a F1-V antigen vaccine is currently under development by the US Army.
For patient education information, see the First Aid and Injuries Center, as well as Plague.
Tularemia
Tularemia is a zoonosis caused by the gram-negative, facultative intracellular bacterium Francisella tularensis. The disease is characterized by fever, localized skin or mucous membrane ulceration, regional lymphadenopathy, and occasionally pneumonia. GW McCoy discovered the disease in Tulare County, California, in 1911. The first confirmed case of human disease was reported in 1914. Edward Francis, who described transmission by deer flies via infected blood, coined the term tularemia in 1921. F tularensis has been considered an important potential BW agent because of its high infectivity after aerosolization.
F tularensis is a nonmotile, obligate aerobic, gram-negative coccobacillus with 2 subspecies. F tularensis subsp tularensis (biovar A) is the most common in the United States. F tularensis subsp palearctica (biovar B) is more common outside the United States. The subspecies are indistinguishable serologically, although they may be distinguished by 169 ribosomal ribonucleic acid (rRNA) analysis. A capsule has been reported to contribute to virulence. No known toxins are produced. The bacteria can remain viable for weeks in water, soil, and hides and for years in frozen rabbit meat; but it is heat labile.
The principal reservoir in North America is the tick, but F tularensis can also be transmitted by infected deer flies and mosquitoes. Naturally occurring tularemia can also be acquired when infected body fluid or tissue comes into contact with broken skin or mucous membranes. In North America, the rabbit is the most common vertebrate associated with transmission of tularemia. In other areas of the world, tularemia is maintained in water rats and other aquatic animals.
Pathophysiology
F tularensis usually is introduced into the host through breaks in the skin or through the mucous membranes of the eye, respiratory tract, or GI tract. Ten virulent organisms injected subcutaneously and 10-50 organisms given by aerosol can cause infection in humans. After inoculation, F tularensis is ingested by and multiplies within macrophages. The host defense against F tularensis is mediated by a T-cell–independent mechanism, which appears early after infection (< 3 d), and a T-cell–dependent mechanism, which appears later (> 3 d) after infection. The role of humoral-mediated immunity and neutrophils in the host defense against F tularensis remains unclear.
Clinical Features
Tularemia can be divided into the ulceroglandular (75-85% of patients) and typhoidal (15-25% of patients) forms based on clinical findings. After an incubation period of 2-10 days, patients with the ulceroglandular form of the disease, which is usually acquired through inoculation of the skin or mucous membranes, develop a constellation of symptoms consisting of fever (85%), chills (57%), headache (45%), cough (38%), and myalgia (31%). Patients may also complain of chest pain, vomiting, arthralgia, sore throat, abdominal pain, diarrhea, dyspnea, back pain, or neck stiffness. Patients with ulceroglandular tularemia have lesions of the skin or mucous membranes, lymph nodes greater than 1 cm in diameter, or both. Ulceroglandular tularemia lesions are shown in the photos below.



Typhoidal tularemia mainly occurs after inhalation and presents with lymph nodes less than 1 cm in diameter and without skin or mucous membrane lesions.
A typical ulcer of tularemia is shown below.
 Typical heaped up ulcer of tularemia. Reprinted from Evans ME, Friedlander AM. Tularemia. Chapter 24. In: Sidell FR, Takafuji ET, Franz DR, eds. Medical Aspects of Chemical and Biological Warfare. In: Zajtchuck R, Bellamy RF, eds. Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997:505.
Typical heaped up ulcer of tularemia. Reprinted from Evans ME, Friedlander AM. Tularemia. Chapter 24. In: Sidell FR, Takafuji ET, Franz DR, eds. Medical Aspects of Chemical and Biological Warfare. In: Zajtchuck R, Bellamy RF, eds. Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997:505.
A cutaneous chancrelike ulcer occurs in approximately 60% of patients and is the most common sign of tularemia. Ulcers are generally single lesions with heaped up borders 0.4-3 cm in diameter. Lesions associated with infection acquired from mammalian vectors usually are located on the upper extremities, whereas lesions associated with infection from arthropod vectors usually are located on the lower extremities.
Enlarged lymph nodes are observed in approximately 85% of patients and may be the initial or the only sign of infection. Although enlarged lymph nodes usually occur as single lesions, they may appear in groups. The appearance of enlarged lymph nodes in upper or lower extremities and the correlation with the vector is the same as for ulcerative lesions. Enlarged lymph nodes may become fluctuant, drain spontaneously, or persist for as long as 3 years. When fluctuant, they may be confused with buboes of bubonic plague. A minority of patients with typhoidal disease develop a morbilliform eruption.
Pharyngitis may occur in as many as 25% of patients with tularemia. On occasion, patients with pharyngitis also may develop a retropharyngeal abscess or suppuration of regional lymph nodes. Pharyngeal ulcers may be found in patients with aerosol-induced disease.
The lower respiratory tract is involved in 47-94% of patients. Approximately 30% of patients with ulceroglandular and 80% of patients with typhoidal tularemia have pneumonia. Patients present with productive or nonproductive cough and less commonly with pleuritic chest pain, shortness of breath, or hemoptysis. Fifty percent of patients have radiographic evidence of pneumonia, and 1% or fewer have hilar adenopathy. Pleural effusions are observed in 15% of patients with pneumonia.
Oculoglandular disease occurs in 1-2% after primary inoculation of the conjunctiva. Painful, purulent unilateral conjunctivitis with preauricular and/or cervical lymphadenopathy is seen.
The mortality rate is 35% if untreated. Those with pneumonia have a greater risk of death, with up to a 60% mortality rate.
Diagnosis
Tularemia can be diagnosed by recovery of F tularensis in culture. Although difficult to culture, it can be recovered from blood, ulcers, sputum, conjunctival exudate, pharyngeal exudates, and gastric washings. On media containing cysteine, F tularensis appears as small, smooth, opaque colonies after 24-48 hours of incubation at 37°C. Identification of the organism is made on the basis of its growth characteristics and bacterial agglutination or fluorescent stain using antiserum specific for F tularensis.
Most diagnoses of tularemia are made serologically by using bacterial agglutination or ELISA. The serologic response may be blunted by the use of antibiotics and may not appear for more than 2 weeks. A 4-fold or greater increase in titer is required to make the diagnosis. Rapid diagnostic testing using DFA and PCR is available through the CDC.
Patients usually do not have abnormalities in the hemoglobin, hematocrit, or platelet count. The peripheral white blood cell count usually is elevated only mildly and often shows a lymphocytosis late in the disease. Patients may have microscopic pyuria, which may lead to erroneous diagnosis of urinary tract infection. Some patients demonstrate mild elevations in levels of lactate dehydrogenase, serum transaminases, and alkaline phosphatase. CSF is usually normal.
Treatment
Patients with tularemia who do not receive appropriate antibiotic therapy may have a prolonged illness characterized by malaise, weakness, and weight loss. With appropriate therapy, tularemia has a mortality rate of only 1-2.5%.
Antibiotics used to treat tularemia include streptomycin, gentamicin, doxycycline, and ciprofloxacin. Streptomycin (30 mg/kg/d IM divided bid for 10-14 d) is the drug of choice for tularemia. Gentamicin (3-5 mg/kg/d parenterally for 10-14 d) is also effective. Doxycycline, ciprofloxacin, and chloramphenicol are also effective but have been associated with significant relapse rates. Although laboratory-related infections with this organism are common, human-to-human spread is unusual, and respiratory isolation is not required.
Patients typically improve dramatically within 24-48 hours of initiation of antibiotic treatment. Failure to improve during by this time frame may indicate resistance to the antibiotic.
Prevention and prophylaxis
No human-to-human transmission of tularemia occurs, but standard precautions should be used for patients with pneumonia or wounds.
Antibiotic prophylaxis after exposure to tularemia should begin with 24 hours and should be administered for 14 days. Doxycycline or ciprofloxacin are the drugs of choice. Prophylaxis is not indicated after tick bites or other potential animal exposures.
A live-attenuated Investigational New Drug (IND) vaccine has been developed and used in humans since 1940. In the 1960s, a further purified derivative was introduced and called live vaccine strain (LVS). Extensive studies have demonstrated that the LVS vaccine protected humans against an aerosol challenge with virulent F tularensis. Evidence indicates that immunization with the LVS vaccine prevents the typhoidal form and ameliorates the ulceroglandular forms of tularemia.
Brucellosis
Brucellosis is a zoonotic infection of domesticated and wild animals caused by an organism of the genus Brucella. The organism infects mainly cattle, sheep, goats, and other ruminants, causing abortion, fetal death, and genital infection. Humans are infected incidentally by contact with infected animals, tissues or discharges, blood, urine, or by ingesting unpasteurized milk products. They may develop numerous symptoms in addition to the usual ones of fever, malaise, and muscle pain. The disease often becomes chronic and may relapse, even with appropriate treatment. The ease of transmission by aerosol suggests that Brucella species may be useful as a BW agent. [28, 29]
Pathophysiology
Brucella species are small, nonmotile, nonsporulating, aerobic, gram-negative coccobacilli that may represent a single species. However, they are classified into six species. Each species has a characteristic predilection to infect certain animal species. Only Brucella melitensis,B suis,B abortus, and B canis cause disease in humans. Only 10-100 organisms are required to cause human disease. Infection of humans with B ovis and B neotomae has not been described.
Animals may transmit Brucella organisms during septic abortion, at the time of slaughter, and in their milk. Brucellosis rarely, if ever, is transmitted from human to human. Brucella species can enter mammalian hosts through skin abrasions or cuts, the conjunctiva, the respiratory tract, and the GI tract. Organisms are ingested rapidly by polymorphonuclear leukocytes, which generally fail to kill them. Organisms also are phagocytized by macrophages, which traffic to lymphoid tissue and eventually localize in the lymph nodes, liver, spleen, joints, kidneys, and bone marrow.
Brucellosis also can replicate extracellularly in host tissue. The host cellular response may range from abscess formation to granuloma formation with caseous necrosis.
Clinical Features
Clinical manifestations of brucellosis are diverse, and the course of the disease varies. Patients may present with an acute, systemic, febrile illness; an insidious chronic infection; or a localized inflammatory process. The disease may be abrupt or insidious in onset, with an incubation period of 3 days to several months. Patients usually have nonspecific symptoms such as fever, malaise, sweats, fatigue, anorexia, and muscle or joint aches. Neuropsychiatric symptoms such as depression, headache, and irritability occur frequently. In addition, focal infection of bones (including the spine), joints (monoarticular or polyarticular), or the genitourinary tract may cause local pain. Cough and pleuritic chest pain also may be noted.
Symptoms often last 3-6 months and occasionally for longer than a year. Brucellosis usually does not cause leukocytosis, and patients may be neutropenic. B melitensis tends to cause more severe, systemic illness than the other Brucella species. B suis is more likely to cause localized suppurative disease.
Infection with B melitensis leads to bone or joint disease in approximately 30% of patients. Sacroiliitis develops in 6-15%, particularly in young adults. Arthritis of large joints occurs with about the same frequency as sacroiliitis. In contrast to septic arthritis caused by pyogenic organisms, joint inflammation observed with B melitensis is mild, and erythema of overlying skin is uncommon. Synovial fluid is exudative, with cell counts in the low thousands, predominantly mononuclear. In both sacroiliitis and peripheral joint infections, destruction of bone is unusual. Organisms can be cultured from fluid in approximately 20% of patients. Spondylitis tends to affect middle-aged or elderly patients, causing back (usually lumbar) pain, local tenderness, and occasionally radicular symptoms.
Radiographic findings, similar to those of tuberculous infection, include disk space narrowing and epiphysitis. Paravertebral abscesses occur rarely. In contrast to frequent infection of the axial skeleton, osteomyelitis of long bones is rare.
Infection of the genitourinary tract, an important target in ruminant animals, also may lead to signs and symptoms of disease in humans. Pyelonephritis, cystitis, and, in males, epididymo-orchitis may occur. Both diseases may mimic their tuberculous counterparts with sterile pyuria on routine bacteriologic cultures.
Lung infections also have been described. Although as many as 25% of patients may complain of respiratory symptoms (mostly cough, dyspnea, or pleuritic pain), chest radiographic examinations usually are normal. Diffuse or focal infiltrates, pleural effusions, abscesses, and granulomas may be observed.
Hepatitis and, rarely, liver abscess also occur. Mild elevations of serum lactate dehydrogenate and alkaline phosphatase levels are common. Biopsy may show well-formed granulomas or nonspecific hepatitis with collections of mononuclear cells.
Other sites of infection include the heart, central nervous system (CNS), and skin. Brucella endocarditis, a rare but feared complication, accounts for 80% of deaths from brucellosis. CNS infection usually manifests as chronic meningoencephalitis, but subarachnoid hemorrhage and myelitis also occur. Cases of skin abscess also have been reported.
Diagnosis
A thorough history eliciting details of appropriate exposures (animals, animal products, environmental exposures) is the most important diagnostic tool. Strongly consider brucellosis in the differential diagnosis when military troops exposed to a biological attack have febrile illnesses. PCR and antibody-based antigen detection systems may demonstrate the presence of organisms in environmental samples collected from attack areas.
When the disease is considered, diagnosis usually is made based on serology. The tube agglutination test remains the criterion standard. This test reflects the presence of anti-O-polysaccharide antibody. Most patients already have high titers at the time of clinical presentation. A 4-fold rise in agglutination titer between acute and convalescent sera (2 wk apart) is diagnostic. Serum testing always should include dilution to at least 1:320. The tube agglutination test does not detect antibodies to B canis, because this organism does not have O-polysaccharide on its surface. ELISA and PCR tests are also available.
In addition to serologic testing, pursue diagnosis by microbiologic cultures of blood or body fluid samples. Hold cultures for at least 2 months. The reported frequency of isolation from blood varies widely, from less than 10% to 90%. B melitensis is said to be cultured more readily than B abortus. Culture of bone marrow may increase the yield.
Treatment
Therapy with a single drug has resulted in a high relapse rate, so use combined antibiotic regimens whenever possible. A 6-week regimen of doxycycline 100 mg PO bid with the addition of streptomycin 1 g/d IM for the first 2-3 weeks is effective in most adults with most forms of brucellosis. Patients with spondylitis may require longer treatment. A 6-week oral regimen with both rifampin 900 mg/d and doxycycline 200 mg/d is effective. Several studies have demonstrated that treatment with a combination of streptomycin and doxycycline may result in less frequent relapse than treatment with the combination of rifampin and doxycycline. Alternatives include ciprofloxacin plus rifampin, or trimethoprim/sulfamethoxazole plus rifampin.
Endocarditis and bone disease likely is best treated with a triple-drug combination of rifampin, streptomycin (or gentamicin), and doxycycline for 6 weeks. Replace infected valves early. CNS disease responds to a combination of rifampin and trimethoprim/sulfamethoxazole but may need prolonged therapy. The latter combination is also effective for children younger than 8 years. Rifampin is recommended for pregnant women.
Prevention/Prophylaxis
Animal handlers should wear appropriate protective clothing when working with infected animals. Meat should be well cooked, and milk should be pasteurized. Laboratory workers should culture the organism only with appropriate Biosafety level 2 or 3.
In the event of a biological attack, the standard gas mask should protect personnel adequately from airborne Brucella species. Brucellosis is not generally transmitted from human to human. No commercially available vaccine exists for humans. A 3- to 6-week course of a single antibiotic should be considered after exposure by percutaneous, mucous membrane, or aerosolization routes.
Q Fever
Q fever (or Query fever) is a zoonotic disease caused by Coxiella burnetii, a rickettsialike organism of low virulence but remarkable infectivity. A single organism may initiate infection. In addition, despite the fact that C burnetii is unable to grow or replicate outside host cells, a sporelike form of the organism is extremely resistant to heat, pressure, and many antiseptic compounds. This allows C burnetii to persist in the environment for long periods under harsh conditions. In contrast to this high degree of inherent resilience and transmissibility, the acute clinical disease associated with Q fever is usually a benign, although temporarily incapacitating, illness in humans. Even without treatment, most patients recover.
The primary reservoir for natural human infection is livestock, particularly parturient females, and the distribution is worldwide. Humans who work in animal husbandry, especially those who assist during parturition, are at risk of acquiring Q fever.
The potential of C burnetii as a BW agent is related directly to its infectivity. It has been estimated that 50 kg of dried C burnetii would produce casualties at a rate equal to that of similar amounts of anthrax or tularemia organisms.
The causative agent of Q fever was designated Coxiella burnetii to recognize the outstanding contribution of both Harold Cox and MacFarlane Burnet in the isolation and characterization of the pathogen in 1937 and 1938. The disease now has been identified in at least 51 countries and on 5 continents.
Pathophysiology
The genus Coxiella has only 1 species. C burnetii is extremely infectious. Under experimental conditions, a single organism is capable of producing infection and disease in humans.
The host range of C burnetii is diverse and includes a large number of mammalian species and arthropods. Among these, the human is the only host identified that experiences illness as a result of infection. A number of different strains of C burnetii have been identified worldwide, and different clinical manifestations and complications may be associated with the various strains.
Humans have been infected most commonly by contact with domestic livestock, particularly goats, cattle, and sheep. The risk of infection is increased substantially if humans are exposed to these animals at parturition. During gestation, the proliferation of C burnetii in the placenta facilitates aerosolization of large numbers of the pathogen during parturition. Survival of the organism on inanimate surfaces, such as straw, hay, or clothing, allows for transmission to individuals who are not in direct contact with infected animals.
Human infection with C burnetii is usually the result of inhalation of infected aerosols, but may also occur after consumption of unpasteurized dairy products. Following this, host cells phagocytize the organisms. After phagocytosis by host cells, dissemination of the pathogen occurs as a result of circulation of organism free in the plasma, on the surface of the cells, and carried by circulatory macrophages.
Little host reaction occurs at the initial portal of entry, either in the lung following inhalation of aerosol or in the skin following a tick bite. Q fever develops without formation of a primary infectious focus in the area of the tick bite, and the organism does not infect the vascular endothelium, as do other rickettsial pathogens. The presence of a lipopolysaccharide on the cell surface of C burnetii protects the pathogen from host microbicidal activity.
Clinical features
Humans are the only hosts that commonly develop an illness as a result of the infection. Incubation varies from 2-40 days (mean, 15 d). The duration of the incubation period correlates inversely with the magnitude of the inoculum. A higher inoculum also increases the severity of the disease. Q fever in humans may be manifested by asymptomatic seroconversion, acute illness, or chronic disease. The frequency of chronic disease (usually endocarditis) is probably less than 1% of the total infected population.
No characteristic illness is described for acute Q fever, and manifestations may vary considerably between locations where the disease is acquired. The onset of symptomatic Q fever may be abrupt or insidious. Fever, chills, and headache are the most common signs and symptoms. Diaphoresis, malaise, myalgias, fatigue, and anorexia are also common. Arthralgias are relatively uncommon. Cough often occurs later in the illness. Chest pain occurs in a minority of patients. Although nonspecific, evanescent skin eruptions have been reported. No characteristic rash results.
Most patients appear mildly to moderately ill. The temperature tends to fluctuate, with peaks at 39-40°C, and is biphasic in approximately 25% of patients. The fever generally lasts less than 13 days but has been reported to last longer in older adults. Fewer than 5% of patients require hospitalization.
Encephalopathic symptoms, headache, hallucinations (visual, auditory), expressive dysphasia, facial pain resembling trigeminal neuralgia, diplopia, and dysarthria have been reported.
Physical findings in acute Q fever are as nonspecific as the clinical symptomatology. Rales are probably the most commonly observed physical finding; evidence of pleural effusion and consolidation also may be noted but not in most cases.
Reports of abnormalities on chest radiographic examination vary with locale, but abnormalities probably are observed 50-60% of the time. The most common abnormality reported is a unilateral homogeneous infiltrate involving 1 or 2 lobes such as is seen with atypical pneumonia. There is a predilection for the lower lobes. Rounded opacities and hilar adenopathy are not uncommon. Consider the diagnosis of Q fever when these abnormalities are observed in the setting of acute pneumonia.
Patients with acute Q fever may present with a clinical picture of acute hepatitis, with aminotransferase levels 2- to 3-fold higher than the upper limit of normal. The total bilirubin can be expected to be elevated in 10-15% of patients with acute Q fever. The white blood cell count is usually normal. The erythrocyte sedimentation rate is elevated in 33% of patients. Mild anemia or thrombocytopenia also may be observed.
Chronic infection with C burnetii usually is manifested by infective endocarditis, which also is the most severe complication of Q fever. In addition, hepatitis, infected vascular prostheses, aneurysms, osteomyelitis, pulmonary infection, cutaneous infection, and an asymptomatic form have been reported.
In Q fever endocarditis, fever has been recorded in 85% of patients, along with other systemic symptoms (eg, chills, headache, myalgias, weight loss). Other frequently reported clinical features of Q fever endocarditis include heart failure, splenomegaly, hepatomegaly, clubbing, and cutaneous signs. Routine blood cultures in patients with Q fever endocarditis are negative, and Q fever should be considered when culture-negative endocarditis is encountered. The diagnosis of infective endocarditis secondary to Q fever is confirmed by serologic testing.
Diagnosis
Diagnosis of Q fever usually is accomplished using serologic testing; the most common methods are complement fixation, indirect fluorescent antibody, and ELISA. Significant antibody titers usually are not identifiable until 2-3 weeks into the illness.
Of the methods currently used for the diagnosis of Q fever, ELISA is the most sensitive and easiest to perform. This assay can establish a diagnosis of Q fever from a single serum specimen with a sensitivity of 80-84% in early convalescence and 100% in intermediate and late convalescence.
Treatment
The mortality rate from Q fever is less than 3%, and most patients recover without treatment within several months. Because of the risk of severe complications, including death, all patients should be treated with antibiotics. Tetracyclines have been the mainstay of therapy since the 1950s. Doxycycline 100 mg PO bid is the drug of choice and is administered for 2 weeks. When initiated within the first few days of the illness, treatment significantly shortens its course. Macrolide antibiotics, such as erythromycin and azithromycin, and trimethoprim/sulfamethoxazole are also effective. Fluoroquinolones have better penetration into the CNS and should be continued for 2-3 weeks if used.
When chronic Q fever infection is manifested by infective endocarditis, the mortality rate is 24% even when patients receive appropriate treatment. At least 1.5-2 years of therapy are required, usually with a combination of doxycycline and a fluoroquinolone, or doxycycline and hydroxychloroquine.
Prevention and prophylaxis
Nosocomial transmission to health care workers is possible, so standard infectious disease precautions should be utilized.
Although an effective vaccine (Q-Vax) is available in Australia and eastern Europe, Q fever vaccines available in the United States are investigational.
Chemoprophylaxis with doxycycline is effective if started between 8 and 12 days after exposure (but not before).
Viral Agents
Smallpox
Variola, the causative agent of smallpox, is the most notorious of the poxviruses (family Poxviridae, genus Orthopoxvirus). Smallpox was an important cause of morbidity and mortality in the developing world until recent times. In 1980, the World Health Organization (WHO) declared endemic smallpox eradicated, with the last occurrence in Somalia in 1977.
Variola represents a significant threat as a BW agent. Variola is highly infectious and is associated with a high mortality rate and secondary spread. Routine vaccination stopped in the United States in 1972 for civilians and in 1989 for military personnel. The United States began vaccination again in 2003 with more than 400,000 military personnel and 38,000 emergency and health care workers vaccinated; however, the remainder of the civilian population is at risk for smallpox. Currently, two WHO-approved and inspected repositories remain: the CDC in the United States and Vector Laboratories in Russia; however, clandestine stockpiles may exist.
Pathophysiology
Variola virus is highly infectious by aerosol, environmentally stable, and can retain infectivity for long periods. Infection through contaminated fomites is infrequent. After exposure to aerosolized virus, the virus multiplies locally in the respiratory tract. After an incubation period of 7-17 days (mean 12 d), variola spreads hematogenously (primary viremia) to regional lymph nodes, where additional replication occurs. Subsequently, variola spreads hematogenously (secondary viremia) to small dermal blood vessels, where skin inflammatory changes (pox) occur.
Two types of smallpox generally are recognized. Variola major, the most severe form, has a fatality rate of 30% in unvaccinated individuals and 3% in those previously vaccinated. Variola minor, a more mild form of smallpox, is lethal in only 1% of unvaccinated individuals.
Clinical manifestations
After the incubation period, symptoms begin acutely with high fever, headache, rigors, malaise, myalgias, vomiting, and abdominal and back pain. During the initial phase, 15% of patients develop delirium, and 10% of light-skinned patients may develop a fleeting erythematous exanthem. After 2-3 days, an exanthem develops on the face, hands, and forearms and extends gradually to the trunk and lower extremities. The lesions progress synchronously from macules to papules to vesicles to pustules that often are umbilicated, such as in molluscum contagiosum. Centrifugal distribution of the rash is an important diagnostic feature, with a greater number of lesions on the face and extremities compared with the trunk. Patients are most infectious on days 3-6 after the onset of fever. Painful ulcerations of the tongue and oropharynx occur. Virus is shed from oropharyngeal and respiratory secretions.
The pustules form scabs 8-14 days after their eruption with depressed depigmented scars upon healing. Death occurs in the second week and is attributed to toxemia with high levels of circulating immune complexes. Patients are infectious until all scabs have separated. The photo below shows pustular lesions covering the patient's body.
 Adult with variola major with hundreds of pustular lesions distributed centrifugally. Photo courtesy of Fitzsimons Army Medical Center Slide File.
Adult with variola major with hundreds of pustular lesions distributed centrifugally. Photo courtesy of Fitzsimons Army Medical Center Slide File.
The photos below show variola major in an unvaccinated child.
 Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 3 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 3 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
 Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 5 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 5 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
 Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 7 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 7 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
The above-described manifestations are known as variola major. In variola minor (ie, alastrim), cutaneous lesions are similar but smaller and fewer in number. Patients are not as ill as those who have variola major.
The photos below show the lesions of variola minor.
 The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
 The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
 The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
Small numbers (3%) of patients develop hemorrhagic lesions, shown below, and these patients typically die of disease before papules develop. Flat smallpox with macular, soft, velvety lesions develops in 4% of patients and forebodes a poor prognosis.
 Hemorrhagic-type variola major lesions. Death usually ensued before typical pustules developed. Reprinted with permission from the World Health Organization (WHO). 1988; 10-14, 35-36.
Hemorrhagic-type variola major lesions. Death usually ensued before typical pustules developed. Reprinted with permission from the World Health Organization (WHO). 1988; 10-14, 35-36.
Modified smallpox occurs in those who have been vaccinated. It is characterized by a mild prodrome with rapid development of lesions and crusting by day 7. Frequently, no pustules form.
Diagnosis
The most difficult aspect of diagnosing smallpox is the current lack of familiarity with the disease for most physicians. Other viral exanthems, such as chicken pox, erythema multiforme with bullae, or allergic contact dermatitis, can look similar. Smallpox is distinguished from chicken pox by the centrifugal distribution of its rash and the presence of lesions at the same stage of development everywhere on the body. The failure to recognize mild cases of smallpox in persons with partial immunity permits rapid person-to-person transmission. Exposed people may shed virus from the oropharynx without ever manifesting disease.
The usual method of diagnosis is demonstration of characteristic Orthopoxvirus virions on electron microscopy of vesicular scrapings. Gispen modified silver stain is rapid but relatively insensitive. When microscopy is unavailable, the gel diffusion test, in which vesicular fluid antigen from a pus lesion is incubated with vaccine hyperimmune serum, may be used. However, none of the above tests differentiate smallpox from monkeypox or cowpox. PCR techniques have been developed and may provide for more accurate diagnosis as this test becomes more widely available.
Treatment
It is critical for medical personnel to recognize a vesicular exanthem in possible terrorist areas or warfare theaters as possible smallpox. Immediate reporting of all possible cases must be made to public health authorities and to the chain of command. Strict quarantine with respiratory isolation for 17 days is applied to all people in direct contact with the index case or cases. The historical secondary attack rate in unvaccinated household contacts was 58% and nearly 4% in those who had been vaccinated.
All personnel exposed to either weaponized variola or clinical cases must be vaccinated immediately. Vaccination is effective at ameliorating or preventing illness if accomplished within 4 days of exposure. Administer vaccinia immune globulin (VIG) to patients who cannot receive the vaccine. Vials of older VIG are stored at the CDC and are available only under IND protocols. A new intravenous formulation of VIG (IV-VIG) is being produced to support the treatment of adverse events that may result from smallpox vaccination. IV-VIG is available from the CDC under IND. The CDC can be contacted through the Clinicians Information Hotline at 1-877-554-4625 for VIG requests.
Treatment of smallpox is mainly supportive. The antiviral agent cidofovir is effective in vitro and may be involved in treatment of symptomatic illness. A cidofovir oral prodrug is in development. Topical trifluridine or idoxuridine may be used to treat ocular disease.
Emergency management guidelines recognize the importance of oral antivirals and call for having at least two smallpox antivirals with different mechanisms of action available in the event of a smallpox outbreak. Multiple antivirals are recommended due in large part to the propensity of viruses to become resistant to antiviral therapy, especially monotherapy. Currently, tecovirimat and cidofovir are stockpiled in the US; however, cidofovir requires intravenous infusion, which would limit its utility in a widespread outbreak. [30]
Brincidofovir, an oral antiviral in late stage development, has proven effective against orthopoxviruses in vitro and in vivo, has a different mechanism of action from tecovirimat (the only oral smallpox antiviral currently in the US Strategic National Stockpile). It has a resistance profile that reduces concerns in the scenario of a bioterror attack using genetically engineered smallpox. [30]
Prevention and prophylaxis
Smallpox vaccine is made from live vaccinia virus and does not contain variola virus (Wyeth Dryvax). It is administered by intradermal inoculation with a bifurcated needle. The permanent scar results from a process known as scarification. A vesicle usually appears 5-7 days after inoculation; scabbing over and healing of the site occur over the next 1-2 weeks. Common adverse effects include low-grade fever and axillary lymphadenopathy. The most frequent complication is inadvertent inoculation to other skin or mucous membrane sites or to other people. The CDC currently has enough vaccine to immunize the entire US population. For further information on adverse reactions and contraindications, visit the Centers for Disease Control and Prevention Web site.
Successful vaccination results in both antibody- and cell-mediated immunity; greater than 95% of primary vaccinees have detectable neutralizing antibody at a titer of 1:10 or more within 1-2 weeks after immunization. Protection against disease following primary vaccination begins to fade after 5 years and is probably negligible after 20 years. In individuals who have been successfully revaccinated one or more times, residual immunity may persist for 30 years or longer. Epidemiological evidence indicates that vaccination within 2-3 days after exposure to smallpox can result in protection against the disease and, even as late as 4-5 days, may protect against a fatal outcome.
JYNNEOS® (Smallpox and Monkeypox Vaccine, Live, Non-replicating) was approved by the FDA in 2019 for the prevention of smallpox and monkeypox in adults 18 years of age and older, and is now part of the Strategic National Stockpile. JYNNEOS® is a live vaccine produced from a modified form of the vaccina virus called Modified Vaccina Ankara, an attenuated, non-replicating orthopoxvirus, and is administered as subcutaneous injection of two doses given 4 weeks apart. [31]
The absolute contraindication to vaccination is significant impairment of systemic immunity. Relative contraindications include immunosuppression, HIV infection, pregnancy, and a history or evidence of eczema and other skin diseases.
For patient education information, see the First Aid and Injuries Center, as well as Smallpox.
Monkeypox
The monkeypox virus is a naturally occurring relative of variola that developed in Africa. The first case of human monkeypox was identified in 1970, with subsequently confirmed cases totaling less than 400. An outbreak of 81 human cases occurred in the United States in 2003 due to exposure to imported pets. That outbreak had no fatalities or secondary human-to-human transmission.
Some concern exists that monkeypox may be weaponized; however, human monkeypox is less virulent than smallpox. Monkeypox has a case-fatality rate of 11% in humans not vaccinated against smallpox. However, pneumonia due to monkeypox has approximately a 50% mortality rate. The secondary attack rate is only 9%, far lower than 25-40% rates observed in smallpox.
The clinical picture of monkeypox is clinically indistinguishable from smallpox, with the exception of enlarged cervical and inguinal lymph nodes. The virus is transmitted by respiratory aerosol or direct contact with an infected individual or fomites. Immunization to vaccinia virus provides protection to 85% of individuals exposed to monkeypox. The treatment of monkeypox remains supportive and clinical management is the same as with smallpox.
Viral Encephalitides
The viral encephalitides, Venezuelan equine encephalitis (VEE) virus, western equine encephalitis (WEE) virus, and eastern equine encephalitis (EEE) virus, are members of the Alphavirus genus and regularly are associated with encephalitis. These viruses first were recovered from horses during the 1930s. VEE was isolated in the Guajira peninsula of Venezuela in 1930, WEE in the San Joaquin Valley of California in 1930, and EEE in Virginia and New Jersey in 1933.
Although natural infections with these viruses occur following bites from mosquitoes and no human-to-human transmission occurs, the viruses also are highly infectious by aerosol. Alphaviruses replicate readily to very high titers and are relatively stable. These viruses could be replicated either in a wet or dried form inexpensively in large amounts. They once were used as model systems by which to study different aspects of viral replication genesis and vector relationships. These characteristics and the familiarity of the virus lend it to weaponization. The intentional release as a small-particle aerosol may be expected to infect a high percentage of individuals within an area of at least 10,000 km. The virus could also be purposefully spread by infected mosquitoes.
Pathophysiology
Susceptibility to viral encephalitides in humans is 90-100%, and virtually 100% of those infected will become ill.
After exposure to these viruses, the tissues of the CNS and reticuloendothelial and/or lymphoid systems most commonly are affected in both humans and animals. An acute incapacitating systemic viral febrile syndrome characterizes most infections. The severity of response is highly dependent upon host and viral factors, including the species and immune response of the host, route of infection, and strain and dose of the virus. VEE virus has the capacity to produce large human epidemics. Outcomes are significantly worse for young and elderly patients
Clinical manifestations – Venezuelan equine encephalitis
After an incubation period of 2-6 days, patients with VEE develop sudden fevers, chills, headache, malaise, myalgias, sore throat, and photophobia. CNS manifestations range from mild confusion and lethargy to seizures, paralysis, and coma. Hospitalization is required for 10% of patients; 4% of children and 1% of adults demonstrate severe CNS infection with a 35% mortality rate for children and a 10% mortality rate for adults. For those that survive, CNS recovery usually is complete.
Clinical manifestations – eastern equine encephalitis
The incubation period for EEE varies from 5-15 days. Adults may exhibit a viral prodrome of up to 11 days before the onset of CNS manifestations. Signs and symptoms include fever, chills, vomiting, muscle rigidity, lethargy, paresis, excess salivation, and impaired respiratory regulation. Children frequently develop facial and periorbital edema. CNS effects range from mild confusion to seizures and paralysis. As many as 30% of survivors of severe disease have permanent neurologic sequelae, which include seizures and various degrees of dementia.
Clinical manifestations – western equine encephalitis
WEE has an incubation period of 5-10 days. Most patients are asymptomatic or have a nonspecific febrile illness/aseptic meningitis picture. Manifestations include fever, nausea, vomiting, malaise, headache, nuchal rigidity, and lethargy. The severity of CNS involvement is inversely proportional to age. Up to 90% of patients younger than 1 year exhibit seizure activity. Typically, adults recover completely. Children have a higher incidence of persistent neurologic sequelae, which ranges from 50% in newborns to 1% in those older than 1 year.
Diagnosis
With all three of these viruses, laboratory evaluation may reveal leukopenia. CSF analysis demonstrates from 10 to thousands of white blood cells per microliter with a lymphocyte pleocytosis. Specific diagnosis depends on virus isolation, serology, or both. Virus may be collected from the nasopharynx for 3 days after the onset of symptoms. Serology tests available include IgM, ELISA, indirect FA, hemagglutination inhibition, compliment fixation, and IgG. PCR is not uniformly available. CSF is also suitable for most of these tests.
Treatment
No specific treatment is available for the viral encephalitides. Supportive care may include aggressive airway management and antipyretic and anticonvulsant drug administration. Patient isolation is not routinely necessary once the diagnosis is confirmed.
Prophylaxis
TC-83 is a live-attenuated IND vaccine for VEE. It is administered as 0.5-mL subcutaneous injection for those at high risk, such as laboratory field personnel. Approximately 20% of those who receive the vaccine fail to make a minimum neutralizing antibody response. An additional 20-25% of those vaccinated develop high fever, chills, and malaise that requires bed rest. C-84 is an inactivated vaccine developed for those with incomplete inactivation from the TC-83 vaccine. It produces only mild tenderness at the injection site. It is given in a 0.5-mL subcutaneous injection, administered at 2- and 4-week intervals until a satisfactory antibody response is measured.
The EEE vaccine is inactivated and administered in a 0.5-mL subcutaneous injection on days 0 and 28. Minimal side effects are noted, and no long-term problems have occurred. Boosters are required to maintain neutralizing titers.
Like the EEE vaccine, the VEE vaccine is inactivated, produces no adverse effects, and requires boosters. The vaccine is administered on days 0, 7, and 28.
Viral Hemorrhagic Fevers
Viral hemorrhagic fevers are caused by the following four families of viruses:
-
Arenaviridae (Lassa, Argentine, Bolivian, Brazilian, Venezuelan hemorrhagic fevers)
-
Bunyaviridae (Rift Valley, Crimean-Congo, Hantavirus)
-
Filoviridae (Marburg, Ebola hemorrhagic fevers)
-
Flaviviridae ( yellow fever, dengue, Kyasanur Forest, Omsk hemorrhagic fevers)
The best known of the viral hemorrhagic fever agents is Ebola virus. First recognized in Zaire in 1976, the virus has been linked to multiple outbreaks in Africa and is associated with a 53-92% mortality rate. A related virus was discovered in Reston, VA, in 1989 in association with an outbreak of illness among cynomolgus monkeys imported from the Philippines. No human cases occurred with this latter outbreak. The natural reservoir of Ebola is not known.
More than 200,000 cases of Lassa fever occur each year in Africa with more than 5000 deaths.
Filoviridae are spread from human to human by infected blood, secretions, organs, or semen. Congo-Crimean hemorrhagic fever is tick-borne but also may be spread by body fluid or the meat of infected animals. Hantavirus is rodent-borne, while Rift Valley fever and yellow fever are spread by mosquitos.
These viruses each are characterized by an acute generalized febrile illness that includes malaise, prostration, increased vascular permeability, and abnormalities of circulatory regulation. All agents are highly infectious via the aerosol route, most are stable as respiratory aerosols, and they can be replicated in cell culture. Thus, they possess characteristics ideal for use by terrorists.
Pathophysiology
The agents that produce viral hemorrhagic fever are all simple RNA viruses with lipid envelopes. They are stable at a neutral pH and able to survive in blood for long periods, which leads to their infectivity of patients around domestic animal slaughters. These viruses are linked to the ecology of their vector, whether rodent or arthropod, which helps in searching for a diagnosis. All of these viral agents are laboratory infectious hazards by aerosol.
The specific viral hemorrhagic fever syndrome that develops in patients depends on numerous factors such as viral virulence and strain characteristic, routes of exposure, dose, and host factors. Mortality is as follows:
-
Arenaviridae: 15-38%
-
Bunyaviridae: 1-50%
-
Filoviridae: 0.5-92%
-
Flaviviridae: 0.2-50%
Clinical manifestations
All viral hemorrhagic fevers primarily target vascular beds. They produce microvascular damage and enhance vascular permeability. Clinical manifestations can be diverse and include fever, myalgia, headache, prostration, conjunctival injection, mild hypotension to severe shock, and mucosal and petechial hemorrhages. Neurologic, hematopoietic, hepatic, and pulmonary involvement can be found with more severe disease.
Among the arenaviruses, Lassa fever is not associated with hemorrhagic or neurologic manifestations, but deafness is common. It causes the most severe capillary leak syndrome among hemorrhagic fever viruses and causes massive edema. Argentine and Bolivian hemorrhagic fevers have much more pronounced hemorrhagic and neurologic manifestations. Bolivian hemorrhagic fever is shown below.
 New World Arenavirus - Machupo. Oral mucosal hyperemia and hemorrhage in a patient with Bolivian hemorrhagic fever.
New World Arenavirus - Machupo. Oral mucosal hyperemia and hemorrhage in a patient with Bolivian hemorrhagic fever.
Rift Valley fever virus is primarily hepatotropic; hemorrhage occurs in only a small portion of patients. Crimean-Congo virus commonly is associated with severe DIC and the most severe hemorrhaging among the viral hemorrhagic fevers. Hantavirus is associated with pulmonary failure and acute kidney injury. A sunburn flush on the head, neck, and upper back is somewhat characteristic.
Limited clinical data are available for Ebola hemorrhagic fever; however, a nonpruritic, centripetal, pinhead-sized maculopapular erythematous exanthem (visible primarily in fair-skinned patients), bleeding and DIC are prominent manifestations of illness.
Of the flaviviruses, yellow fever virus is primarily hepatotropic. Black vomit caused by hematemesis is common, and patients usually develop clinical jaundice and die from hepatorenal syndrome.
Diagnosis
A high index of suspicion and detailed travel history are the most important steps in making the diagnosis of viral hemorrhagic fever. These agents are linked tightly with their natural geographic area and ecology of the reservoir species and vectors. Patients often recall exposures to rodents (Arenavirus, Hantavirus), mosquitoes (Rift Valley fever virus, yellow and dengue fever viruses), or even slaughtered horses (Rift Valley fever virus, Crimean-Congo virus). Suspect viral hemorrhagic fever in patients with fever, diffuse mucosal and dermal bleeding, and known travel to an endemic area for the illness.
Laboratory tests may be helpful. Leukopenia and thrombocytopenia are common, except in Lassa fever and Hantavirus. Proteinuria and hematuria are both common, but their absence rules out Hantavirus and Argentine and Bolivian hemorrhagic fevers.
Definitive diagnosis requires specific virologic diagnosis. ELISA can detect early immunoglobulin antibody responses during the acute illness; however, results may take 3-10 days. Reverse transcriptase PCR also may be used to identify a specific RNA virus. Testing can be conducted at the CDC in Atlanta or the US Army Medical Research Institute of Infectious Disease in Frederick, Maryland.
Treatment
Treatment of a viral hemorrhagic fever is largely supportive. Patients benefit from rapid nontraumatic hospitalization to prevent damage to the capillary bed. Air transport is contraindicated. Sedative and pain-relieving medications are helpful, but aspirin and other antiplatelet agents should be avoided.
Avoid intravenous lines and catheters unless absolutely necessary. Secondary infections should be sought and aggressively treated.
Immunosuppressive agents such as steroids are contraindicated. The treatment of bleeding is controversial. Generally, mild bleeding should not be treated, whereas severe hemorrhage requires appropriate replacement therapy. Fluid infusions are typically safe for severe volume depletion except in the setting of pulmonary edema.
Specific treatment with ribavirin has been used and currently is being investigated as therapy for Lassa fever, Hantavirus, Argentine hemorrhagic fever, Crimean-Congo, and Rift Valley Fever. Investigational treatment IND oral and IV protocols for ribavirin are available from the CDC and Department of Defense (USAMRIID). Treatment is most effective if begun within 7 days. Ribavirin has poor activity against the filoviruses and flaviviruses.
Prevention and prophylaxis
The only established and FDA-licensed virus-specific vaccine against any of the VHF viruses is the 17D live-attenuated yellow fever vaccine. It is mandatory for those traveling into endemic areas of Africa and South America. Current trials are underway for other vaccines and antibody therapies.
Strict adherence to barrier precautions (gloves, gown, eye protection, and face mask) and careful handling of infectious material and needles is needed to prevent nosocomial transmission. Patients should be placed in negative pressure rooms with 6-12 air exchanges per hour to decrease or prevent aerosol transmission of virus. All patient waste and linen should be incinerated or autoclaved.
Survivors should avoid sexual contact for 3 months. Corpses should be promptly sealed and buried or cremated.
Biological Toxins
Staphylococcal Enterotoxin B
Staphylococcal enterotoxin B (SEB) is one of the best-studied and, therefore, best-understood toxins. Staphylococcal enterotoxin is one of the most common causes of food poisoning. Nausea, vomiting, and diarrhea normally occur following ingestion of contaminated foodstuffs. The toxin causes a markedly different clinical syndrome when exposure is through a nonenteric route.
In a BW or terrorist situation, the toxin is likely to be acquired through inhalation of an SEB aerosol. SEB is stable as an aerosol, and the inhaled dose necessary to incapacitate individuals is small (0.004 mcg/kg). Within 24 hours of inhalation of SEB toxin, exposed individuals are likely to be incapacitated by systemic illness created by the toxin. SEB could also be used to contaminate food or small-volume water supplies.
Pathophysiology
SEB is an extracellular product produced by coagulase-positive staphylococci. The toxin is heat stable and generally forms in the presence of overgrowth of staphylococcal organisms, as occurs with poorly handled food. The effects of the enterotoxin are mediated by its interactions with the host's own immune system. The toxin binds directly to the major histocompatibility complex and subsequently stimulates large numbers of T- lymphocytes. These activated T-lymphocytes then stimulate the release of various cytokines (eg, tumor necrosis factor, interleukin-1 and interleukin-2, interferon), which are thought to mediate the toxic effects of SEB.
Clinical manifestations
Signs and symptoms begin 2-12 hours after inhalation and 2-10 hours after ingestion. Mild-to-moderate inhalation exposure to SEB produces nonspecific systemic illness that is characterized by fever, chills, headache, nausea, vomiting, dyspnea, chest pain, myalgias, and a nonproductive cough. Severe exposures can lead to a toxic shock–like picture and even death. Oral exposure results in predominantly nausea, vomiting, and diarrhea, but fever, chills and myalgias may also be present. Ocular exposure may result in conjunctivitis.
In mild-to-moderate cases, the physical examination is typically unremarkable. In severe instances, rales are common from pulmonary edema. Depending on the severity of exposure, duration of illness varies from 3-10 days. Coughing may last up to 1 month.
Diagnosis
Diagnosis of SEB intoxication can be difficult and is made primarily using clinical and epidemiologic methods. Laboratory studies may show a nonspecific neutrophilic leukocytosis and an elevated erythrocyte sedimentation rate. In severe exposures with significant pulmonary symptoms, a chest radiograph may show interstitial edema.
Enterotoxin is a stable protein that can be collected from serum if performed quickly. However, by the time symptoms are noted, the detection of toxin is unlikely. SEB accumulates in urine and may be detected for several hours following exposure. If the source of infection is from an inhalation injury, the toxin may be isolated from nasal swabs for up to 12-24 hours.
Treatment
Supportive care is the mainstay of treatment. Close attention to oxygenation and hydration are important. Patients with severe SEB may need ventilator support and diuretics. Most patients are expected to do well after the initial phase, but the time to full recovery may be prolonged.
Prophylaxis
No approved human vaccine exists for SEB, although a vaccine is nearing advanced development and testing. Passive immunotherapy agents have demonstrated some promise when given within 4-8 hours of exposure in animal models, but such therapy is still investigational.
Ricin
Ricin, a plant protein toxin derived from the beans of the castor plant, is one of the most toxic and easily produced of the plant toxins. Although the lethal toxicity of ricin is approximately 1000-fold less than botulinum toxin, the worldwide ready availability of castor beans and the ease with which toxin can be produced give it significant potential as a biological weapon.
Since ancient times, more than 750 cases of ricin intoxication have been described. Ricin is thought to have been used in the assassination of Bulgarian exile Georgi Markov in London in 1978. He was attacked with an umbrella device that implanted a ricin-containing pellet into his thigh.
Pathophysiology
The toxicity of ricin varies greatly with the route of administration. Ricin is extremely toxic to cells and acts by inhibiting protein synthesis. Inhalation exposure causes primarily pulmonary symptoms, ingestion causes GI symptoms, and intramuscular exposure results in a localized reaction.
Clinical Manifestations
Following inhalation exposure of ricin, toxicity begins within 4-8 hours and is characterized by the sudden onset of nasal and throat congestion, nausea and vomiting, itching of the eyes, urticaria, and tightness in the chest, cough, and dyspnea. If exposure is significant, pulmonary manifestations occur after 12-24 hours and include airway lesions, alveolar flooding, and severe respiratory distress. In animal studies, death occurs 36-48 hours after severe exposure.
Ingestion of ricin is generally less toxic because of its poor absorption and enzymatic degradation in the digestive tract. Out of 751 ingestions recorded, only 14 resulted in a fatality. Clinical manifestations occur rapidly and are characterized by nausea, vomiting, abdominal pain and cramping, diarrhea, fever and chills, hematochezia, and eventually, shock and vascular collapse. Autopsy findings have revealed significant hepatic, splenic, and renal necrosis.
At low doses, intramuscular exposures produce flulike symptoms, myalgias, nausea, vomiting, and localized pain and swelling at the injection site. Severe intoxication results in local lymphoid necrosis and GI hemorrhage, as well as diffuse hepatic, splenic, and renal necrosis.
Diagnosis
The diagnosis of ricin poisoning is made on the basis of clinical and epidemiologic factors. In a BW or terrorist situation, exposure is likely to occur by inhalation of a toxin aerosol. Thus, consider ricin poisoning when patients experience upper airway and pulmonary symptoms in the setting of a known or suspected mass casualty incident.
Patients may have neutrophilic leukocytosis, hypoxemia, and bilateral infiltrates on chest radiograph. Confirmation of ricin exposure can be made by ELISA analysis of a swab sample from nasal mucosa or from serum. Ricin can be identified for up to 24 hours after exposure. PCR can detect castor bean DNA.
Treatment
Treatment is supportive. Determine specific treatment largely by the route of exposure and clinical manifestations. Inhalation injury may require treatment of pulmonary edema, with respiratory support as indicated. Early after ingestion, patients should undergo GI decontamination with gastric lavage and the administration of activated charcoal. Intravenous crystalloid infusion and pressor support may be necessary for patients with hypotension.
Prophylaxis
Currently, no vaccine is available for ricin exposure. Investigational vaccines have proved effective in animals. Some chemotherapeutic agents are being studied as well.
For patient education information, see the First Aid and Injuries Center, as well as Ricin.
Botulinum Toxin
The anaerobic, spore-forming, gram-positive bacillus Clostridium botulinum produces botulinum toxins. Botulinum toxins are the most lethal toxins known and depending on the subtype, are 10,000-100,000 times more toxic than chemical nerve agents. The estimated lethal dose to 50% of the exposed population (LD50) is 0.001 mcg/kg in humans.
Since botulinum toxin is so lethal and easy to manufacture and weaponize, it represents a credible threat as a BW agent. When used as a BW or terrorist agent, exposure is likely to occur following inhalation of aerosolized toxin or ingestion of food contaminated with the preformed toxin or microbial spores. Historically, Japan (1930s - 1940s), the US (1940s - 1960s) and the former Soviet Union (1950s - 1990s) all conducted research on using botulinum toxin as a weapon. US research led to the development of the first botulinum type A toxoid vaccine during World War II, and eventually to safe and effective therapeutic uses for botulinum toxin type A. [32] . Iraq admitted to active research on offensive use of botulinum toxins and to weaponizing and deploying more than 100 munitions with botulinum toxin in 1995. [9]
Pathophysiology
All seven subtypes (A-G) of botulinum toxin act by similar mechanisms. The toxin produces similar effects whether ingested or inhaled. The time course and severity of illness vary with route of exposure and dose received. Symptom onset is slower after inhalation exposure.
Botulinum toxins bind to the presynaptic nerve terminal at the neuromuscular junction and cholinergic autonomic sites. This prevents the presynaptic release of acetylcholine and blocks neurotransmission. Interruption of neurotransmission produces muscular weakness and paralysis. Recovery requires months as the neurons develop new axons.
Clinical manifestations
Symptom onset may occur hours to several days after inhalation exposure (usually from 12-36 h). Initial signs and symptoms include blurred vision, mydriasis (in 50% of cases), ptosis, dysphagia, dysarthria, dysphonia, and muscle weakness. Anticholinergic signs and symptoms, such as dry mouth, urinary retention, ileus, and constipation, are seen.
After 24-48 hours, neuromuscular manifestations progress to symmetric descending paralysis and respiratory failure. Varying degrees of muscular weakness may occur. Patients may become cyanotic or exhibit narcosis from carbon dioxide retention secondary to respiratory failure. Postural hypotension may occur from autonomic insufficiency. Deep tendon reflexes may be depressed or absent on physical examination. Cranial nerve palsies often are present. Sensory symptoms do not occur, and CNS symptoms are not seen until respiratory failure is present (due to CO2 narcosis and/or hypoxia).
Diagnosis
The occurrence of multiple related cases of descending and progressive bulbar and skeletal paralysis in afebrile patients should suggest the diagnosis of botulinum toxicity. Laboratory tests, including CSF studies, generally are not helpful. Oral exposure can be detected by analyzing serum or gastric contents with a mouse neutralization assay. Intoxication by inhalation can be diagnosed using ELISA identification from nasal swabs up to 24 hours after exposure.
The differential diagnosis includes the following:
-
Stroke
-
Myopathy
-
Viral syndromes
-
Psychiatric illnesses
Treatment
The most serious complication of toxicity is respiratory failure. With supportive care and ventilatory assistance, fatalities should be less than 5%. Complete recovery may take up to a year.
For confirmed exposures, a heptavalent equine antitoxin (types A-G) is available from the CDC [33] . The antitoxin does not reverse the signs and symptoms already present but neutralizes circulating toxin to prevent further progression. This antitoxin has all the disadvantages of horse serum products, including the risks of anaphylaxis and serum sickness. Skin testing is performed by injecting 0.1 mL of a 1:10 dilution of antitoxin intradermally and monitoring the patient for 20 minutes. After a negative skin test, administer the antitoxin at a dose of 10 mL IV over 20 minutes, which is repeated until improvement ceases. With a positive skin test, administer 0.01-0.1 mL of antitoxin subcutaneously, gradually increasing the dose every 20 minutes until 2 mL can be sustained without reaction.
A bivalent human antitoxin (types A and B; BabyBIG) is FDA approved and available from the California Infant Botulism Treatment and Prevention Program for treating infant botulism.
Prophylaxis
A Botulinum Heptavalent Antitoxin (equine) (HBAT) toxoid for C botulinum (types A-G) is available through the CDC [33] .
Mycotoxins
The trichothecene mycotoxins are highly toxic compounds produced by certain species of filamentous fungi (Fusarium, Myrotecium, Cephalosporium, Trichoderma, Verticimonosporium, Stachybotrys species). These mycotoxins (eg, T-2, nivalenol) cause multiple organ effects, which include emesis, diarrhea, weight loss, nervous disorders, cardiovascular alterations, immunosuppression, hemostatic derangements, skin toxicity, and bone marrow damage.
Because of their antipersonnel properties, ease of large-scale production, and amenability to dispersal by various methods (dusts, droplets, aerosols, smoke, rockets, artillery mines, portable sprays), mycotoxins have an excellent potential for weaponization. Trichothecenes ("yellow rain") have been used as a BW agent in Southwest Asia and Afghanistan. [34]
Pathophysiology
These toxins are nonvolatile, low-molecular-weight compounds that are highly soluble in acetone, ethyl acetate, chloroform, ethanol, methanol, and propylene glycol. The trichothecenes vaporize when heated in organic solvents. Extraction of the mycotoxin from fungal cultures yields a yellow-brown liquid that evaporates into a yellow crystalline product (thus, the "yellow rain" appearance). These toxins require a 3-5% sodium hydroxide solution and heating at 900°F for 10 minutes or 500°F for 30 minutes for complete inactivation.
The trichothecene mycotoxins are cytotoxic to most eukaryotic cells by way of inhibiting protein synthesis and electron transport. Rapid absorption from the gut or pulmonary mucosa can produce initial symptoms in 5 minutes and maximal effects by 60 minutes. Peak tissue levels occur 1-4 hours following exposure. These toxins are absorbed slowly through intact skin.
Clinical manifestations
After exposure to the mycotoxins, early symptoms begin within minutes. Cutaneous manifestations include burning, tender erythema, edema, and blistering with progression to dermal necrosis and sloughing of large skin areas in lethal cases. Respiratory exposure results in nasal itching, pain, sneezing, epistaxis, rhinorrhea, dyspnea, wheezing, cough, and blood-tinged saliva and sputum. The images below show vesicles on a hairless guinea pig after exposure to mycotoxin.
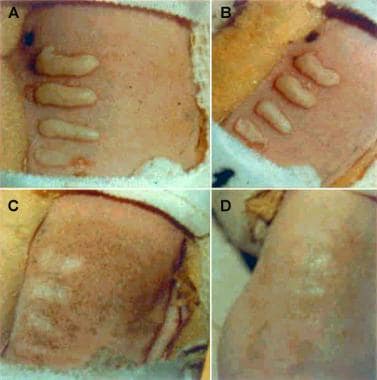 Vesicles and erosions on the back of hairless guinea pigs at (a) 1 day, (b) 2 days, (c) 7 days, and (d) 14 days after application of (bottom to top) 25 ng, 50 ng, 100 ng, or 200 ng of T-2 mycotoxin in 2 mcL of methanol. Reprinted from Wannamacher RW Jr, Wiener SL. Trichothecene mycotoxins. In: Zajtchuk R, Bellamy RF, eds. Medical Aspects of Chemical and Biological Warfare - Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997: 666.
Vesicles and erosions on the back of hairless guinea pigs at (a) 1 day, (b) 2 days, (c) 7 days, and (d) 14 days after application of (bottom to top) 25 ng, 50 ng, 100 ng, or 200 ng of T-2 mycotoxin in 2 mcL of methanol. Reprinted from Wannamacher RW Jr, Wiener SL. Trichothecene mycotoxins. In: Zajtchuk R, Bellamy RF, eds. Medical Aspects of Chemical and Biological Warfare - Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997: 666.
GI toxicity consists of anorexia, nausea and vomiting, abdominal cramping, and watery and/or bloody diarrhea. Entry into the eyes results in pain, tearing, redness, and blurred vision. Systemic toxicity may occur and includes weakness, prostration, dizziness, ataxia, tachycardia, hyperthermia or hypothermia, diffuse bleeding, and hypotension. Death may occur within minutes to days depending on the dose and route of exposure.
Diagnosis
Diagnosis of an attack of trichothecene mycotoxin depends on clinical observations and identification of the toxin from biological and environmental samples. Many patients presenting with the above symptoms and reporting a yellow rain or smoke attack lend support to the diagnosis. Initial laboratory studies are nonspecific. Elevations of serum creatinine, potassium, and phosphorus may occur, as well as abnormalities of coagulation parameters. An initial rise in absolute neutrophils can be observed. Leukopenia, thrombocytopenia, and anemia may occur 2-4 weeks following initial exposure.
Currently, a rapid identification kit for any of the trichothecene mycotoxins does not exist. Gas-liquid chromatography has been used in the past with great success. Serum, urine, and stomach contents can be tested at a reference laboratory.
Treatment
Treatment is supportive. The immediate use of protective clothing and masks during a mycotoxin aerosol attack should prevent illness. If a soldier is unprotected during an attack, the outer clothing should be removed within 4-6 hours and decontaminated with a solution of 1% sodium hypochlorite plus 0.1M sodium hydroxide for at least 1 hour. The skin should be washed with copious amounts of soap and uncontaminated water. The eyes, if exposed, should be irrigated with copious amounts of normal saline or sterile water. A skin decontamination kit (M291) currently is fielded to all US military personnel and is efficacious against most chemical warfare agents, including the mycotoxins.
No specific therapy exists for a trichothecene exposure. After appropriate skin decontamination, give victims of inhalation and oral exposures superactivated charcoal orally. Activated charcoal binds mycotoxins. Treat severe respiratory distress with endotracheal intubation and mechanical ventilation as needed. Early use of systemic steroids increases survival time by decreasing the primary injury and shocklike state that follows significant poisoning.
Prevention and prophylaxis
No vaccine exists for trichothecene mycotoxin exposure.
Available only to the US Department of Defense and many NATO military forces is the Reactive Skin Decontamination Lotion (RSDL). The proposed mechanism of action is neutralization of traditional chemical warfare agents by a combination of physical removal and nucleophilic breakdown, which renders the original toxic substance nontoxic. [22]
Physical barrier protection of the skin, mucous membranes, and airway provided by use of HAZMAT suits or chemical protective mask and clothing, such as MOPP gear, are the only effective methods of protection. The Skin Exposure Reduction Paste Against Chemical Warfare Agents (SERPACWA) has been shown to block dermal irritation in animal studies and can be applied at closure points of protective garments as well as to any exposed skin. It is FDA-approved for use in conjunction with Mission Oriented Protective Posture (MOPP) gear to reduce or delay the absorption of chemical warfare agents through the skin when SERPACWA is applied prior to exposure. [22]
-
The "eight ball" 1 million liter test sphere at Fort Detrick, Maryland. This aerobiology chamber was used before 1969 when the United States was performing offensive biological warfare research. Animals were tethered within the sphere while aerosolized agents were aerosolized.
-
Front of main building at the United States Army Medical Research Institute of Infectious Diseases (USAMRIID) on the grounds of Fort Detrick, Maryland.
-
Vesicles and erosions on the back of hairless guinea pigs at (a) 1 day, (b) 2 days, (c) 7 days, and (d) 14 days after application of (bottom to top) 25 ng, 50 ng, 100 ng, or 200 ng of T-2 mycotoxin in 2 mcL of methanol. Reprinted from Wannamacher RW Jr, Wiener SL. Trichothecene mycotoxins. In: Zajtchuk R, Bellamy RF, eds. Medical Aspects of Chemical and Biological Warfare - Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997: 666.
-
Adult with variola major with hundreds of pustular lesions distributed centrifugally. Photo courtesy of Fitzsimons Army Medical Center Slide File.
-
New World Arenavirus - Machupo. Oral mucosal hyperemia and hemorrhage in a patient with Bolivian hemorrhagic fever.
-
Typical heaped up ulcer of tularemia. Reprinted from Evans ME, Friedlander AM. Tularemia. Chapter 24. In: Sidell FR, Takafuji ET, Franz DR, eds. Medical Aspects of Chemical and Biological Warfare. In: Zajtchuck R, Bellamy RF, eds. Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997:505.
-
Ulceroglandular tularemia on the face. Courtesy of Dr Hon Pak.
-
Ulceroglandular tularemia on an extremity. Courtesy of Dr Hon Pak.
-
Ulceroglandular type of tularemia on the hand. Courtesy of Dr Hon Pak.
-
Characteristic skin lesion of variola viral infection on the arms and the legs of an adolescent. Photo used with the permission of the World Health Organization (WHO).
-
Small child with pustular lesions due to variola viral infection. Photo used with the permission of the World Health Organization (WHO).
-
Infant with advanced lesions due to variola viral infection. Photo used with the permission of the World Health Organization (WHO).
-
Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 3 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
-
Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 5 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
-
Unvaccinated infant with the ordinary form of the variola major strain of smallpox has centrifugally distributed umbilicated pustules on day 7 in the course of the disease. Reprinted with permission from the World Health Organization (WHO).
-
The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
-
The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
-
The ordinary form of the variola minor strain of smallpox (alastrim) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are sparser and evolved more rapidly than the extremity lesions. Reprinted with permission from the World Health Organization (WHO).
-
Hemorrhagic-type variola major lesions. Death usually ensued before typical pustules developed. Reprinted with permission from the World Health Organization (WHO). 1988; 10-14, 35-36.



