Background
Buruli ulcer, caused by Mycobacterium ulcerans, is a chronic, debilitating, necrotizing disease of the skin and soft tissue. Buruli ulcer is an emerging infectious disease and is the third most common mycobacterial disease of the immunocompetent host, after tuberculosis and leprosy. [1] Although it has been reported in over 33 countries around the world, the greatest burden of disease is in the tropical regions of West and Central Africa, Australia, and Japan. [2] It primarily affects children aged 5-15 years. [2] Buruli ulcers generally begin as a painless dermal papule or subcutaneous edematous nodule, which, over a period of weeks to months, breaks down to form an extensive necrotic ulcer with undermined edges. Treatment includes a prolonged course of antibiotics and surgical debridement. Early identification and treatment are key, as lesions heal with scarring that can be a significant source of morbidity. Other names for this entity include Bairnsdale ulcer, Daintree ulcer, Mossman ulcer, and Searl ulcer. Note the image below.
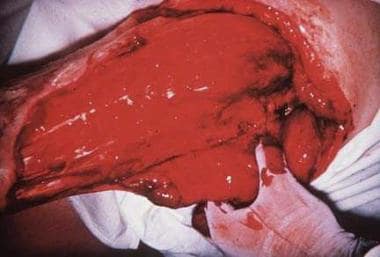 Buruli ulcer can extend to 15% of a person's skin surface and may destroy nerves and blood vessels. Metastatic bone lesions may develop.
Buruli ulcer can extend to 15% of a person's skin surface and may destroy nerves and blood vessels. Metastatic bone lesions may develop.
Buruli ulcer was first described by Sir Albert Cook in patients from Buruli County in Uganda, and the causative organism was isolated in 1948 by MacCallum in the Bairnsdale region of Victoria, Australia. A reemergence of cases led the 1998 World Health Organization (WHO) to reclassify Buruli ulcer as a "neglected emerging infectious disease," which has stimulated ongoing research into diagnosis, pathogenesis, and effective treatment. [3, 4, 5]
Pathophysiology
M ulcerans are slow-growing mycobacteria that produce a soluble polyketide exotoxin called mycolactone, which can diffuse extensively in the subcutaneous tissue. Because mycolactone has both immunosuppressive properties and cytotoxic properties, dramatic tissue destruction occurs without inducing inflammation or systemic symptoms, such as fever, malaise, or adenopathy. [6, 7, 8, 9, 10] Mycolactone was first identified in 1999. Research has revealed the mechanisms of action of mycolactone, as described below.
Molecular targets
Mycolactone targets scaffolding proteins, such as the Wiskott-Aldrich syndrome protein (WASP), [11] which controls actin dynamics and leads to a loss of cellular detachments and cell death. [12]
Mycolactone also inhibits the function of the Sec61 translocation, which is responsible for protein translocation into the endoplasmic reticulum. This affects 30-50% of mammalian proteins, including circulating inflammatory mediators and proteins involved in lipid metabolism, coagulation, and tissue remodeling. [13] Therefore, patients with M ulcerans infections have global and chronic defects in protein metabolism. This is evident by reduced levels of total serum proteins and blood urea nitrogen, without the presence of malnutrition, kidney impairment, or liver impairment. [13]
Buruli ulcers are traditionally thought to be painless ulcers. Research has shown that the hypoalgesic effect occurs via activation of the angiotensin II type 2 receptor (AT2R), leading to neurite degeneration and cell death. [14] Another prominent feature of Buruli ulcers is extensive coagulative necrosis caused by mycolactone.
Ogbechi et al showed that mycolactone decreased thrombomodulin expression on the surface of human dermal microvascular endothelial cells, thereby impairing the activation of protein C. This study also showed that fibrin deposition is a prominent feature of these ulcers and the tissue necrosis could be caused by fibrin-driven ischemia. [15]
Genetic susceptibility
Genetic susceptibility may be associated with the SCLC11A1 (NRAMP1) D543 polymorphism. [16]
Etiology
M ulcerans are slow-growing mycobacteria and are the causative agent of Buruli ulcers. The optimal temperature for growth is 30-32°C. This temperature is slightly below that of core body temperature and may explain some of the predisposition for lesions on the extremities and lack of visceral involvement. M ulcerans is sensitive to temperatures above 37°C, which has led to ongoing clinical trials using local heat application devices for treatment. [17]
M ulcerans is an environmental pathogen that has been isolated from biofilms and small aquatic animals of slow-moving or stagnant bodies of water. [18, 19, 20, 21] Although the exact mode of transmission is unknown, M ulcerans most likely causes infection through contamination of a traumatic wound. The absence of protective equipment during agricultural activities is a well-documented risk factor. [22] Proper wound hygiene has been shown to decrease infection rates. [23, 24, 25]
Because of its fragility and sensitivity to direct sunlight, M ulcerans likely persists within a protective host, although no hosts have been identified to date. [22] Transmission via the bites of Australian salt marsh mosquitoes with possums serving as the reservoir is supported by scientific evidence, but a mammalian reservoir has not been identified in other areas of the world. [23, 26, 27, 28] African biting water insects (Naucoridae, Belostomatidae, and Acanthamoeba species) have been implicated in the transmission of M ulcerans in ongoing research. [29, 28] Human-to-human transmission has rarely been reported. There is not an increased risk of infection associated with living with an infected family member. [23] In 2010, investigation of a familial outbreak of Buruli ulcers in Japan revealed matching insertion sequence 2404 in the infected wounds and crayfish found near the family's house. Given the location of the ulcers, direct inoculation was deemed unlikely. This supports the evidence that aquatic environments act as a reservoir for M ulcerans. [30]
A plasmid-encoded polyketide toxin termed mycolactone is responsible for the extensive destruction and suppressed host response in Buruli ulcers. Four variants have been identified. Mycolactone A and B are the more virulent variants and are found in Africa. Mycolactone C is found in Australia, and mycolactone D is found in Asia. [31] For more information, see Overview/Pathophysiology.
Epidemiology
US frequency
According to the World Health Organization (WHO), as of 2015, there have been no cases of confirmed Buruli ulcers originating in the United States. [3]
International frequency
Approximately 6000 cases are reported annually around the world, especially from rural Africa. [3]
Buruli ulcers have been reported in 33 countries. The largest number of endemic cases occur in countries in central and western Africa, such as Côte d'Ivoire, Benin, Ghana, Democratic Republic of the Congo, Cameroon, Nigeria, Togo, and Liberia. [32] Other involved geographic areas include Australia, Papa New Guinea, Japan, and sporadic cases in Central and South America. Subtropical and swampy terrain are major endemic foci for M ulcerans.
Race
No specific racial predilection is known.
Sex
No differences exist in the rates of infection among males and females.
Age
Buruli ulcer may affect any age group, but most cases occur in children ages 5-15 years, except in Australia, where Buruli ulcer is more prevalent in adults older than 50 years. [33]
Prognosis
Most patients have complete healing, with or without significant scarring or impairment. Even with medical and surgical care, patients often require hospitalizations averaging 3 months. The best prognosis occurs when treatment is instituted as early as possible before significant tissue destruction can occur. Without medical care, more than half the affected individuals are left with a functional limitation. The scarring can be disfiguring and can have a significant emotional and socioeconomic impact on patients. Treatment involves long hospital stays (average of 3 months), antibiotic regimens, and surgical procedures, which are resources often limited in endemic areas. [34]
Buruli ulcer has a low mortality rate; however, it is a significant source of morbidity and socioeconomic burden. Skin and soft-tissue necrosis can be extensive, involving as much as 15% of the patient's skin surface and may extend deep, exposing fascia, muscle, and bone.
When Buruli ulcers are identified early and treated appropriately, the prognosis is good. Klis et al found that 85% of patients who presented with small lesions and who received 8 weeks of antibiotics indicated no effect, or only a small effect, of the disease on their current life at long-term follow up visits. [35] The median score on the Dermatology Life Quality Index was 0 (range, 0-4), indicating a good quality of life. [35] These results highlight the importance of early identification and treatment, in stark contrast with the debilitating contracted scars that result if these ulcers are not treated in a timely manner.
The majority of the systemic complications from Buruli ulcers are from the toxicities of long-term antibiotic use. See Treatment/Complications section.
Elderly patients have a tendency towards more severe disease and increased complications from treatment. [33]
-
Buruli ulcer can extend to 15% of a person's skin surface and may destroy nerves and blood vessels. Metastatic bone lesions may develop.
-
An edematous Buruli ulcer in a 9-year-old Togolese girl. Courtesy of Wayne M Meyers, MD.
-
Photo of Togolese girl taken 5 years after the Buruli ulcer had been excised and repaired with autologous split-skin graft by GB Priuli, MD. Courtesy of Wayne M Meyers, MD.
-
Well-circumscribed ulceration with sharp, undermined borders on the lower leg. Courtesy of Ronald E Grimwood, Jr, MD, Baylor Scott and White Health.
Tables
Method |
Pros |
Cons |
Direct smear examination |
• Easy to perform at local level • Does not require expensive materials and equipment • Rapid results • Uses swabs, fine-needle aspiration, and biopsy samples |
• Low sensitivity (< 60%) • Needs trained personnel • Needs external quality assurance |
PCR |
• Results fairly rapid • Uses swabs, fine-needle aspiration, and biopsy samples • High sensitivity (>95%) |
• Requires a sophisticated laboratory • Expensive to perform • Needs trained personnel • Requires strict quality control |
Culture of M ulcerans |
• Uses swabs, fine-needle aspiration, and biopsy samples |
• Requires a sophisticated laboratory • Needs trained personnel • Results take >8 weeks • Low sensitivity (20-60%) • Not useful for immediate patient management |
Histopathology |
• Sensitivity is about 90% • Results fairly rapid (if services are available) • Useful in establishing differential diagnosis and monitoring unexpected response to treatment |
• Requires a sophisticated laboratory • Expensive to perform • Needs trained personnel • Requires invasive procedure (ie, biopsy) |
Category |
Form of Disease |
Treatment |
Primary Aim |
Secondary Aim |
Level of Health Care System |
Diagnosis |
I |
Small, early lesion (eg, nodules, papules, plaques, ulcers < 5 cm in diameter) |
Complete antibiotics If at or near a joint, maintain same movement as on unaffected side If surgery is needed in noncritical areas, consider this after 8 weeks of antibiotic treatment |
Cure without surgery Cure without movement limitations |
Reduce or prevent recurrence |
Community health centers and district hospitals |
Strong clinical diagnosis (with or without laboratory confirmation) |
II |
Nonulcerative and ulcerative plaque and edematous forms Single, large ulcerative lesion 5-15 cm in diameter |
Complete antibiotics, before surgery (if possible) If at or near a joint, maintain same movement as on unaffected side |
Cure without surgery Reduce extent of the surgical debridement when needed Cure without movement limitations |
Reduce or prevent recurrence |
Health centers, district and tertiary hospitals |
Strong clinical diagnosis (with or without laboratory confirmation) |
III |
Lesions in the head and neck region, particularly the face Disseminated/mixed forms (eg, osteitis, osteomyelitis, joint involvement) Multiple lesions and osteomyelitis Extensive lesion >15 cm |
Complete antibiotics, before surgery (if possible) If at or near a joint, maintain same movement as on unaffected side |
Cure without surgery Cure without movement limitations |
Reduce or prevent recurrence |
District and tertiary hospitals |
Strong clinical diagnosis (with or without laboratory confirmation) |





