Practice Essentials
Granular cell tumors are uncommon lesions, although the head and neck region accounts for approximately 50% of all lesions. A somewhat similar lesion, congenital epulis, occurs less frequently than the granular cell tumor and occurs on the alveolar ridge of newborns. Note the images below.
Etiology
The etiology of oral granular cell tumors is unknown. Also see Pathophysiology.
Prognosis
The prognosis is excellent, and recurrence is uncommon. Malignancy is limited to approximately 1-2% of all granular cell tumors. [1]
Signs and symptoms
Granular cell tumors are slow-growing lesions (0.5-1 mm per year) that are neither painful nor tender. Congenital epulis apparently is neither painful nor tender. The rate of growth is difficult to determine because of its presence at birth and the need for its removal to allow feeding. No etiologic factors appear to be associated with either lesion. Note the image below.

The head and neck region accounts for approximately 45-65% of all sites for granular cell tumors. Approximately 70% of oral granular cell tumors occur in the tongue. [2, 3] Buccal mucosa accounts for about 10-15% of oral lesions. Approximately 10% of lesions have been reported bilaterally. Multiple tumors are occasionally present. [4, 5, 6] They have been found to occur in the lungs and trachea [7] ; the esophagus [8] ; the cecum [9] ; the colon, appendix, and mesentery [10] ; the perianal area [11] ; and the skin of the breast, scalp, [12] trunk, [13] and extremities. [14]
Congenital epulis occurs more frequently in the maxilla. These lesions generally are less than 2 cm in diameter. Large lesions can interfere with breathing and feeding. [15, 16]
Diagnostics
No clinical laboratory tests are used for these lesions. A definitive diagnosis requires biopsy.
Conservative excisional biopsy is indicated because both lesions are rarely larger than 2 cm in diameter. As a general rule, the depth of biopsy for granular cell tumors approximates the diameter of the lesion. Margins do not need to be extensive; generally, a few millimeters is adequate.
The depth of biopsy for congenital epulis is the periosteum. Removal of bone is not indicated. Since these are exophytic lesions, surgical margins do not need to be much greater than the clinical margins.
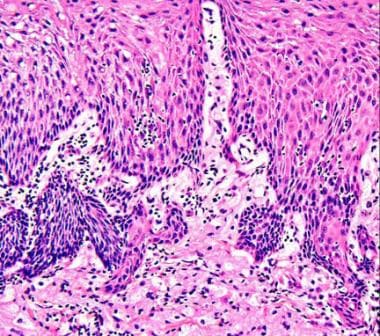
The granular cell tumor is characterized by the presence of sheets or clusters of plump, polygonal cells with a granular cytoplasm. These lesions are not circumscribed and often come into intimate contact with the overlying surface squamous epithelium. A frequent finding is pseudoepitheliomatous hyperplasia of the overlying epithelial layer. These cells generally are uniform and do not exhibit significant atypical features. Malignant granular cell tumors, which fortunately are rare, may have a very benign histologic appearance. Tumor cells more or less stain uniformly positive for S-100 protein, neuron-specific enolase, CD68, PGP9.5, and inhibin alpha. [17, 18, 19, 20]
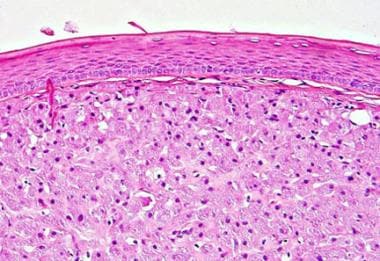
Congenital epulis also contains sheets and/or clusters of plump cells with a granular cytoplasm and rounded or oval nuclei. [21]
Pseudoepitheliomatous hyperplasia generally is not present. Congenital epulis lacks specificity for S-100 protein and is vimentin positive.
Management
Treatment for granular cell tumors and congenital epulis is surgery. While extensive surgery is not indicated, recurrence of granular cell tumors has been reported several years after removal. Recurrence of congenital epulis has not been reported; however, the number of total cases is small. If congenital epulis is asymptomatic and surgery is deferred, the lesion may regress spontaneously. [22]
Excision with a scalpel under local anesthesia is the preferred method; however, surgical margins are difficult to determine intraoperatively in the case of the granular cell tumor. Excision down to the periosteum usually is the goal for treating congenital epulis; however, recurrence does not seem to occur even if this lesion is not completely removed.
Granular cell tumors have been reported to recur several years after removal. Long-term follow-up care is warranted.
Pathophysiology
In 1926, Abrikossoff first described granular cell tumors. The origin of these lesions was believed to be from skeletal muscle because they were found insinuated within muscle. For many years, these lesions were referred to as granular cell myoblastoma. It was not until the advent of electron microscopy that the origin from muscle came into question.
Granular cell tumors now generally are accepted as being of neural origin, either Schwann cell or neuroendocrine. Immunocytochemical markers for S-100, neuron-specific enolase, myelin basic protein, and protein gene product 9.5 (PGP9.5) support a neural origin. [23]
Malignant granular cell tumors are extremely uncommon, accounting for less than 2% of granular cell tumors. [24] Granular cell tumor with an overlying squamous cell carcinoma has been reported. [25]
Congenital epulis is a lesion found on the alveolar ridge of newborns. Histologically, these lesions appear similar to the granular cell tumor; however, congenital epulis is negative for S-100 and other markers found in the granular cell tumor. Pseudoepitheliomatous hyperplasia, a frequent finding in granular cell tumors, generally is not present over the congenital epulis. Malignant congenital epulis has not been reported.
Epidemiology
Frequency
Oral granular cell tumor is too uncommon to accurately assess an incidence rate.
Race-, sex-, and age-related information
Granular cell tumors occur more commonly in blacks than in whites. Congenital epulis does not appear to have a racial predilection.
Granular cell tumors occur twice as frequently in females than in males. The occurrence rate for congenital epulis is approximately 8-10 times more common in females than in males.
The age range for occurrence of granular cell tumors is from the second to the eighth decade, most frequently in the fourth and fifth decades. [26] However, congenital oral granular cell tumor has been reported in a neonate,27 and non-congenital granular cell tumor of the tongue was reported in a 16-year-old female. [27]
-
Clinical photograph of a granular cell tumor on the tongue of a 38-year-old man.
-
Granular cell tumor.
-
Congenital epulis.




