Overview
Many men and women choose to remove unwanted body hair for cosmetic, social, cultural, or medical reasons. [1, 2] Medical indications for hair removal include the following:
-
Hypertrichosis: Congenital or drug-induced increase in hair growth in areas that are not androgen dependent; occurs in both men and women
-
Pseudofolliculitis (second image below): Hair growth from grafted donor sites, preoperative hair removal, and sex-change operations performed in men
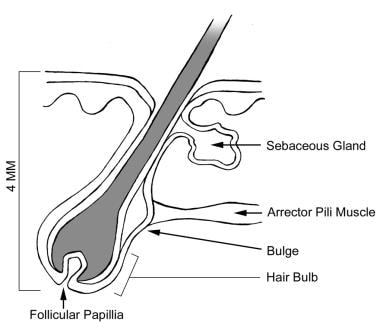
The third image below depicts the anatomy of a hair follicle.


Many methods are available for temporary or permanent hair removal, each with its own relative efficacy and adverse effects. Different methods for the removal of body hair include the following:
-
Temporary hair removal: Shaving, epilation, depilation, bleaching [7]
-
Temporary hair reduction: Eflornithine hydrochloride (VANIQA cream 13.9%)
-
Permanent hair reduction: Intense pulsed light, laser-assisted hair removal
-
Permanent hair removal: Electrolysis
The development of home-use devices is increasing. [8, 9] The Medscape Aesthetic Medicine Resource Center may be of interest.
Temporary Hair Removal
Shaving
Shaving is the method used most frequently to temporarily remove unwanted hair. Shaving is fast, easy, painless, effective, and inexpensive. The results are temporary—lasting from mere hours for facial hour to up to 3 days; as a result, shaving requires a constant commitment in order to maintain a hair-free appearance.
Shaving is performed with a razor on wet skin using shaving cream or other lubricants. The razor is often oriented against the direction of hair growth. For sensitive areas, shaving with the direction of hair growth may reduce cuts. Contrary to a widespread misconception, shaving does not result in increased hair growth or thicker hair. [10] The primary disadvantages and/or adverse effects of shaving include skin irritation, cuts in the skin, ingrown hair pseudofolliculitis, the need to shave daily, and stubble.
Compared with waxing, shaving is associated with considerably less discomfort. Both shaving and waxing, however, were found to significantly reduce body odor in the axillae when followed by soap washing. [11]
Epilation
Epilation involves the removal of the entire hair shaft and is the most effective method for temporarily removing hair. Epilation includes waxing, plucking, threading, sugaring, and using abrasives or mechanical devices (eg, Epilady). For epilation to be effective, treated hairs should be long enough for the device to grasp them. The long-term effects of epilation on the hair follicle are not known. Epilation wounds the hair follicle; therefore, repetitive epilation over several years may result in permanent matrix damage, resulting in finer or thinner hairs and, perhaps, as anecdotal evidence suggests, long-term permanent reduction in hair growth. Long-term clinical trials demonstrating the effects of repetitive epilation are lacking.
Plucking
Plucking is best performed using tweezers and is an economic method for removing the occasional coarse hair or a small cluster of hairs, such as those found on the eyebrows, chin, or nipples. The results of plucking last longer than shaving because hair is pulled from the hair shaft, as in waxing. This method is time consuming, tedious, and painful. Generally, plucking does not reduce the number of hairs that ultimately regrow. [12] The reaction of the hair follicle to plucking can be unpredictable, possibly resulting in adverse effects such as folliculitis, hyperpigmentation, scarring, ingrown hairs, and distorted follicles. Adverse effects from plucking include pain, hyperpigmentation, scarring, folliculitis, and ingrown hair pseudofolliculitis.
Waxing
Waxing is essentially mass plucking and involves applying warm or cold wax onto hair-bearing skin and quickly stripping off the hardened wax—along with the embedded hairs—against the direction of hair growth. [10] Waxing is the most expensive yet most effective method of epilation because hair is removed completely from the hair shaft in large quantities. Often, hair can take 2-3 weeks to regrow after waxing. The effects of long-term waxing on the hair follicle are unknown. Theoretically, this modality may reduce regrowth since repeated waxing may destroy follicles. While many kits are offered for use at home, an experienced salon-based operator is able to apply wax quickly to large body surface areas for faster and more successful hair removal.

Although no formal studies have been conducted, the recommendation is that patients using systemic retinoids (ie, isotretinoin [Accutane], acitretin [Soriatane]) refrain from waxing until treatment has been discontinued for a minimum of 6 months to 1 year to avoid skin tearing and scarring. Patients using topical retinoids (ie, tretinoin [Retin-A, Avita], adapalene [Differin]) should also be careful when waxing to avoid injuring the skin. It is recommended that a clearly visible sign be placed in waxing salons warning clients not to wax while using systemic or topical retinoids.
Waxing should not be performed on moles, warts, or irritated, sunburned, or broken skin. Pay special attention to the temperature of wax to avoid burning skin. Adverse effects from waxing include pain, hyperpigmentation, scarring, folliculitis, and ingrown hair pseudofolliculitis. A life-threatening Streptococcus pyogenes and herpes simplexvirus infection of the external genitalia occurred in a 20-year-old diabetic woman following a routine perineal "Brazilian" bikini wax. [13] Additionally, while the pathogenesis is not entirely clear, epilation by waxing more frequently results in follicular lesions (folliculitis) in the proximal extremities despite the fact that distal extremities are waxed more often. [14]
Studies have also found that epilation by waxing induces hair follicles to adopt the growth stage. This can be used to significantly enhance the immune response to transcutaneous DNA immunization by applying plasmid DNA to a recently waxed area of skin. The antibody responses to the topical application of a DNA vaccine post waxing are as strong as those following intramuscular injections. [15, 16]
Threading
Threading is an ancient manual technique, popular in the Middle East, that involves the use of a long twisted loop of thread that is rapidly rotated across the skin. By maneuvering the twisted string, hairs are trapped within the tight entwined coils and are pulled or broken off. Adverse effects from threading include pain, hyperpigmentation, scarring, folliculitis, and ingrown hair pseudofolliculitis. One report suggests threading may be beneficial in patients on isotretinoin therapy, which may cause increased skin fragility. [17]
Abrasives
Abrasives such as pumice stones and devices or gloves made of fine sandpaper work by physically rubbing the hair away from the skin surface. This method can be irritating to skin and is not commonly used for hair removal.
Sugaring
Sugaring is similar to waxing. The sugar mixture is prepared by heating sugar, lemon juice, and water to form a syrup. The syrup is formed into a ball, flattened onto the skin, and then quickly stripped away. Similar to waxing, the hair is removed entirely from the hair shaft; thus, sugaring is an alternative to waxing for people sensitive to wax. Adverse effects from sugaring include pain, hyperpigmentation, scarring, folliculitis, and ingrown hair pseudofolliculitis.
Depilation
Chemical depilatories remove part of the hair shaft and are easy and painless to use. The standard chemical depilatory agents, available in gels, creams, lotions, aerosols, or roll-on forms, are mixtures of thioglycolic acid and sodium or calcium hydroxide. Thioglycolate depilatories work by hydrolyzing and disrupting the disulfide bonds of keratin in hair, causing hair to break apart and allowing it to separate from skin. Common brands of thioglycolate-based depilatory products include Nair, Magic Shave, and Veet. Depilatories are good for use on the legs, bikini line, face, and underarms, and they perform best when hair is at a reasonable length. Before using a depilatory, carefully read the manufacturer's instructions. Test a small site before use to assess for irritation or allergic reactions. Do not use these agents on eyebrows, near mucous membranes, or on broken skin.
Results last up to 2 weeks. [18] Adverse effects include skin irritation, burns, folliculitis, ingrown hairs, pseudofolliculitis, and allergic contact dermatitis to either thioglycolate or fragrances.
Bleaching
Bleaching is not a method of hair removal; however, patients use bleaching as an inexpensive method of disguising the presence of unwanted hair by removing its natural pigment. Common sites for bleaching include the upper lip, beard area, and arms. The active ingredients in over-the-counter bleaching agents are hydrogen peroxide and sulfates. Together, this combination lightens, softens, and oxidizes hair, reducing its noticeability. As with chemical depilatories, perform a test on a small patch of hair to assess for allergic reaction.
The disadvantages of bleaching include skin irritation, temporary skin discoloration, pruritus, and the prominent appearance of bleached hair against tanned or naturally dark skin. Reports exist of generalized urticaria, asthma, syncope, and shock in reaction to the persulfate activator added to boost the effect of hydrogen peroxide bleach.
Temporary Hair Reduction
Eflornithine
Eflornithine (VANIQA) is a topical cream available by prescription in the United States. It has been approved by the US Food and Drug Administration (FDA) for the reduction of unwanted facial hair in women. [19] It is the only topical, nonhormonal, and nonsystematic FDA-approved prescription treatment for women diagnosed with facial hirsutism. Eflornithine is not a hair remover or depilatory; rather, it is a topical cream that decreases the rate of hair growth by inhibiting ornithine decarboxylase, an enzyme in human skin that stimulates hair growth. When this enzyme is blocked by the medication, metabolic activity in the hair follicle decreases and hairs grow more slowly. It has only been studied on the face and the adjacently involved areas under the chin; therefore, it should only be used in those areas. Because eflornithine does not remove hair, it must be used in combination with patients' typical hair removal methods (eg, shaving, waxing, plucking). [20]
Approximately 32% of 594 female subjects showed marked improvement in the reduction of unwanted facial hair, compared with only 8% of control subjects who used placebo. Results are based on prerelease clinical trials in which eflornithine was used for 24 weeks. Improvement often occurred in as few as 4-8 weeks. After discontinuing treatment, facial hair growth returned to pretreatment levels by 8 weeks.
In adults, a thin layer is applied twice daily to affected areas of the face. Do not wash the area for at least 4 hours. Pediatric recommendations have not been established. No interactions have been reported, and contraindications include documented hypersensitivity. Eflornithine may cause temporary redness, stinging, burning or tingling, rash, and folliculitis. It is classified as pregnancy class C, meaning that a fetal risk has been revealed in animal studies but not established or studied in humans; thus, it may be used in a pregnant patient if the benefits outweigh the risk to the fetus.
Eflornithine treatment was found to produce statistically significant improvements in the widespread anxiety and social fears associated with female hirsutism. [21] Additional pharmacological hair removal treatments are available for hair specifically caused by hirsutism. See Hirsutism Medication for more information.
Permanent Hair Reduction
Laser-assisted hair removal
Laser-assisted hair removal is a method available to achieve permanent reduction of unwanted hairs. The various lasers most commonly available for hair removal are the alexandrite laser (755 nm), diode laser (810 nm), and Nd:YAG laser (1064 nm). These lasers target melanin and subsequently produce selective photothermolysis of the hair follicles. The longer wavelengths, such as with the 1064-nm Nd:YAG laser, are safer for darker skin types IV-VI. The risk for adverse events such as dyspigmentation, blistering, crusting, edema, and scarring is greater with darker skin types. [22] See Laser-Assisted Hair Removal for more information.
Generally, the efficacy of laser treatment is greater with light-skinned people who have darker-pigmented hair. [21] Studies have also demonstrated that laser hair removal results in more rapid and complete reduction across different skin types when combined with topical eflornithine. [20, 23] In the same vein, a 2015 study has also demonstrated that the use of an alexandrite laser along with topical licorice is a more effective treatment for idiopathic hirsutism than alexandrite laser alone. [24]
Intense pulsed light sources for hair removal
Intense pulsed light (IPL) sources use the same principle of selective photothermolysis used with lasers to target melanin in hair follicles; however, a noncoherent filtered flashlamp that emits wavelengths ranging from 500-1200 nm is used in this process, rather than using just one wavelength. Different cutoff filters are used to select the appropriate wavelength for each patient; nevertheless, IPL subjects the skin to a wider range of light energies of varying absorption coefficients for the chromophores, which may expose the patient to some unnecessary wavelengths. A disadvantage of IPL is that some machines have capitated maximum energies, which can hinder those patients needing higher energies in order to achieve better results. [25]
Studies have shown that the hair removal efficiency rate (ie, percent of the number of hairs present compared with baseline counts) is best after 1-3 treatments. Adverse effects are minimal, and the hair removal efficiency rate achieved was 76% after a mean of 3.7 treatments and greater than 50% when evaluated more than 12 months following the last treatment. [26]
Compared to the Nd:YAG laser, IPL treatment has a similar hair removal efficacy; however, IPL treatment is more commonly associated with postinflammatory pigmentation. [27, 28] While IPL treatments were found to be more efficacious than those done with a ruby laser, IPL treatments were, again, associated with more adverse reactions—such as pain, discomfort, and crusting—than ruby laser treatments. [28, 29] Nevertheless, treatment with all lasers and IPL sources rarely results in adverse effects. [28]
Laser and IPL devices are also capable of treating a variety of conditions in addition to hair removal, including treatment of vascular and pigmented lesions, warts, wrinkles, and even acne.
Home-use devices have been developed, and some claims to efficacy have been made [30] ; however, randomized, double-blind, controlled studies supporting these claims are uncommon. [8] Additional unsponsored research is needed before accurate comparisons can be made between home-use devices and other methods of hair removal. [31]
Permanent Hair Removal
Electrolysis
Electrolysis, also termed electrology, is an effective method for permanently removing hair, especially in small areas. Electrolysis involves the insertion of a small, fine needle into the hair follicle, followed by the firing of a pulse of electric current that damages and eventually destroys the hair follicle. Multiple treatment sessions are required to achieve a clinically significant result. The two types of electrolysis are galvanic electrolysis (direct current electrolysis) and thermolysis (alternating current electrolysis). [32]
-
Galvanic electrolysis: In galvanic electrolysis, a direct electric current is passed down a needle inserted into the hair follicle, where it acts on tissue saline to produce sodium hydroxide (lye), a caustic agent that destroys the hair bulb and dermal papilla (chemical reaction 2 NaCl + 2 H2 0 = 2 NaOH + H2 + Cl2). During the procedure, the patient holds a metal rod covered with conductive cream or gel or a metal plate attached to a moistened pad. The current (milliamperes) is set by the technician based on the patient's pain threshold, and the duration of the pulse is controlled by how long the technician presses down on the hand or foot pedal. Galvanic electrolysis is slow and may require a minute or more for each hair, including repeated insertions into the follicle. [18]
-
Thermolysis: Thermolysis uses a high-frequency alternating current that is passed down the needle into the follicle. The high-frequency alternating current produces heat in the hair follicle via molecular vibration, resulting in destruction of the hair bulb by thermal—rather than chemical—means. Thermolytic electrolysis is much quicker than galvanic electrolysis, taking 0.02 to 20 seconds for each hair. [18]
Owing to the benefits of thermolytic electrolysis, most modern electrolysis machines use thermolysis or the blend method—a combination of galvanic electrolysis and thermolysis. Unfortunately, no controlled clinical trials have compared these two methods; thus, claims of superiority of one method over the other are based on anecdotal evidence.
Significant evidence indicates that the region of the erector pili muscle insertion is the site of the stem cells responsible for hair regeneration. More research is needed to determine the effects of electrolysis on this region.
Proper electrolysis requires accurate needle insertion technique and appropriate intensities and duration of current. In addition, only anagen-phase hairs should be treated because telogen-phase hairs are believed to be more resistant to damage. Anagen-phase hairs can be easily distinguished from telogen-phase hairs by shaving the area to be treated and, in a few days, treating only the hairs visible on the skin surface since these would be anagen-phase hairs. [18] After electrolysis, the regrowing rate can be up to 40%. [33]
Electronic tweezers and other devices have been developed for home use; however, since hair is not an electric conductor, current cannot be transmitted via hair to the hair bulb. In addition, no published data prove that damage occurs in the hair follicle or that these devices produce permanent hair removal. More likely, these devices represent a means for temporary hair shaft removal similar to waxing or plucking, but do not work well as a means of permanent hair removal. [18]
Important, and potentially permanent, adverse effects of electrolysis include scarring (ie, keloid formation) and postinflammatory hyperpigmentation or hypopigmentation, and these adverse effects are dependent on technician experience as well as the duration and intensity of the current. Pain, a primary adverse effect of electrolysis, can be diminished with the use of new topical anesthetic creams (eutectic mixture of local anesthetics [ELA-Max]) an hour prior to the procedure. This should be performed in a monitored setting and only to limited areas of skin. Maintaining some sensation is desirable because pain is related to the amount of damage to the hair follicle. Other adverse effects include local bacterial and viral infections. The spread of hepatitis or HIV has not been reported with electrolysis. Finally, electrolysis is not safe for patients with pacemakers. [18]
Summary
Temporary and permanent methods of hair removal or reduction are important components in the treatment of patients with unwanted hair. No single method is perfect for all patients. Factors that should be considered when choosing a method of nonlaser hair removal include the underlying medical condition causing excessive hair growth, the size and location of treatment area(s), the desire for temporary versus permanent hair removal, the ability to tolerate pain or discomfort, and the expertise of the technician providing treatment.
-
Man with pseudofolliculitis barbae on his neck.
-
Anatomy of a hair follicle.
-
Woman with hirsutism.
-
Preparation of hot wax for hair removal.





