Overview
Excisional skin surgery involves the use of relatively superficial structures, is performed under local anesthesia, and seldom entails major blood loss or fluid shifts. That being said, it is still an invasive procedure, and a preoperative assessment of the patient is essential.
Anesthesia
Local anesthesia is used for simple excisions. A solution of lidocaine (0.5%, 1%, or 2%) with 1:100,000 epinephrine is typically injected by using a 0.5-inch-long 30-gauge needle. [1] No absolute contraindications to the use of lidocaine with epinephrine in cutaneous surgery exist. Such anesthetic preparations can be safely used even at distal terminal body sites, such as the fingertips and penis, provided that no tourniquet or equivalent device is used concurrently. Lidocaine is pregnancy category B and epinephrine is category C; however, in dermatologic surgery, the benefits of small quantities of epinephrine often outweigh the risks. [2]
The anesthetic may be delivered into the dermis or upper aspect of the subcutis. Intradermal injection results in blanching of the skin and increased follicular prominence. The person administering the injection can be confident that the needle tip is in the dermis when significant backpressure is felt and when force is required to maintain the forward flow of the anesthetic. Injections should be administered at a slow constant rate to minimize the patient's discomfort. Buffering the anesthetic by adding sodium bicarbonate (1 part per 9 parts lidocaine) can further enhance the patient's comfort by diminishing the associated acidic sting.
The entire surgical area plus a rim of several millimeters should be anesthetized. Preferably, the lesion to be excised should not be directly injected, especially if it is to be sent for pathologic examination. Rather, anesthetic should be delivered circumferentially toward the center. A so-called ring block may be particularly desirable in excising a cyst that may be ruptured by injecting into its belly. Areas that have not yet been anesthetized should be injected through already numb areas to protect the patient from the discomfort of repeated pinpricks.
Patients are often concerned about intraoperative pain. Painless injection of the anesthetic is reassuring to the patient and communicates that the surgeon is determined to make the procedure as pleasant as possible. This effect, in turn, encourages the patient to cooperate with the surgeon during the remainder of the process.
Simple excisions rarely require large quantities of anesthetic. However, during larger excisions on the trunk or during protracted procedures that require frequent reinjection, monitoring the amount used may be prudent. For 1% lidocaine, toxic doses are approximately 300 mg, or 30 mL, when used without epinephrine and 500 mg, or 50 mL, when used with epinephrine in a healthy adult patient weighing 150 lb (70 kg).
To maximize the patient's comfort, the level of anesthesia should be tested before an incision is made. This test can be completed by tapping the 30-gauge needle on the skin and asking the patient to report when he or she feels a sharp sensation. Tender areas may be injected with additional amounts of solution. The patient should be reassured that more anesthetic is available should it be needed later.
For more information, see Medscape articles Local and Regional Anesthesia and The Role of Antibiotics in Cutaneous Surgery.
Equipment
In the operating room, a sterile tray should be available for the surgery. At minimum, this tray should contain a scalpel handle, a No. 15 blade, an Adson serrated forceps, 2 skin hooks, a Gradle or other appropriate scissors for cutting tissue, scissors for cutting sutures, a needle holder, suture material, many cotton-tipped applicators, gauze, and cloth towels for draping the patient. A No. 10 blade is a broader, sturdier blade that is often used when performing cutaneous surgery on the back. Antiseptic solution and anesthetic may be included on the tray, or it may be applied before the tray is opened.
Suture materials
Often, both deep or buried (subcutaneous or dermal) and superficial or skin (dermal and epidermal) sutures are placed. In multilayered closures, the deep sutures bear virtually all of the tension, and the superficial sutures approximate the epidermal edges for an optimal, cosmetically acceptable result.
Various suture materials are available. The selection of specific materials is based on the surgeon's preference. Deep sutures that are commonly used include polydioxanone (PDS), Monocryl, and Vicryl, of which the first 2 are monofilaments (single, nonbraided strands). Each of these sutures is absorbable and do not need to be removed. Monofilaments are less prone to harbor infectious organisms, and synthetic sutures are less immunoreactive. Frequently used skin sutures are nonbraided synthetic nylon (eg, Ethilon) and polypropylene (eg, Prolene). These do need to be taken out.
On the face, cutaneous sutures may be removed after 5-7 days. On the trunk and extremities, they may be removed after 10-14 days. Prolonged placement of superficial sutures can result in reepithelialization over the sutures, as well as the formation of unsightly permanent track marks along the external path of the sutures. If reinforcement is required after the superficial sutures are removed, Steri-Strips may be applied.
Sutures are available in various thicknesses that are suitable for different body sites and tissues. Usually, 6-0 superficial sutures are used on the face, and 5-0 or 4-0 sutures are used on the trunk and extremities. Deep sutures are often of slightly greater caliber than the corresponding skin sutures. Facial excisions are routinely closed with 5-0 deep sutures, and 4-0 deep sutures may be required on other body sites. Large excisions on the back or scalp may require the use of 3-0 subcutaneous sutures.
Surgeons should choose the smallest suture that allows the wound edges to be apposed without cutting into the tissues. Larger-than-necessary sutures do not add to wound strength but do increase the burden of foreign material in the skin. Some experts believe that the placement of deep sutures improves the cosmesis of low-tension wounds [3] yet adds little to high-tension wounds. For instance, in high-tension skin on the trunk or scalp, closure with only skin sutures may provide a final result as attractive as that with a multilayered closure.
Absorbable materials, such as chromic catgut, can be used if removal of the skin sutures is not practical. Along the mucosa or close to the eyes, silk sutures, which are associated with a higher risk of immunogenicity and infection, may be more comfortable.
Tissue adhesives
Tissue adhesives, usually cyanoacrylate compounds, are another option for wound closure, especially in areas of low tension. Advantages include faster closure time compared with sutures and lack of track marks. Disadvantages include cost and possible higher rate of dehiscence, especially in areas under tension. Cosmetic outcomes and wound infection rates mirror those of sutures. [4, 5]
For more information, see Medscape article Materials for Wound Closure.
Technique
Preoperative preparation
The patient's past medical history should be elicited and documented in all cases. Conditions that may interfere with wound healing (eg, collagen vascular diseases, smoking, diabetes) and the use of concurrent medications that may increase the likelihood of intraoperative bleeding (eg, aspirin, other nonsteroidal anti-inflammatory drugs, oral vitamin E, warfarin) are of particular interest. Major medical problems, such as cerebrovascular, cardiovascular, or respiratory disease, should be investigated further, even if they seem to be stable. The internist or other physician who is managing these important conditions may be consulted if the surgeon judges it necessary. The planned excisional surgery should be explained to the physician, and his or her opinion regarding the feasibility of the procedure can be obtained in writing and placed in the patient's chart.
Aspirin, warfarin (Coumadin), and other agents prescribed for the modification of bleeding time or platelet function must not be discontinued without the expressed permission of the physician prescribing them. Catastrophic complications, including widespread pulmonary embolus, stroke, and clotting of artificial heart valves, may occur when medically necessary anticoagulation is terminated perioperatively. [6] Intraoperative and postoperative complications are minimal even when warfarin is continued during the surgical period. [7]
Patients who are able to undergo surgery but who are in frail health may require intraoperative cardiac monitoring. Exceptionally sick patients may be best operated on in a hospital clinic setting, where specialized emergency services are available. Prophylactic oral antibiotics may be initiated if indicated by preexisting conditions (eg, valvular disease, rheumatic heart disease) or if the operation is prolonged or complex.
A focused physical examination should be performed prior to excisional surgery. The presumptive diagnosis and the appropriateness of the operation should be confirmed. The surgeon is responsible for ensuring that the procedure is feasible.
Prior to commencing with the operation, the surgeon should clean the surgical site with an antiseptic solution such as chlorhexidine gluconate (Hibiclens) or povidone-iodine (Betadine). The impregnated swab or gauze should be firmly moved in one direction along the skin in a spiral motion, from the center to the periphery. No areas should be missed, and the cleansed area should extend well beyond the surgical site.
For more information, see Medscape Reference article Preoperative Evaluation and Management.
Planning the elliptical, or fusiform, excision [8, 9]
The elliptical, or fusiform, excision is the classic approach to removing an approximately round or linear lesion. [10, 11] An excision of this shape is preferred because of the subsequent ease of its closure. A round excision larger than a 4-mm punch is difficult to close without leaving excess outpouchings of skin or dog ears.
The ellipse should be long enough so it can be sutured together without dog ears but no longer than necessary to minimize the length of the inevitable scar. The process begins by marking the lesion to be removed. A permanent marker or other skin marker may be used to circle the target lesion. Often, a free margin of several millimeters must be removed from around the primary lesion, and the mark for this margin can be drawn as a larger concentric circle. Then, an ellipse should be marked around the larger circle. The diameter of the circle should form the short axis of the ellipse, and the longer axis should be 3-4 times this length. Alternatively, the angle between 2 lines drawn from an edge of the long axis to the bilateral midpoint edges of the ellipse should be about 30° (see image below).
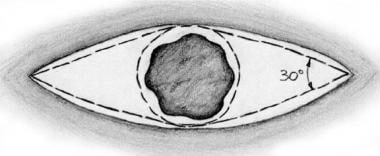 In the classic elliptical or fusiform excision, the edges are at an internal angle of 30°. Although this angle defines the relationship of the edge to the central lesion being removed, the actual cutting angle at the edge is typically broader, as demonstrated in the image.
In the classic elliptical or fusiform excision, the edges are at an internal angle of 30°. Although this angle defines the relationship of the edge to the central lesion being removed, the actual cutting angle at the edge is typically broader, as demonstrated in the image.
The orientation of the ellipse is important. Ideally, the long axis should lie parallel to the relaxed skin tension lines at the body site involved. Diagrams that display the common skin tension lines on the face and body are available (see image below). The precise inclination of these lines can be confirmed by having the patient engage in a variety of exaggerated facial expressions. On the arms and legs, flexion and extension can substitute for such maneuvers. The surgeon can obtain this information at the surgical site by deliberately wrinkling the skin at the surgical site between his or her thumb and forefinger. By placing the ellipse along relaxed skin tension lines, the surgeon ensures that the final scar is parallel to these lines. If the scar is thin and small and if the patient is elderly, it may be barely noticeable, appearing as merely another wrinkle or crease to the untrained observer.
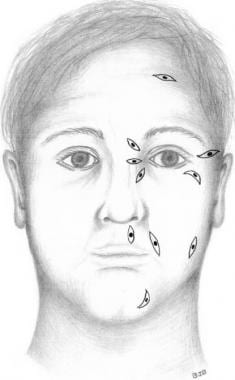 Ellipses should be oriented in the relaxed skin tension lines. If the ellipses are placed carefully, linear scars are minimally noticeable. The locations of the skin tension lines vary slightly among individuals; therefore, stylized diagrams do not provide sufficient guidance. Close examination and pinching of the skin reveals the orientation of the lines.
Ellipses should be oriented in the relaxed skin tension lines. If the ellipses are placed carefully, linear scars are minimally noticeable. The locations of the skin tension lines vary slightly among individuals; therefore, stylized diagrams do not provide sufficient guidance. Close examination and pinching of the skin reveals the orientation of the lines.
For more information, see Medscape articles Essentials of Tissue Movement and Facial Anatomy in Cutaneous Surgery.
Needle management
The suture needle should be clasped with a needle driver at a point two thirds the distance from the tip (see image below). Securing the needle at this point reduces the likelihood of bending or breaking it during surgery. Needle holders are typically held with the handles in the palm of the dominant hand. The index finger is placed immediately proximal and posterior to the jaws of the needle holder. In this orientation, the index finger can guide the path of the needle, and the palm can rotate the needle once it is in the skin. Notably, the surgeon does not need to place his or her fingers through the rings of the needle holder while suturing.
 The needle driver should be used to grasp the needle in the middle or slightly beyond the middle toward the insertion of the suture. Holding the needle too close to the end results in slippage and bending of the shaft.
The needle driver should be used to grasp the needle in the middle or slightly beyond the middle toward the insertion of the suture. Holding the needle too close to the end results in slippage and bending of the shaft.
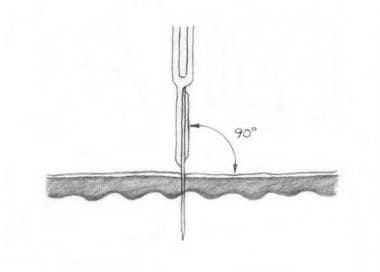
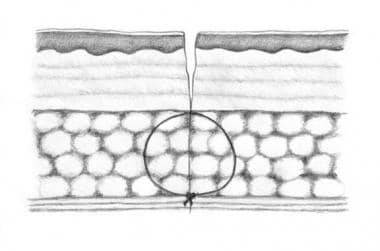
The needle is inserted perpendicular to the skin, that is, at a 90° angle (see image below). Proper entry requires some hyperpronation of the hand at the wrist. As the needle penetrates deeper, its movement becomes oblique and then lateral, until it emerges in the center of the wound. Then, the needle reenters the skin on the opposite site of the wound, with the direction of motion gradually shifting from lateral to oblique. Ultimately, the needle exits the skin on the contralateral side, again at a 90° angle. Sutures that enter and exit the skin at 90° angles and travel obliquely and then laterally under the skin are most effective for inducing eversion.
If tension along the wound is low, extracting the needle on the far side may be difficult. In this case, a forceps can be pressed flat against the far side of the wound, and the needle can be pushed through its tips. The tips can be used to pull out the needle, which should be rotated during this process to avoid bending it. The surgeon should never use his or her fingers to pull the needle because this action poses an unacceptably high risk of an inadvertent needle stick.
The surgeon should visually inspect the wound edge to ensure that it is everted and even.
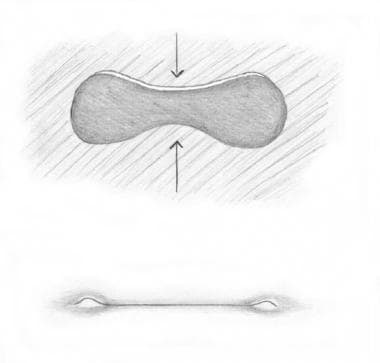
Eversion refers to the creation of a central ridge along the closure line. As the wound matures, spreading and contraction associated with normal healing flattens this elevation, leading to a flat scar. Evening of the skin edges is also necessary to ensure that the final contour is smooth. At times, one edge may be significantly lower than the other; this asymmetry may be corrected by inserting the needle deep on the low side and shallow on the high side. In this manner, the lower edge is elevated, and the higher one is depressed. The size of the 2 bites and their respective distances from the edge of the wound should remain roughly equivalent.
For more information, see Medscape article Closure of Complicated Wounds.
Cutting and undermining [12]
The surgeon should hold the scalpel between the thumb and forefinger of his or her dominant hand. The other hand is used to apply 3-point traction to stretch and immobilize the surgical site. An incision is commenced toward the direction of the operating surgeon with the anterior belly of the blade pressing against the previously marked ellipse. One firm, continuous stroke is applied to cut the epidermis and partly through the dermis on each side. The blade should be exactly perpendicular to the tissue (ie, at a 90° angle) during this process (see image below). Jerky, sawing, or repetitive motions result in nicked edges or fishtailing beyond the edge of the ellipse. On thick skin, such as that on the back and extremities, the initial incisions may not be adequate to achieve a cut of sufficient depth. In this case, the blade may be reintroduced into the previously incised grooves, and the motion is repeated as the blade presses against the outside margin.
 In general, the scalpel blade should be maintained perpendicular to the skin surface because vertically oriented cuts close most neatly and with the best eversion. The position of the hand may need to be modified when a topographically curved surface is incised.
In general, the scalpel blade should be maintained perpendicular to the skin surface because vertically oriented cuts close most neatly and with the best eversion. The position of the hand may need to be modified when a topographically curved surface is incised.
The depth of the excision depends on the type of lesion being excised and the anatomic location. Most excisions continue to the superficial, middle, or deep part of the subcutis. Once the ellipse that contains the lesion has been incised to the desired depth on all sides, the ellipse may be removed. Forceps with teeth or a skin hook may be used to gently grasp the tissue from one end. Then, a scalpel blade or scissors are used to undercut the tissue (see image below). If the tissue is held over the scalpel blade during the cutting process, the tissue is cut less deeply than if it were pulled away from the scalpel blade. After the fusiform piece of tissue is removed, an uneven layer of fatty tissue may remain at the site. This uneven layer should be carefully trimmed to create an even plane to ensure optimal even closure of the wound.
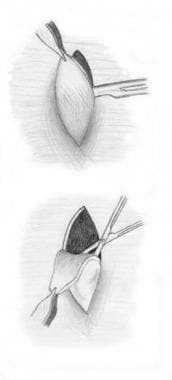 When freeing tissue with a scalpel, the surgeon can tug the skin laterally toward himself or herself to help ensure even depth. A pair of scissors easily stays in the correct plane and can be used to reflect the tissue ellipse upward.
When freeing tissue with a scalpel, the surgeon can tug the skin laterally toward himself or herself to help ensure even depth. A pair of scissors easily stays in the correct plane and can be used to reflect the tissue ellipse upward.
Undermining the area around the edges of the removal site can be helpful. Undermining decreases both the vertical and lateral tension on the final closure, improving the cosmesis of the result. When tension is not great or when the wound is small, undermining may not be necessary. Similarly, if the maintenance of hemostasis is a challenge, undermining may only exacerbate the problem.
The process of undermining is best performed by holding up the wound edges with a skin hook. Closed blunt-tipped scissors should be inserted into the tented space. When they are some distance inside, they should be opened. In this manner, tissues are not cut, but rather, pushed aside. Some experts advocate so-called sharp undermining; though this approach may provide a more even closure, it creates a substantial risk of nerve or vessel injury in the hands of the novice.
The depth of undermining ideally extends to the most superficial layer possible. Often, this level is the superficial fat. The lateral extent of the undermining should be sufficient to permit low-tension closure of the wound. Excessive undermining can result in the opposite problem of having too much tissue and creating dog ears that then must be removed.
Hemostasis
Blood may collect in the cavity left after ellipse removal, as a result of slow oozing or more rapid bleeding from a few point sources. Vessels may have been cut in the subcutis and along the dermal wound edge. Seldom are these vessels of large caliber, but even moderate bleeding should be controlled prior to closure. The development of hematomas and persistent bleeding after discharge can be prevented with this approach.
Electrocautery can be used to close vessels. Damage to adjacent nonbleeding tissue should be minimized during the procedure. Grasping the bleeding vessel with a fine forceps and touching the active electrode to the handle permits precise targeting for coagulation. The area at the cauterized site must be dry for the device to work optimally, and this dry field may be maintained by applying gauze, by rolling over it with a cotton-tipped applicator, or by using a suction apparatus (in rare instances).
The electrosurgical apparatus can also be used to directly touch the bleeding areas; however, in some cases, this approach may result in greater destruction of uninvolved surrounding tissue. In general, electrocoagulation should be sufficient but not excessive. Not every pinpoint bleeder needs to be treated, and the wound edge should be treated sparingly if at all. Overuse of the cautery device can devitalize tissue at the closure site, impeding healing and creating a reservoir of necrotic tissue that is vulnerable to superinfection. A small amount of oozing is permissible as an end point prior to closure.
Larger vessels can be tied off with sutures. The vessels may initially be grasped with a hemostat and then tied off with a small amount of adjacent tissue. Figure-eight closures are rarely necessary in cutaneous surgery. Similarly, absorbable gelatin sponges (Gelfoam) and similar hemostatic packing materials are required only in rare circumstances.
Suture technique
Before the sutures are placed, hooks or hand pressure can be used to simulate the final closure. This simulation demonstrates exactly the point on one side of the wound that should appose a given point on the contralateral side. The rule of halves suggests that the first suture should be placed in the middle of the wound, bisecting each half with additional sutures. The surgeon can proceed in this manner until the wound is sewed shut.
Alternatively, the surgeon may begin by placing stitches at one end of the wound and continuing to the other end. This technique is helpful when the wound is under substantial tension. Tension may also be relieved by placing 1 or 2 skin sutures near the center before the subcutaneous sutures are placed. Afterward, these temporary tension-relieving skin sutures can be removed. The distance between parallel sutures depends on the thickness of the skin and the anatomic site. When the dermis is thicker, sutures are farther apart and deeper. For all wounds, the tension peaks at the center of the ellipse, and sutures here may be placed closer together.
Most suture ties in excisional surgery are instrument ties rather than hand ties. The typical knot is the surgeon's knot square, which consists of placing 2 loops around the needle holder at 1 edge of the suture and then it pulling through to the other edge. Buried knots are tightened parallel to the closed incision (deep suture placement is shown in image below). Superficial knots are tightened perpendicular to the wound line, with the first knot minimally tightened and merely laid down on the skin. The use of multiple throws of the surgeon's knot is routine, but the use of more than 3 throws should be avoided with buried knots because the throws greatly increase the volume of foreign material implanted into the skin.
 Deep absorbable stitches should be placed so that the knot is facing downward. This placement reduces the likelihood that a spitting suture erupts to the surface. Deep stitches can be placed in either the subcutis, as shown here, or slightly higher, with the uppermost portion in the reticular or mid dermis.
Deep absorbable stitches should be placed so that the knot is facing downward. This placement reduces the likelihood that a spitting suture erupts to the surface. Deep stitches can be placed in either the subcutis, as shown here, or slightly higher, with the uppermost portion in the reticular or mid dermis.
Buried knots are cut on the knot while a small (0.25-in) tail is left on superficial sutures. The knots should be pulled to one side of the suture line. Impingement of knots directly on the suture line may distort the final result. Superficial sutures should not be so tight that the tissue is distorted or strangulated. Similarly, the manipulation of the wound edges with pickups and hooks should be minimized during closure, because the tissue can be damaged or perforated.
A slight excess in length along one edge of the wound can be sewn out. In other words, the surplus skin can be evenly distributed along the suture line so that no bulges or focal peaks are apparent. If the extra tissue is too extensive for this method, a dog ear may need to be excised.
For more information, see Medscape article Suturing Techniques.
Common stitches
Many types of suture configurations can be used to close an excision. The most common are the subcutaneous, or buried, stitch for deep sutures and the simple interrupted stitch or the running stitch for superficial sutures.
The subcutaneous stitch provides wound stability, closes dead space, everts the edges, and relieves tension. In deep wounds, the knot can be positioned upward, that is, with the needle pointed down with the first bite, without excessive tissue reaction. However, in most excisions, the knot is too close to the surface and should be buried; that is, the needle is pointed upward with the first bite to yield a knot directed downward, or buried. Stitches placed through only fat tend to pull through; therefore, a portion of the fascia or dermis should be included. On the other hand, stitches that are too superficial can cause the wound edges to pucker or cause eventual spitting of the suture to the surface of the wound. Vicryl is more likely to spit than the monofilament deep sutures.
The simple interrupted stitch is the most fundamental stitch in cutaneous surgery. It can be used to effectively close a large wound, finely evert the edges of a small or medium wound, and close wounds with edges at different heights. A few simple interrupted stitches can be placed to improve eversion or add strength along a running stitch. The disadvantages of the simple interrupted stitch include the potential for railroad-track scarring and the time required to place the stitches. Compared with running sutures, which are tied at only 2 ends, simple interrupted sutures are better at distributing tension and, hence, achieving eversion.
The placement of running stitches is a convenient, quick method in suturing well-approximated tissue with minimal residual tension. Such stitches are particularly useful on areas with loose skin such as the eyelids, neck, or scrotum. Running sutures are also easy to remove. However, compared with simple interrupted sutures, running stitches are not as strong, and optimal wound eversion and even distribution of the tension may be more difficult.
Subcuticular running sutures, which lie within the dermis just beneath the skin surface, are another type of stitching technique. [13] This stitch can be performed using absorbable or nonabsorbable sutures and prevents the appearance of track marks. It is typically used on the trunk and extremities. [14] This particular closure is not advised for high-tension areas or wounds with little eversion, as the suture itself does not promote eversion.
Even approximation of the wound edges is important. Failure to achieve such approximation can result in a problematic scar. In young, aesthetically conscious patients, secondary intention healing and the use of Steri-Strips alone does not provide a cosmetically acceptable result. Silk sutures may be used, but these alone do not correct uneven edges.
Other considerations
Lazy S repair
On convex surfaces, such as the extremities, a linear closure may result in buckling as the wound contracts and matures. An S- shaped ellipse (see image below) may reduce the tendency for such deformation by providing slack for contraction. The overall scar may be slightly longer, but it will be cosmetically more acceptable. Similarly, on the face, a curvilinear rather than straight ellipse may have cosmetic benefits in certain cases. Scars with curvature may blend better with natural skin lines and prevent impingement on adjacent cosmetic units.
 At areas such as the elbow, where the skin is intermittently stretched, an S-shaped closure can provide better camouflage in the skin tension lines and confer the desired laxity.
At areas such as the elbow, where the skin is intermittently stretched, an S-shaped closure can provide better camouflage in the skin tension lines and confer the desired laxity.
Dog-ear repair
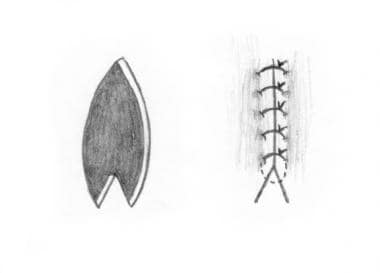
The cone of excess tissue that is created at either end of the aperture may have to be removed to permit even closure without wrinkling and bunching (see image below). This tissue can be removed by gently pulling the cone to one side of the excision axis with a hook and by extending the excision beyond it. The redundant triangle of tissue can be pulled across the excision line and cut parallel to the excision with scissors or a scalpel. Although it is important not to trim too much tissue, most novices err on the side of caution and fail to remove enough.
 If an approximately round defect is closed starting in the middle and moving outward, residual skin pouches form at the ends. These dog ears can be removed before closure or after the central closure is complete.
If an approximately round defect is closed starting in the middle and moving outward, residual skin pouches form at the ends. These dog ears can be removed before closure or after the central closure is complete.
M-plasty
Extending the excision to remove the dog ear may not be feasible because of the proximity of vital structures such as the lateral canthus of the eye or the vermilion border of the lip. In such cases, an M-plasty repair (see image below) may be indicated. With this process, the scar is shortened and deflected approximately 15° on either side of the main axis.
 An M-plasty can be performed to redirect the suture line away from an anatomically sensitive area such as the lateral canthus.
An M-plasty can be performed to redirect the suture line away from an anatomically sensitive area such as the lateral canthus.
Postoperative Care
Once the wound is closed, the surgeon should ensure that the tissue is well approximated and that hemostasis is maintained. The surgeon can firmly roll gauze over the length of the wound to expresses any blood if residual bleeding or a hematoma is present. These complications may require further management with sustained pressure, drainage, or reopening and exploration of the wound.
A topical ointment can be applied directly to the wound site. The function of topical ointment is to maintain a moist local environment while simultaneously facilitating the removal of the debris and crust to ensure cosmetically optimal reepithelialization. The risk of infection after cutaneous surgery is low, especially for superficial wounds in well-vascularized areas such as the head and neck. Consequently, all bland emollient (eg, petrolatum, Aquaphor Healing Ointment, topical antibiotic, similar preparation) are equally effective in facilitating wound healing. However, if a patient is using a topical antibiotic, the development of local erythema or irritation may indicate an allergic response, and the topical antibiotic should be switched to an entirely bland emollient such as petrolatum. With large or time-consuming excisions, oral antibiotic prophylaxis may be indicated.
After the topical ointment is applied, nonadhesive dressings (eg, Telfa) should be applied. Gauze placed directly on the wound makes dressing removal difficult and painful, and tearing of the closure is possible. However, a roll of gauze may be applied over the Telfa to serve as a pressure dressing for hemostasis. Stretchable adhesive tape, such as Hypafix, can be used to hold this dressing in place. Patients should be instructed to remove the dressing in 24-48 hours. Thereafter, the daily application of a topical ointment and an adhesive bandage after the wound is gently cleansed with soapy water should be sufficient.
Patients should avoid strenuous activity for at least 2 weeks after the excision procedure. Larger excisions and those on the trunk may be particularly vulnerable to exercise-related spreading. Smokers should be urged to abstain for at least a week, because smoking significantly impairs wound healing. Patients should contact their physician's office if excessive bleeding, redness, swelling, pain, fever, or other constitutional symptoms develop. The patient should be told that the continuous application of firm pressure for 15 minutes may stop any bleeding from the wound; however, if it does not, they should seek help. Prescription pain medications (eg, Tylenol with codeine) may be given if appropriate. Written instructions should also be provided because patients are often too tense or preoccupied to clearly recall verbal instructions.
Appointments for suture removal may be scheduled for 1-2 weeks after surgery. These follow-up visits afford the physician an opportunity to monitor the healing of the wound. Patients traveling from far away who have a nurse or physician nearby may not need a return appointment. The use of absorbable superficial sutures may be preferable in patients who are busy or unable to return for follow-up care.
For more information, see Medscape articles Surgical Dressings and Dermatologic Surgical Complications.
-
When freeing tissue with a scalpel, the surgeon can tug the skin laterally toward himself or herself to help ensure even depth. A pair of scissors easily stays in the correct plane and can be used to reflect the tissue ellipse upward.
-
At areas such as the elbow, where the skin is intermittently stretched, an S-shaped closure can provide better camouflage in the skin tension lines and confer the desired laxity.
-
An M-plasty can be performed to redirect the suture line away from an anatomically sensitive area such as the lateral canthus.
-
Top: Ellipses can be closed by using the rule of halves: The initial stitch is placed in the middle, and subsequent stitches are placed to bisect the remaining expanses. Bottom: Alternatively, in high-tension wounds, an easier approach may be placing stitches beginning at one end, where the tension is less, and then gradually moving toward the other end. A hybrid approach may entail starting with a middle stitch, which approximates the closure, and then placing stitches from one end to the other.
-
In the classic elliptical or fusiform excision, the edges are at an internal angle of 30°. Although this angle defines the relationship of the edge to the central lesion being removed, the actual cutting angle at the edge is typically broader, as demonstrated in the image.
-
Ellipses should be oriented in the relaxed skin tension lines. If the ellipses are placed carefully, linear scars are minimally noticeable. The locations of the skin tension lines vary slightly among individuals; therefore, stylized diagrams do not provide sufficient guidance. Close examination and pinching of the skin reveals the orientation of the lines.
-
The needle driver should be used to grasp the needle in the middle or slightly beyond the middle toward the insertion of the suture. Holding the needle too close to the end results in slippage and bending of the shaft.
-
Deep absorbable stitches should be placed so that the knot is facing downward. This placement reduces the likelihood that a spitting suture erupts to the surface. Deep stitches can be placed in either the subcutis, as shown here, or slightly higher, with the uppermost portion in the reticular or mid dermis.
-
If an approximately round defect is closed starting in the middle and moving outward, residual skin pouches form at the ends. These dog ears can be removed before closure or after the central closure is complete.
-
In general, the scalpel blade should be maintained perpendicular to the skin surface because vertically oriented cuts close most neatly and with the best eversion. The position of the hand may need to be modified when a topographically curved surface is incised.








