Overview
Venous insufficiency leading to varicose veins can be a serious, progressive process. When the refluxing circuit involves failure of the primary valves at the saphenofemoral junction, treatment options for the patient are limited, and early recurrences are the rule rather than the exception.
In the historical surgical approach, ligation and division of the saphenous trunk and all proximal tributaries was followed either by stripping of the vein or by avulsion phlebectomy. Proximal ligation requires a substantial incision at the groin crease. Stripping of the vein requires additional incisions at the knee or below and is associated with a high incidence of minor surgical complications. Avulsion phlebectomy requires multiple 2- to 3-mm incisions along the course of the vein and can cause damage to adjacent nerves and lymphatic vessels.
Endovenous ablation has replaced stripping and ligation as the technique for elimination of saphenous vein reflux. One of the endovenous techniques is a radiofrequency-based procedure. Additional methods of radiofrequency delivery were introduced in 2007. Endovenous procedures are far less invasive than surgery and have lower complication rates. The procedure is well tolerated by patients, and it produces good cosmetic results. Excellent clinical results are seen at 4-5 years, and the long-term efficacy of the procedure is now known with 10 years of experience. [1, 2, 3, 4, 5] The original radiofrequency endovenous procedure was cleared by the US Food and Drug Administration (FDA) in March 1999.
Endovenous techniques (endovenous laser therapy, radiofrequency ablation, and endovenous foam sclerotherapy) clearly are less invasive and are associated with fewer complications compared with more invasive surgical procedures, with comparable or greater efficacy. [6, 7, 8, 9]
Technology
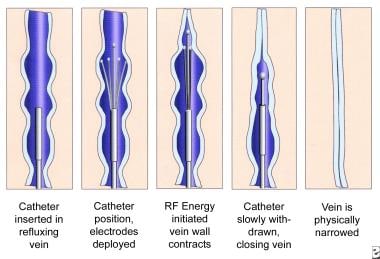
The original radiofrequency endovenous ablation system worked by thermal destruction of venous tissues using electrical energy passing through tissue in the form of high-frequency alternating current. This current was converted into heat, which causes irreversible localized tissue damage. Radiofrequency energy is delivered through a special catheter with deployable electrodes at the tip; the electrodes touch the vein walls and deliver energy directly into the tissues without coagulating blood. The system called ClosureFast delivers infrared energy to vein walls by directly heating a catheter tip with radiofrequency energy.
Energy delivery
In the original radiofrequency catheter system, the catheter was pulled through the vein while feedback was controlled with a thermocouple to a temperature of 85°C to avoid thermal injury to the surrounding tissues or carbonization of the vein wall. With the new system, the catheter is held in place while energy heats the catheter to a specified temperature of 120ºC. As the vein is denatured by heat, it contracts around the catheter.
With the previous-generation radiofrequency system, as shrinkage and compaction of tissue occurred, impedance was decreased, which decreased heat generation; however, this is no longer the case. Only the temperature of the catheter metal core is monitored as it delivers heat to the vessel wall in 20-second increments. Previously, the radiofrequency generator could be programmed to rapidly shut down when impedance rose, thus assuring minimal heating of blood but efficient heating of the vein wall. In the present system, catheter core temperature is monitored and adjusts energy to keep the core at 120 º C. Heat delivered to the vein wall causes the vessel to shrink in the treated area, and the catheter is gradually withdrawn along the course of the vein until the entire vessel has been treated. This is performed in 7-cm segments.
The image below demonstrates a schematic diagram of the process.
Catheters
Many different radiofrequency ablation catheters are available for medical applications. The ClosureFast (manufactured by Medtronic) and Venclose radiofrequency vein ablation devices are two systems commercially available in the United States. The ClosureFast system offers two catheters, 3 cm and 7 cm in size, while the Venclose system developed one catheter capable of two heating lengths (2.5 cm and 10 cm).
Histologic Findings
Immediately after treatment, biopsy specimens show a significant reduction in the size of the vein lumen, with denudation of endothelium, thrombus formation, thickened vessel walls, loss of collagen birefringence, and inflammatory changes. The zone of thermal damage is limited to 2 mm beyond the point of contact with the electrodes.
In more than 90% of patients, biopsy specimens demonstrate complete occlusion of the vein lumen 6 weeks after treatment. The lumen is completely ablated in most areas, with some portions of the vessel demonstrating a small residual lumen containing organized fibrous thrombi. Birefringence is present, and new collagen growth is evident.
Technique
Radiofrequency ablation catheters cannot be easily passed along a tortuous superficial vein; therefore, the procedure is principally of use in the treatment of truncal varicose veins, such as the great saphenous vein. Radiofrequency ablation is also used with small saphenous vein incompetence.
Preprocedure
Duplex ultrasonography is used to confirm and map all areas of reflux and to trace the path of the refluxing great saphenous trunk from the saphenofemoral junction down the leg to the lower thigh or upper part of the calf. The vein, the saphenofemoral junction, and the anticipated entry point are marked on the skin. An appropriate entry point is selected just above or just below the knee, at a point permitting cannulation of the vessel with a 16-gauge needle introducer.
Procedure
The leg is prepared and draped, and a superficial local anesthetic agent is used to anesthetize the site of cannulation. Needle puncture of the vessel is guided by duplex ultrasonography. The Seldinger technique is used to place a guidewire into the vessel, and an introducer sheath is passed over the guidewire, which is removed. The ClosureFast catheter is passed through the sheath, and the tip is advanced to 2 cm below the saphenofemoral junction under duplex ultrasonographic visualization.
With ultrasonographic guidance, a local anesthetic agent is injected into the tissues surrounding the great saphenous vein above and within its fascial sheath. The anesthetic is injected along the entire course of the vein from the catheter insertion point to the saphenofemoral junction. In most patients, 200-400 mL of lidocaine 0.1% is sufficient to both anesthetize and compress the vessel. Note the importance of delivering the anesthetic agent in the correct intrafascial location, with a volume sufficient to compress the vein and dissect it away from other structures, such as nerves, along its entire length.
Duplex ultrasonography is used to position the catheter tip 2 cm below the level of the terminal valve of the saphenofemoral junction. The catheter must not extend into the femoral vein because injury to the femoral vein may cause deep vein thrombosis.
In the previous radiofrequency ablation system, when the console is switched on and the test mode is activated, the baseline impedance should be 250-300 ohms and the baseline temperature should be 32-37°C. When radiofrequency energy is applied, the thermocouple temperature should rise to 80-85°C within 10-15 seconds. In the new system, when the radiofrequency is activated, the catheter core temperature should rapidly rise to 120ºC and should be sustained for 15 seconds of the 20-second pulse cycle. If the temperature does not rise quickly, a malpositioned catheter tip should be strongly suspected.
In the previous system, after the temperature reaches 85°C and remains constant for 15 seconds, the catheter tip is slowly withdrawn at a rate of approximately 1 cm per minute (1 mm every 6 seconds). In the new system, two 20-second cycles are performed in the proximal section, after which the catheter is withdrawn 7 cm as per catheter markings. The next 20-second cycle is repeated once, and, if 120ºC is maintained, the catheter is then withdrawn another 7 cm until the entire vein is treated.
When proper tumescent anesthesia is performed, the patient should never experience a sudden heat sensation. If this happens, more anesthetic is injected.
Postprocedure
Posttreatment duplex ultrasonography confirms the contraction of the vessel and the absence of flow along the entire length of the treated vessel. In the previous system, if persistent flow is observed, the procedure may be repeated immediately, provided the catheter can still be easily passed along the vessel to the desired site of treatment. In the new system of ClosureFast, the procedure is not repeated because the targeted vessel typically shows no flow.
Follow-up Care
Compression is of vital importance after any venous procedure. Compression is effective in reducing postoperative bruising and tenderness, and it can also reduce the risk of venous thromboembolism in both the treated leg and the untreated leg.
A class II (30- to 40-mm Hg gradient) compression stocking is applied to the treated leg, and, if the patient is willing, it is also applied to the untreated leg. Bed rest and lifting of heavy objects are forbidden, and normal activity is encouraged.
The patient is reevaluated 3-7 days after the operation, at which time duplex ultrasonography should demonstrate a closed great saphenous vein and no evidence of thrombus in the femoral, popliteal, or deep veins of the calf.
At 6 weeks, an examination should reveal clinical resolution of truncal varices, and an ultrasonographic evaluation should demonstrate a completely closed vessel and no remaining reflux. If any residual open segments are noted, sclerotherapy is performed under ultrasonographic guidance.
For patient education resources, see Varicose Veins.
Complications
Reported complications of the procedure are rare. Local paresthesias can occur from perivenous nerve injury but are usually temporary. Thermal injury to the skin was reported in clinical trials when the volume of local anesthetic was not sufficient to provide a buffer between the skin and a particularly superficial vessel, especially below the knee. Progression of thrombus from local superficial phlebitis has occasionally been observed when compression was not used. The greatest current area of concern is deep vein thrombosis, with one 2004 study documenting deep vein thrombus requiring anticoagulation in 16% of 73 limbs treated with a radiofrequency ablation procedure. [10, 11, 12]
Outcomes
Published results show a high early success rate with a very low subsequent recurrence rate up to 10 years after treatment. Early and mid range results are comparable to those obtained with other endovenous ablation techniques. The authors’ overall experience has been a 90% success rate, with rare patients requiring a repeat procedure in 6-12 months. Overall efficacy and lower morbidity have resulted in endovenous ablation techniques replacing surgical stripping.
Patient satisfaction is high and downtime is minimal, with 95% of patients reporting they would recommend the procedure to a friend.
In a study of 104 patients (147 limbs) treated with radiofrequency endovenous ablation for varicose veins of the lower extremities, including 82 patients (121 limbs) with great saphenous varicose veins, occlusion was achieved in 99.4% of the targeted veins. One limb demonstrated partial recanalization, and endovenous heat-induced thrombosis occurred in five limbs, although the thrombi vanished within 1 month postintervention, with no antithrombotic therapy needed. Patients were followed up for 12 months. [13]
A study by Proebstle et al found that at 5-year follow-up, radiofrequency segmental thermal ablation remained a successful treatment for over 90% of patients who underwent the therapy for incompetent great saphenous veins. The vein occlusion rate was 91.9% at last follow-up, with the Venous Clinical Severity Score changing from 3.9 at baseline to 0.6 at 1 year, 0.9 at 3 years, and 1.3 at 5 years. [14]
A study by Baccellieri et al indicated that in radiofrequency ablation of the great saphenous vein, risk factors for the vein’s recanalization include the accessory saphenous vein being directly confluent with the saphenofemoral junction, a history of more than two pregnancies, and a great saphenous vein diameter of, preoperatively, over 10 mm. The investigators also reported that age over 70 years and incompetent perforator veins increase the likelihood of varicose vein recurrence. The study’s mean follow-up period was 57.2 months. [15]
A study by Bush et al indicated that perforating veins are the most frequent cause of recurrent varicose veins after radiofrequency or laser ablation. Of 2380 patients involved in the study, 164 had a recurrence of varicose veins, with the median period to recurrence being 3 years. Among the patients who experienced recurrence, 159 had undergone great saphenous vein ablation as their initial treatment, including 52 who had concurrently undergone small saphenous vein or anterior accessory great saphenous vein ablation. Along with perforating veins (64% of patients), the most common factors behind varicose vein recurrence were as follows [16] :
-
Recanalized great saphenous vein (29% of patients)
-
New anterior accessory great saphenous vein reflux (24% of patients)
-
New small saphenous vein reflux (15% of patients)
It was also found that a higher rate of recanalization occurred with radiofrequency ablation than with the laser procedure.
A study by Bissacco et al indicated that in patients who undergo endovenous radiofrequency ablation, independent risk factors for recanalization of the great saphenous vein consist of the presence of CEAP (clinical, etiologic, anatomic, and pathophysiologic) class C4 or C5 venous disease, a preoperative great saphenous vein diameter of over 6 mm, and a history of smoking. Dependent risk factors consisted of patient age over 61 years and such postoperative complications as pigmentation, edema, and paresthesia. The investigators also found, at follow-up periods of 1 week and 1, 3, and 5 years, recanalization rates of 2.4%, 4.3%, 9.3%, and 17.5%, respectively. [17]
A study by Bozoglan et al also suggested that endovenous laser ablation may have some advantages over radiofrequency ablation of varicose veins. The study included 60 patients with bilateral saphenous vein insufficiency, each of whom had one leg treated with the radiofrequency procedure and the other treated with laser therapy. The investigators found that the recanalization rate was 6.8% in the legs treated with radiofrequency ablation, compared with 0% in the laser-treated legs. Moreover, 51.7% of patients were satisfied with endovenous laser ablation, versus 31.0% who were satisfied with radiofrequency ablation (and 17.2% who were satisfied with both procedures). [18]
However, a retrospective study by Hwang et al indicated that radiofrequency ablation has certain advantages over 980-nm endovenous laser ablation in the treatment of recurrent varicose veins associated with residual great saphenous vein insufficiency, as can appear following saphenofemoral ligation with or without stripping. The investigators reported that such recurrence was safely and effectively treated in the study with 980-nm or 1470-nm endovenous laser ablation or radiofrequency ablation, with the three modalities together responsible for complete closure in 35 out of 37 limbs (94.6%). However, the Venous Clinical Severity Score (VCSS) saw a significantly greater decrease and the ecchymosis grade was significantly lower in the limbs treated with radiofrequency ablation than in those managed with 980-nm endovenous laser ablation. [19]
Similarly, a literature review by Ahadiat et al suggested that endovenous laser therapy leads to a lower recurrence rate than radiofrequency ablation in the treatment of varicose veins of the great saphenous vein but that radiofrequency ablation may lead to less postoperative pain and bruising. [20]
While finding that incompetent great and anterior accessory saphenous veins in the thigh can safely and effectively treated be treated with either radiofrequency or microfoam ablation, Talutis et al reported the rate of complete vein closure to be higher in association with radiofrequency ablation (100%) than with the microfoam procedure (90%). [21]
-
Schematic images of the process of radiofrequency endovenous occlusion.
-
Radiofrequency ablation console (VNUS Medical Technologies) showing (left to right) time, temperature, impedance, and power (in watts).
-
Closure radiofrequency ablation catheters in 2 sizes (VNUS Medical Technologies).