Background
The lips are the focal point of the face during social interactions. The lips are composed of skin, muscle, and mucosa, and they lack direct bony attachments or infrastructure. Hence, the lips are elastic and pliable; these characteristics are both advantages and disadvantages during surgical reconstruction.
The lips play many important roles and are particularly important in both verbal and nonverbal communication. They are necessary for articulation of the letters B, F, M, N, and V. [1] In addition, people use their lips to communicate a variety of feelings through facial expression. The lips serve important functions in eating and imbibition. The competence of the oral sphincter is important during chewing and sucking through a straw.
Because the lips are vital for interpersonal relations, even the slightest asymmetry is easily detected and can cause devastating consequences for the patient. Therefore, maintaining the functional and cosmetic integrity of the lips during surgical reconstruction is of the utmost importance. [2]
Relevant Anatomy
The lips are divided into three main sections: cutaneous, vermilion, and mucosal. The upper cutaneous lip is bordered superiorly by the nasal sill and columella, laterally by the nasolabial fold, and inferiorly by the vermilion lip. The upper lip is composed of three cosmetic units: two lateral and one medial. The lateral units are bordered by the nasolabial groove laterally and by the philtral crests medially. The medial philtral subunit is composed of the two convex philtral crests and the central philtral groove. See the anatomic diagrams below.
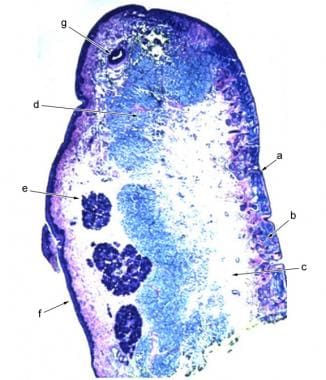 Histologic cross section of the lip showing the anatomic layers: epidermis of cutaneous lip (A), dermis of cutaneous lip (B), subcutaneous tissue of cutaneous lip (C), orbicularis oris muscle (D), lamina propria of mucosal lip with salivary glands (E), mucosa of mucosal lip (F), labial artery (G).
Histologic cross section of the lip showing the anatomic layers: epidermis of cutaneous lip (A), dermis of cutaneous lip (B), subcutaneous tissue of cutaneous lip (C), orbicularis oris muscle (D), lamina propria of mucosal lip with salivary glands (E), mucosa of mucosal lip (F), labial artery (G).
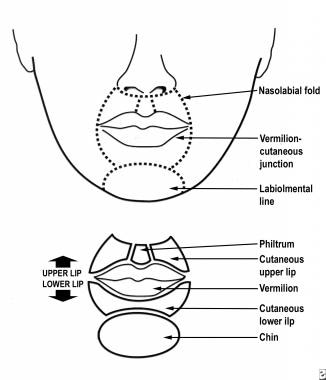
The Cupid's bow is the downward projection of the philtral unit, which gives the lip its characteristic appearance. The white roll is the light linear projection that circumferentially outlines the upper and lower lip at the border of the cutaneous and vermilion lip. Reconstruction of the Cupid's bow and the white roll is crucial in preserving the aesthetic nature of the lip; even slight alterations or misalignments of these areas are overtly noticeable.
The lower cutaneous lip is bordered superiorly by the lower vermilion lip; laterally by the extension of the nasolabial folds; and inferiorly by the mental crease, which separates the lower lip from the chin. This portion of the lip makes up 1 cosmetic unit. The relaxed skin tension lines emanate from the vermilion in a radial fashion and are perpendicular to the fibers of the orbicularis oris muscle.
The vermilion portion is the most cosmetically apparent portion of the lip. This portion is a modified mucosal membrane that lacks pilosebaceous units, eccrine glands, and salivary glands. The pink-to-red color of the vermilion lip is due to the extensive superficial vasculature in this area. The wet, or mucosal, lip abuts the teeth and contains minor salivary glands, which empty onto its surface. The red line is where the upper and lower lips meet, and this line corresponds to the transition zone between the vermilion lip and the mucosal lip. A recent study showed the ability of cutaneous keratinized epithelium transplanted into the oral cavity via skin grafts or flaps to transform over time and mimic the mucosa in both clinical appearance and histopathology. [3]
Knowledge of the cross-sectional anatomy of the lip is important to the dermatologic surgeon. Starting from the external surface, the layers are as follows: epidermis of the cutaneous lip, dermis of the cutaneous lip, subcutaneous tissue of the cutaneous lip, orbicularis oris, submucosal of the mucosal lip, and mucosa of the mucosal lip.
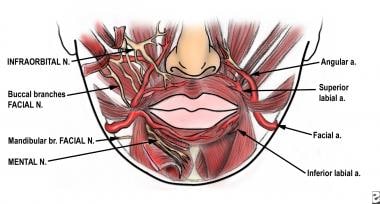
The arterial supply of the lips comes from the inferior and superior labial arteries, which branch off the facial artery at the oral commissures. The labial arteries can be found between the orbicularis oris and the submucosa deep to the vermilion-mucosal transition zone. Identifying the labial artery is critical for hemostasis during lip surgery. Variations in the arterial supply occur in the labiomental region, and surgeons should be aware of such variability. [4]
The sensory innervation of the upper lip is derived from branches of the trigeminal nerve (cranial nerve V). The upper lip is supplied by the infraorbital nerve, which exits the maxilla at the infraorbital foramen. Sensation in the lower lip is derived from the mental nerve, which exits the mandible at the mental foramen. The identification of these nerves is useful in performing nerve blocks for lip surgery. Motor innervation of the perioral muscles is supplied from the facial nerve (cranial nerve VII). The buccal branch of the facial nerve innervates the orbicularis oris muscle and the lip elevators. The marginal mandibular branch of the facial nerve innervates the orbicularis oris and lip depressors. This nerve is most susceptible to injury at the middle portion of the mandible, where it is most superficial.
The primary muscle of the lip is the circumferential orbicularis oris muscle. This muscle has no direct bony attachments, but rather, it is suspended from the surrounding muscles that attach into it. The orbicularis primarily acts as a sphincter, closing the mouth and keeping the lips closed. However, through complex movements, this muscle also functions in puckering, sucking, whistling, blowing, and creating facial expressions. The lip elevators are composed of the levator labii superioris alaeque nasi, levator labii superioris, zygomaticus major, zygomaticus minor, and levator anguli oris muscles. The upper lip retractors are the zygomaticus major, zygomaticus minor, and levator anguli oris muscles. The lip depressors are the depressor anguli oris and depressor labii inferioris muscles. The lower lip retractors are the depressor anguli oris and platysma muscles. The mentalis muscle causes the lower lip to protrude.
Contraindications
No absolute contraindications exist for this procedure.
-
Histologic cross section of the lip showing the anatomic layers: epidermis of cutaneous lip (A), dermis of cutaneous lip (B), subcutaneous tissue of cutaneous lip (C), orbicularis oris muscle (D), lamina propria of mucosal lip with salivary glands (E), mucosa of mucosal lip (F), labial artery (G).
-
Patient A. Primary repair of a Mohs surgical defect in the upper cutaneous lip. (The ruler is in centimeters.)
-
Patient A. Postoperative photograph. The primary repair is oriented in the relaxed skin tension lines. (The ruler is in centimeters.)
-
Patient A. The scar is almost invisible 2 months after primary repair. (The ruler is in centimeters.)
-
Patient B. Wedge excision of the lower lip. Full-thickness lip defect.
-
Patient B. Reapproximation of the orbicularis oris muscle.
-
Patient B. Reapproximation of the vermilion-cutaneous border.
-
Patient B. Result immediately after surgery.
-
Patient B. Appearance 3 months after surgery.
-
Patient C. Unilateral advancement flap used to repair a Mohs surgical defect.
-
Patient C. Photograph obtained immediately after surgery.
-
Patient C. Result 4 weeks after surgery.
-
Patient D. Bilateral advancement flap of the upper lip used to repair a Mohs surgical defect in the right upper cutaneous lip. (The ruler is in centimeters.)
-
Patient D. Appearance of the patient immediately after surgery. Note the placement of incision lines at the nasal sill and vermilion border. (The ruler is in centimeters.)
-
Patient D. Three months after surgery, only the vertical scar is noticeable. (The ruler is in centimeters.)
-
Patient E. Unilateral rotation flap used to repair a Mohs surgical defect on the right lateral upper cutaneous lip.
-
Patient E. Appearance of the rotation flap immediately after surgery. Note the placement of the major portion of the incision in the melolabial fold.
-
Patient E. Postoperative result 3 months after surgery.
-
Patient F. Bilateral rotation flap used to repair a large Mohs surgical defect on the medial cutaneous lip. (The ruler is in centimeters.)
-
Patient F. Bilateral rotation flaps were used to close the defect. (The ruler is in centimeters.)
-
Patient F. Postoperative result at 1 month after surgery. (The ruler is in centimeters.)
-
Patient G. Transposition flap used to repair a Mohs surgical defect on the lateral upper cutaneous lip. (The ruler is in centimeters.)
-
Patient G. A superiorly based rhombic transposition flap was designed and sutured in place. (The ruler is in centimeters.)
-
Patient G. Postoperative result at 1 month after surgery. (The ruler is in centimeters.)
-
Anatomy of the lip region.
-
Cosmetic units of the lip.





