Background
In 1845, the surgeon Bernhard von Langenbeck together with the physician Antoinne Lembert described the first cases of human actinomycosis. Surgeons of the time considered it submandibular adenitis, while the dermatologists thought it was syphilis. [1] The term "actinomycosis" (from the Greek aktino and mykos translating to "ray-fungus") was given by the botanist and mycologist Carl Otto Harz. It derived from the characteristic filamentous, branching morphology of the organisms resembling fungal hyphae. The specimens evaluated by Harz represented material submitted by the pathologist Otto Bolliger, who had found the disease in jaws of cattle in 1877. [2] In 1878, the surgeon James A Israel demonstrated one of the species as a human infectious pathogen. [3, 4]
Actinomycosis is a chronic, slowly progressing, granulomatous infectious disease caused by human-associated Actinomyces species. It is well known that it represents an endogenous infection. The causative agents are inhabitants of mucosal surfaces and skin, gaining access by disruption of the epithelial barrier via trauma, surgical procedures, or foreign bodies. [5, 6, 7] Although actinomycosis is considered an uncommon disease, its true prevalence is not available. [5, 8, 9] Its clinical presentation includes features such as abscess formation, dense fibrotic tissue reaction, and draining sinus tracts. [6] The infection is usually classified according to the affected body site as orocervicofacial (50-65%), thoracic (15-30%), and abdominopelvic (20%). Less frequent sites of presentation include the central nervous (2-3%) and musculoskeletal (rare) systems, and a disseminated form (rare). [6, 7, 10, 11] Cutaneous actinomycosis is generally a secondary process to deeper tissue infection, spreading by direct extension or by hematogenous means. [5, 12, 13] It usually begins as an inflammatory soft-tissue mass/abscess, which may or may not develop fistulous tracts with draining sites.
Owing to the slowly progressing and indolent nature of the condition, in association to early nonspecific symptoms (ie, edema, low-grade fever, weight loss), initiation of medical care is occasionally delayed. [7] Additionally, the clinical and radiologic findings of actinomycosis are varied and may represent a challenge, owing to overlapping characteristics with other inflammatory, infectious, and neoplastic entities. [6] The diagnosis is established by microbiologic isolation of Actinomyces, in the appropriate clinical setting. Currently, 16S rRNA gene sequence analysis and MALDI-TOF mass spectrometry are both precise diagnostic methods adopted by multiple laboratories. [14, 15, 16]
The treatment of actinomycosis may require high-dose, prolonged antibiotic therapy, and, occasionally, an interventional procedure such as collection drainage or surgical excision/resection. [7, 8]
Pathophysiology
Actinomycosis is a bacterial infection that spreads by direct extension and, rarely, hematogenously. [3, 5, 12, 13] Actinomyces are found as commensal flora of human mucosae and skin, giving origin to foci of infection as a result of disruption of the epithelial surfaces secondary to trauma, surgical procedures, or foreign bodies. [5, 6, 7] Their pathogenicity is low, but little is known about their mechanism of infection. It has been speculated they may have the ability to evade the host's immune system. Additionally, since Actinomyces are frequently isolated from polymicrobial infections (75-95%), it has been presumed that interactions with other microorganisms contribute and synergistically enhance the pathogenic process. [5, 17]
See the image below.
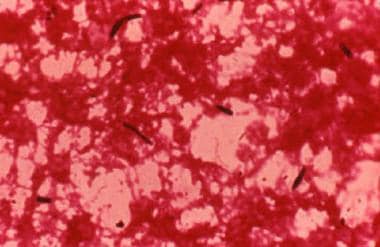 Photomicrograph of gram-positive organisms in actinomycosis, which may be confused with those causing a mycotic infection (hematoxylin and eosin, original magnification X40).
Photomicrograph of gram-positive organisms in actinomycosis, which may be confused with those causing a mycotic infection (hematoxylin and eosin, original magnification X40).
Etiology
The genus Actinomyces belongs to the family Actinomycetaceae, order Actinomycetales, and phyla Actinobacteria. It is currently composed of 54 validly published species. [18] These are anaerobic or microaerophilic, nonsporulating, nonmotile, gram-positive bacilli with filamentous and branching histopathological structures. [19] More than half of Actinomyces species have been associated with human infections, with Actinomyces israelii being the leading agent causing actinomycosis. Additional species associated with classic actinomycosis include Actinomyces gerencseriae and Actinomyces graevenitzii. A wide range of the published species are increasingly emerging as infectious agents at many body sites. [5] Detailed characterization of Actinomyces at nonoral human body sites is infrequent. [5]
Actinomyces is one of the predominant genera in the human oral microbiome, with at least 19 species currently identified as part of it. [20] Some of these play a central role in early biofilm formation. The total biomass of Actinomyces do not differ between periodontally healthy and diseased subjects, although a relative focal decrease in their numbers has been described in diseased sites. In general, it is thought they do not play a pathogenic role in periodontitis. [5, 21, 22]
See the image below.
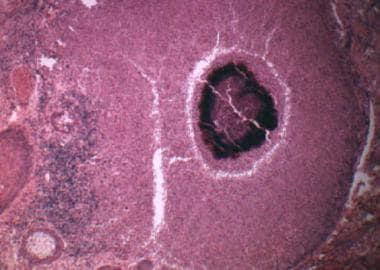 Photomicrograph of a characteristic sulfur granule of actinomycosis (hematoxylin and eosin, original magnification X10).
Photomicrograph of a characteristic sulfur granule of actinomycosis (hematoxylin and eosin, original magnification X10).
Epidemiology
Frequency
Actinomycosis occurs worldwide, although it is a rare infection. Little is known about its epidemiology, and the limited existing knowledge derives mostly from case reports and case series. Based on this information, Actinomyces affects people of all ages, without predilection for a particular race. Of note, a higher rate of infection has been seen among males, hypothesized (by circumstantial evidence) to be related to increased trauma or poorer dental hygiene. [19, 23] Some cases have been linked to specific conditions such as corticosteroid use, osteoradionecrosis or bisphosphonate-related osteonecrosis, leukemia, renal failure, congenital immunodeficiencies, and human immunodeficiency virus infection. [5, 19, 24, 25] While Actinomyces affect immunocompromised patients, most cases have been reported in immunocompetent individuals. [7, 8] Risk factors associated with orocervicofacial actinomycosis include, in addition to poor dental hygiene, smoking and heavy alcohol use.
Race
Actinomycosis has no race predilection.
Sex
Actinomycosis has a male predominance, with an approximate ratio of 3:1. [26]
Age
Actinomycosis affects subjects of all ages, although pediatric cases are less frequent. [5]
Prognosis
Actinomycosis is known for its slow progression and indolent nature. [7] Source control with antibiotic therapy and surgical interventions, as pertinent, are the mainstay of treatment. Prompt recognition of uncontrolled or advanced infection is critical to avoid the additional morbidity from radical and extensive surgeries. [27]
-
Photomicrograph of gram-positive organisms in actinomycosis, which may be confused with those causing a mycotic infection (hematoxylin and eosin, original magnification X40).
-
Photomicrograph of a characteristic sulfur granule of actinomycosis (hematoxylin and eosin, original magnification X10).
-
Oral fistula due to actinomycosis.
-
Periapical radiograph shows infection in the premolar tooth.








