Practice Essentials
Dermabrasion is a tried and true method for ablative facial resurfacing. Numerous laser resurfacing technologies are available in the marketplace and can be very costly devices with associated costly disposables for each use. Dermabrasion is highly cost effective and predictable when performed for the appropriately selected use.
Background
The face is arguably the most critical aesthetic unit of the human body. The art of facial rejuvenation has been practiced since ancient civilizations, and the interest in this subject continues to grow. Various options exist to perform skin resurfacing of the face, including dermabrasion, laser resurfacing, and chemical peels. [1, 2, 3, 4, 5] All skin-resurfacing modalities aim to remove damaged skin and stimulate normal wound healing. Dermabrasion is a simple, cost-effective means of skin resurfacing that can provide repeated and reliable results when used on the face or many other areas of the body.
The goal of dermabrasion is to remove a controlled thickness of damaged skin to stimulate normal wound healing and skin rejuvenation, while avoiding the complications of scarring and pigmentary changes. [6, 7] This controlled damage rapidly heals because of the abundance of a rich vascular and adnexal network along with the supply of macronutrients, which promotes tissue remodeling of the proteins and structures of the skin, yielding rejuvenated skin that is smoother and firmer than before.
Numerous studies have demonstrated that dermabrasion is a reliable and effective method for skin resurfacing and should be a part of a plastic and dermatologic surgeon's repertoire in resurfacing damaged skin and the aging and damaged face. [8] It has features that make it superior to chemical peels and lasers, including the ability to use it in focal segments of the face, the lower likelihood of injury to the pigment-containing melanocytes resulting in pigmentary changes, and the much lower cost compared with laser treatments. With experience, the risks of scarring and skin sloughing due to traction injuries are very low.
The development of antiviral medications, semipermeable dressings, tumescent anesthesia, and cryoanesthesia has advanced the technique of dermabrasion, as well as other resurfacing surgeries such as chemical peeling, ablative laser resurfacing (see Carbon Dioxide Cutaneous Laser Resurfacing and Erbium-YAG Cutaneous Laser Resurfacing), nonablative laser resurfacing, and microdermabrasion. A comprehensive understanding of the advantages and the disadvantages of each of these resurfacing procedures is necessary to achieve optimal surgical results in patients who undergo resurfacing surgery.
See the image below.

Anatomy
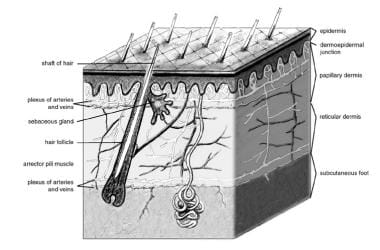
The most important element in dermabrasion is recognition of the appropriate depth of treatment. The skin is composed of 2 mutually dependent layers, the epidermis and the dermis, which rest on a fatty subcutaneous layer. The epidermis contains no blood vessels and protects the underlying dermis from the external elements. The epidermis is entirely dependent on the underlying dermis to deliver nutrients and to remove waste by means of diffusion across the dermoepidermal junction. An important function of the dermis is to sustain and support the epidermis. The dermis is divided into 2 layers: the relatively superficial papillary dermis and the relatively deep reticular dermis. Collagen, elastic tissue, and reticular fibers are present throughout both layers.
Epidermal appendages are intradermal epithelium-lined structures that can divide and differentiate. They develop as downgrowths of the epidermis into the dermis. They include sebaceous glands, sweat glands, apocrine glands, mammary glands, and hair follicles. Epidermal appendages serve an important role as a source of epithelial cells. These appendages are responsible for reepithelialization if the overlying epidermis is removed or destroyed in situations such as partial-thickness burns, chemical peeling, dermabrasion, traumatic abrasions, or harvesting of split-thickness skin grafts. See the image below.
Controlled dermabrasion can be performed on the epidermis and on the upper layers of the dermis. The wound heals by means of reepithelialization from the remaining epidermal appendages, similar to the healing of partial-thickness burns. Reepithelialization begins within 24 hours of wounding and is usually complete after 7-10 days. Collagen remodeling continues for 3-6 months and results in dermal thickening and contraction, which further enhance the smoothing effect.
Areas of the body where the skin adheres closely and tightly to underlying structures are referred to as adherent or tight structures. Those areas where the skin can be very loose, such as the neck and upper and lower eyelids, are referred to as loose areas. Dermabrasion must be performed evenly across the entire area to be treated, and the leading edge needs to be as deep as the trailing edge of the abrader. This is very difficult to perform in areas that are very loose, even with cooling of the skin. Wherever possible, progression should go from fixed areas to looser areas rather than in the opposite direction. Areas of very loose skin can be caught within a mechanical dermabrader and sheared off completely, leaving a severe deficit, which can cause open wounds and scarring. Extremely loose areas should be approached with caution and only by an experienced dermabrasion specialist.
Pathophysiology
With aging, the skin undergoes atrophy. This process typically begins during the fourth decade of life. The outermost portion of the epidermis, the stratum corneum, becomes disorganized and less effective as a protective barrier to the external environment. A gradual decline also occurs in the number of melanocytes populating the basal layer of the epidermis. The dermoepidermal junction becomes flattened because fewer dermoepidermal papillae are present. The most significant changes occur in the dermis, where an overall loss of organization occurs as the dermis thins with age. The amount of ground substance decreases and elastic fibers degenerate, making the skin less resistant to deformational forces. Collagen is also lost, and the proportion of type I collagen relative to type III collagen is reduced.
Actinic damage also produces changes in the skin, resulting in skin that actually thickens. Actinic keratoses and lentigines form. Dermal elastosis results from accumulation of thickened degraded collagen and elastic fibers. Ground substance also increases, while mature forms of collagen decrease. Facial rhytides occur, probably as the result of a combination of aging, photodamage, gravity, and repeated use of the muscles of facial expression.
Prognosis
Dermabrasion is a well-established technique for skin resurfacing using mechanical abrasion of the skin. It can yield excellent results when a well-trained surgeon performs the procedure for the appropriate patient. The keys to performing dermabrasion are experience and understanding of its principles to provide sufficient resurfacing to the appropriate depth and minimize scar formation. [8] Careful patient screening is crucial to ensure realistic expectations. [8] With meticulous postoperative care, the results can be highly satisfying for patients.
With the armamentarium of resurfacing modalities increasing, mechanical dermabrasion remains an important dermatosurgical procedure, particularly for the improvement of cystic acne, postsurgical scars, partial-thickness Mohs defects, and the visual appearance of skin grafts.
Small areas may be easily and safely treated with proper technique, and these areas demonstrate rapid recovery. Although experience and skill are necessary in order to avoid serious complications with full-face dermabrasion, its efficacy for the treatment of acne scarring and deep rhytides currently remains unmatched for the patient who is willing to endure the resultant recovery period.
Close follow-up during the postoperative period is important in order to recognize and treat the most serious potential complications of infection and scarring at the earliest stages. While new technologies continue to emerge, mechanical resurfacing will likely remain an essential and unmatched modality for scar improvement.
Patient Education
Preoperative counseling is imperative to ensure realistic patient expectations. The patient's desired outcome must be clearly communicated and understood. Physicians may show patients preoperative and postoperative photos of patients treated with dermabrasion; complications should be included. In general, dermabrasion yields 35-50% subjective improvement of skin texture. Patients should not expect restoration of perfect skin, and dermabrasion does not affect skin redundancy or eliminate the possible need for rhytidectomy. Patients should be told that the greatest improvement is usually observed 6 months after surgery. Patients should be provided a reference list of alternative procedures and should be instructed that combining other procedures with dermabrasion is not uncommon.
Patients should avoid sun exposure before and after the procedure. Some surgeons prescribe antiviral prophylaxis to all patients, and patients with a history of herpes simplex should receive strong prophylactic doses of acyclovir 400 mg 3 times daily or valacyclovir 500 mg twice daily, beginning the day of, or even prior to, the procedure. The herpes virus requires viable epidermal cells to establish an infection. Therefore, antiviral therapy should continue for 10-14 days to allow complete reepithelialization to occur. Prophylactic antibiotics are usually not needed. However, patients with a history of impetigo, staphylococcal skin infection, or a compromised immune system may benefit from antibiotics.
After a patient is appropriately selected, the physician obtains informed consent for the procedure. This process includes a thorough discussion of possible complications. Select patients may require preoperative laboratory screening to include complete blood cell count and serum chemistries. In addition, at-risk individuals should be screened for HIV and infectious hepatitis
-
Skin anatomy.
-
Technique and hand position for dermabrading raised scars.
-
Dermabrasion of a raised scar.
-
Technique of dermabrasion for a depressed scar.
-
A Bell hand engine is pictured.
-
End pieces, such as a wire brush and a diamond fraise, commonly used for abrading are shown.
-
Frigiderm is an effective spray refrigerant used in wire brush and diamond fraise dermabrasion.
-
Freeze defects and rhytides in their relaxed state without stretching or distorting so that they may be sculpted and recontoured.
-
To hold the hand engine properly, the forefingers grasp the body of the hand engine while the thumb stabilizes the neck.
-
For full-face procedures, beginning abrading at the dependent areas along the mandible or the chin and working toward the center of the face is best.
-
Dressing for full-face dermabrasion is shown.
Tables
Type |
Skin Color |
Characteristics |
I |
Very white |
Always burns, never tans |
II |
White |
Usually burns, tans with difficulty |
III |
White or light brown |
Mildly burns, average ability to tan |
IV |
Brown |
Rarely burns, tans easily |
V |
Dark brown |
Very rarely burns, tans very easily |
VI |
Black |
Never burns, darkly pigmented |
Skin Type |
Age (y) |
Clinical Findings |
I (mild) |
20-30 |
Early photoaging, fine wrinkling |
II (moderate) |
30-40 |
Early to moderate photoaging, present with motion, no keratoses |
III (advanced) |
50 and over |
Advanced photoaging, wrinkles with rest, visible keratoses, noticeable discolorations |
IV (severe) |
60 and over |
Severe photoaging, wrinkles throughout, dynamic and gravitational wrinkling, actinic keratoses |








