Overview of Guttate Psoriasis
Guttate psoriasis is characterized by the acute onset of small, 1-10 mm diameter, droplike, erythematous-to-salmon-pink papules, usually with a fine scale, [1] as demonstrated in the images below.
 Guttate psoriasis. The distinctive, acute clinical presentation of guttate psoriasis characterized by small, droplike, 1-10 mm in diameter, salmon-pink papules, usually with a fine scale. Courtesy of Hon Pak, MD.
Guttate psoriasis. The distinctive, acute clinical presentation of guttate psoriasis characterized by small, droplike, 1-10 mm in diameter, salmon-pink papules, usually with a fine scale. Courtesy of Hon Pak, MD.

 Guttate psoriasis. Note characteristic lesions consisting of multiple, discrete, droplike papules with a salmon-pink hue. A fine scale, which is usually absent in early-stage lesions, may be appreciated on the more established ones. Courtesy of Hon Pak, MD.
Guttate psoriasis. Note characteristic lesions consisting of multiple, discrete, droplike papules with a salmon-pink hue. A fine scale, which is usually absent in early-stage lesions, may be appreciated on the more established ones. Courtesy of Hon Pak, MD.
See Psoriasis: Manifestations, Management Options, and Mimics, a Critical Images slideshow, to help recognize the major psoriasis subtypes and distinguish them from other skin lesions.
This variant of psoriasis primarily occurs on the trunk and the proximal extremities, but it may have a generalized distribution. Lesions usually spread centripetally and are monomorphic. New guttate psoriasis lesions continue to develop during the first month of disease; they remain stable during the second month, and the remission begins during the third month. [2] The word guttate is derived from the Latin word gutta, meaning drop.
Guttate psoriasis is more common in individuals younger than 30 years. An upper respiratory tract infection from group A beta-hemolytic streptococci (eg, Streptococcus pyogenes) often precedes the eruption by 2-3 weeks. [3] Streptococcal perianal dermatitis, a superficial bacterial infection of the anus and perianal skin in children, has also been linked with the appearance of guttate psoriasis. [4, 5]
Although episodes may recur, especially those due to pharyngeal carriage of streptococci, isolated bouts have commonly been described. Generally, the disease is self-limiting, but a certain percentage of cases progress to chronic plaque psoriasis.
The sudden appearance of the papular lesions in response to streptococcal infection could either be the first manifestation of psoriasis in a previously unaffected individual or an acute exacerbation of long-standing plaque psoriasis. Uncommonly, guttate psoriasis may be chronic in nature and/or arise in the absence of preceding streptococcal infection. [6] Other triggers include viral infection and medications. [7, 8, 9, 10, 11]
For more information, go to Psoriasis.
Pathophysiology of Guttate Psoriasis
The exact pathophysiologic mechanism in guttate psoriasis is undetermined. Guttate psoriasis is believed to result from an immune reaction triggered by a previous streptococcal infection in a genetically susceptible host. [12]
Studies indicate the importance of chromosome 6 in determining the resultant psoriatic phenotype. HLA-Cw*0602–positive patients are more prone to develop the guttate form. Interactions of HLA-C with killer immunoglobulin–like receptors (KIR) on natural killer cells or natural killer T cells can be deregulated by streptococcal infection. T lymphocytes and cytokines are believed to cause the characteristic inflammatory changes appreciated on histopathologic examination of lesions. [13]
Psoriasis was originally classified as a Th1 disease, but Th17 cells have also been recognized to have an important role. Studies are also proposing a role for antimicrobial peptides and dendritic cells in the pathogenesis of psoriasis. Cathelicidin LL-37 is especially thought to lead to activation of dendritic cells, inducing production of interferons. Elevated levels of the cathelicidin LL-37 have been reported in patients with plaque and guttate psoriasis compared with healthy controls. [14, 15] Levels of inflammatory cytokines interleukin (IL)‒1RA, IL-2, IL-23, and interferon (IFN)‒gamma were also elevated in these patients. There was no significant difference in serum levels of inflammatory cytokines and LL-37 between the plaque type and guttate psoriasis group, but a positive correlation between disease activity and cytokine levels was noted. [14]
An autoimmune phenomenon has also been postulated to underlie guttate psoriasis because some streptococcal products and components have been found to cross-react with normal human epidermis. [16, 17] Electron microscopic studies of guttate psoriasis have shown that mast cell degranulation is an early and constant feature in the evolution of guttate psoriatic lesions. Furthermore, Langerhans cell migration appears to be impaired during an acute episode of guttate psoriasis. [18]
Epidemiology of Guttate Psoriasis
The guttate form of psoriasis is relatively uncommon in the United States, occurring in less than 2% of the psoriatic population. International surveys on the guttate form of psoriasis among patients with psoriasis have found a wide range of prevalences, from 1.6-44%. A 2009 study has shown that the prevalence of psoriasis correlates with the distribution and mortality of streptococcal epidemics. [19]
Race and sex in guttate psoriasis
Guttate psoriasis affects people of all races and affects males and females equally.
Guttate psoriasis and children
Guttate psoriasis is the second most common psoriasis variant in children. [20, 21]
Clinical Presentation of Guttate Psoriasis
Patient history
The onset of the guttate psoriasis skin lesions often is acute, with multiple papules erupting on the trunk and the proximal extremities, in a centripetal fashion. The lesions are often accompanied by slight pruritus.
In most cases of guttate psoriasis, a history of an antecedent streptococcal infection, usually of the upper respiratory tract (eg, pharyngitis or tonsillitis), 2-3 weeks prior to the eruption can be elicited. [22, 23] Perianal streptococcal infections, which often present as chronic pruritus of the anus in children, have also been associated with guttate psoriasis. [4, 5]
Multiple other infectious agents have been implicated, although episodes of guttate psoriasis attributed to them are not as frequent as those attributed to streptococci. Associated organisms include the following:
-
Bacteria -Staphylococcus aureus
-
Fungi -Malassezia, Candida
Drug therapy, including biologic agents, may sometimes precipitate a guttate-type flare. The most commonly implicated medications include lithium, beta-blockers, antimalarial drugs, and nonsteroidal anti-inflammatory drugs. [25] Immunomodulatory drugs such as antiprogrammed cell death-1 (PD-1) inhibitors, infliximab, etanercept, imatinib, and adalimumab have also been reported to cause guttate psoriasis. [26, 27, 28, 29]
A positive family history of psoriasis may be present, and the outcome is generally good. [30, 31]
Physical examination
Examination of the skin reveals characteristic lesions consisting of multiple, discrete, 1-10 mm in diameter, droplike papules with a salmon-pink hue. A fine scale, which is usually absent in early-stage lesions, may be appreciated on the more established ones, as shown in the image below.
Guttate psoriasis. Note characteristic lesions consisting of multiple, discrete, droplike papules with a salmon-pink hue. A fine scale, which is usually absent in early-stage lesions, may be appreciated on the more established ones. Courtesy of Hon Pak, MD.
The lesions of guttate psoriasis appear first on the trunk and the proximal extremities, progressing in a centripetal fashion. Lesions are commonly monomorphic and at the same stage of evolution. They may sometimes spread to involve the face, the ears, and the scalp. The palms and the soles are rarely affected. Nail changes in the form of pits, ridges, and the oil-drop sign, which are characteristic of chronic psoriasis, may be absent
Additional findings may include pharyngeal or perianal erythema in cases associated with acute streptococcal infections. Ledoux et al emphasize a careful examination, including the perianal region, in children being examined for guttate psoriasis. [5]
Etiology of Guttate Psoriasis
The etiology of guttate psoriasis is not well understood. Genetic as well as environmental factors have been implicated in its pathogenesis.
Genetic factors
As in other types of psoriasis, genetic predisposition seems to play an important role in the development of an acute guttate psoriasis flare. [32]
Compared with control populations, a significant excess of HLA-BW17 has been found in patients with guttate psoriasis. Other researchers have found an increase in HLA-B13 positivity. Moreover, the inability to produce normal amounts of antibody to streptolysin-O by HLA-B13–positive individuals might explain their high prevalence of guttate psoriasis.
Interestingly, an increased prevalence of HLA-Cw6*0602 has also been found. These patients experience psoriasis at markedly higher rates than control subjects. [33, 34]
Thus far, psoriasis is the only disease associated with HLA-C gene expression. [16] HLA-B*57 and DRB1*07 have also been detected with increased frequency in psoriasis patients. [35]
Proteomic and immunohistochemistry studies have demonstrated that guttate psoriasis and chronic plaque psoriasis are phenotypically distinguishable in their protein expression patterns. [36, 37]
Streptococcal infection and guttate psoriasis
The association of guttate psoriasis with streptococcal infection has been recognized for more than 50 years. As many as 80% of patients with guttate psoriasis have clinical or laboratory evidence of streptococcal infection, usually in the form of tonsillopharyngitis. [38]
The streptococcal serotypes in these patients are similar to those seen in the general population. Aside from group A streptococci, Lancefield groups C and G streptococci have also been related to guttate psoriasis. [39, 40] Although specific Lancefield groups have been associated with psoriasis, no association with any specific M serotype has been discovered.
A number of cases in children have also been triggered by streptococcal perianal cellulitis. Presumably, absorption of streptococcal by-products occurs across the mucosa, as with pharyngeal infections.
Unfortunately, although the association is definite, details regarding the exact mechanism by which streptococcal infection influences the formation of the psoriatic lesions are still largely theoretical.
Lotus et al demonstrated that guttate psoriasis patients expressing the HLA-Cw*0602 allele were twice as likely to have positive streptococcal throat cultures. [17]
T lymphocytes and guttate psoriasis
Histologic studies of early-stage psoriatic skin lesions reveal that the activation of T lymphocytes, endothelial cells, and macrophages precedes epidermal proliferation. [41] The increased proliferation of the epidermal layer characteristic of psoriasis might be induced by activated T lymphocytes via the production of cytokines. Indeed, group A streptococcal antigen–specific T lymphocytes, which secrete high levels of gamma interferon, can be consistently isolated from guttate psoriatic skin lesions.
Consistent with the role of T lymphocytes is the concept of superantigenic stimulation by certain streptococcal components or products. Examples of superantigens produced by group A beta-hemolytic streptococci are streptococcal pyogenic exotoxins (SPE) types A, B, and C; a 22-kd pepsin fragment of M type-5 protein; S pyogenes– derived cytoplasmic membrane–associated protein (CAP); and secretion-type CAP (SCAP). [42]
In general, unlike a conventional peptide antigen, a superantigen stimulates T cells almost solely through the beta variable (Vβ) portion of the T-cell receptor and induces an expansion of both CD4+ and CD8+ T cells. Therefore, an increased representation of Vβ2+ T lymphocytes, such as that in both the epidermis and the dermis of guttate psoriatic lesions, compared with that of lymphocytes from the peripheral blood of the same patients and lymphocytes in normal skin, strongly suggests that T-cell stimulation by a superantigen is probably involved. [43]
It appears that patients with guttate psoriasis respond to group A streptococcal antigen presentation in the same way as nonpsoriatic patients. However, the magnitude of their response is much greater. [3]
The fungus Malassezia furfur has been associated with the appearance of psoriatic lesions, but a causative role has not been proven. A study by Aydogan et al showed that the prevalence of M furfur was similar in patients with psoriasis and those without. However, in psoriatic patients with M furfur, cytokines important in the regulation of helper T-lymphocytes (Th2 cells), such as IL-4, IL-10, and IL-13, were markedly downregulated as compared to normal controls and psoriatic patients without M furfur. Thus, cytokine dysregulation appears to be important in the development of psoriasis in this patient population. [44]
Autoantibodies in guttate psoriasis
Immunoblotting has demonstrated intense antistreptococcal antibody activity in the sera of patients with guttate psoriasis. Immunoglobulin G (IgG) antibodies against 3 different S pyogenes proteins—namely, a 60-, a 70-, and a 14-kd antigen—have been identified. Indirect immunofluorescence studies of these antibodies showed that they react only with autologous skin in patients with guttate psoriasis and not with normal skin or lesional skin from patients who do not have psoriasis. [39, 45]
Autoantibodies in psoriatic sera may recognize certain structures in the transformed keratinocytes of affected psoriatic skin. These autoantibodies cross-react with streptococcal antigens. Cross-reaction has been demonstrated on immunofluorescent microscopy by using a monoclonal antibody (mAb 111-15504) to group A streptococci, which does not cross-react with antigens in normal human skin. These antigens were associated with class 1M protein and were mostly concentrated in the dermal papillae around the capillaries and inside the cells of the epidermal basal layer.
Immunologic changes
Epidermal Langerhans cell migration is inhibited in early-onset, plaque-type psoriasis. Altered Langerhans cell migration has recently also been demonstrated in patients with guttate psoriasis. A small study revealed decreased migration compared with healthy controls. In patients with resolved guttate psoriasis, the epidermal Langerhans cell migration was normal. [18]
Vaccination
Over the past years, concerns have been raised about vaccination as a possible trigger for new onset of psoriasis or exacerbation of existing disease. Several small studies have reported an association between influenza vaccination in the 2009-2010 flu season and psoriasis. Most cases presented as mixed/guttate psoriasis. [46] More studies are necessary for further evaluation, but a study by Sbidian et al suggested a very low incidence of associated cases and emphasized the relative safety and relevance of vaccinations. [47]
Drugs
Tumor necrosis factor blocker therapy has been associated with the development or worsening of guttate psoriasis. [26, 27, 28, 48]
Diagnosis of Guttate Psoriasis
Diagnostic considerations
A careful history should be taken to exclude certain drugs, such as beta-blockers and lithium, which may cause an eruption similar to that of guttate psoriasis. Viral exanthema should also be considered.
Especially in patients with palmar and plantar lesions, serologic analysis should be performed to exclude secondary syphilis. Skin biopsy is probably the single most useful diagnostic test if the clinical diagnosis is not certain.
Histopathologic findings and severity do not correlate with the clinical severity or the Psoriasis Severity Index. [49]
Differential diagnosis
The differential diagnosis of guttate psoriasis includes the following:
Serology
Levels of antibodies to streptolysin O, hyaluronidase, and deoxyribonuclease B may be elevated in more than half the patients with guttate psoriasis. Significant elevations of antistreptococcal M6 protein have been documented. Routine screening in asymptomatic patients is controversial. Patients with symptoms suggestive of a streptococcal infection should undergo appropriate laboratory testing.
Cultures
A bacteriologic culture of the throat or the perianal area may be helpful to isolate the organism in selected cases. Throat culture continues to be the criterion standard to diagnose streptococcal pharyngitis.
Urinalysis
Urine results are usually negative. Detection of blood and protein on urinalysis could suggest a rare case associated with a concomitant poststreptococcal acute glomerulonephritis. However, reported cases have failed to prove association of psoriasis and poststreptococcal renal disease. [50]
Histologic Findings
Because the clinical appearance is so characteristic, biopsy is seldom necessary to confirm the diagnosis of guttate psoriasis. Histopathologic changes may not be diagnostic when samples of early-stage papules are obtained at biopsy.
The epidermis shows hyperplasia and small foci of parakeratosis with an absence of the granular layer. Dermal changes consisting of capillary dilatation and edema may be more pronounced, and an infiltrate consisting of lymphocytes and macrophages is seen mostly in the upper dermis. A few polymorphonuclear leukocytes may be found at all levels. Early lesions exhibit more inflammation and less acanthosis, and very early lesions can show normal basket-weave orthokeratosis overlying parakeratotic changes.
In fully developed guttate lesions, vacuolated keratinocytes eventually disappear, leaving areas of agranulosis with overlying parakeratosis. Degenerated polymorphonuclear leukocytes on an otherwise orthokeratotic stratum corneum may be the earliest presentation of Munro microabscesses.
The term squirting papillae has been used to describe a phenomenon wherein neutrophils are discharged from the papillary capillaries, resulting in collections of neutrophils in association with parakeratotic mounds, as demonstrated in the image below. In some cases, marked exudation may lead to the formation of the highly diagnostic spongiform pustule of Kogoj, which is seen in psoriasiform variants. [21, 51] (See the images below regarding histologic findings.)
Histopathologic findings and severity do not correlate with the clinical severity or Psoriasis Severity Index. [49]
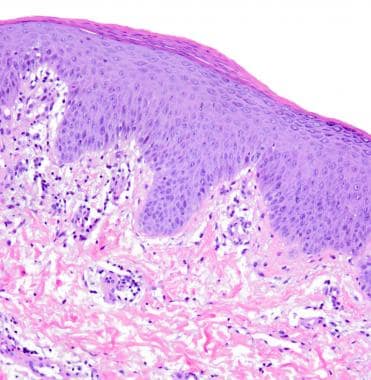 Guttate psoriasis. Superficial perivascular, predominantly lymphocytic infiltrate with minimal dermal edema. The overlying epidermis has psoriasiform hyperplasia. Notice how the stratum granulosum (on right) disappears underneath the mound of parakeratosis in the stratum corneum (in center) (hematoxylin and eosin, 100X). Courtesy of Cary Chisholm, MD.
Guttate psoriasis. Superficial perivascular, predominantly lymphocytic infiltrate with minimal dermal edema. The overlying epidermis has psoriasiform hyperplasia. Notice how the stratum granulosum (on right) disappears underneath the mound of parakeratosis in the stratum corneum (in center) (hematoxylin and eosin, 100X). Courtesy of Cary Chisholm, MD.
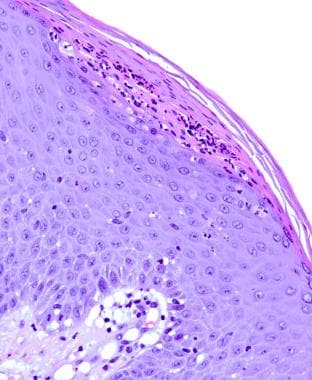 Guttate psoriasis. A Munro microabscess is present in the stratum corneum, underneath parakeratosis (in center). Neutrophils can be seen migrating through the psoriasiform epidermis, towards the microabscess (the so-called squirting papillae) (hematoxylin and eosin, 200X). Courtesy of Cary Chisholm, MD.
Guttate psoriasis. A Munro microabscess is present in the stratum corneum, underneath parakeratosis (in center). Neutrophils can be seen migrating through the psoriasiform epidermis, towards the microabscess (the so-called squirting papillae) (hematoxylin and eosin, 200X). Courtesy of Cary Chisholm, MD.
Overview of Treatment
Usually, guttate psoriasis spontaneously resolves within a few weeks to months without treatment. In general, there is no firm consensus on specific treatment algorithms. [52]
As in other conditions, the choice of treatment should be tailored to the individual. Should guttate psoriasis result as a reaction to a new medication, removal of the offending medication may be warranted if other treatments do not ameliorate the symptoms.
Simple reassurance and emollients may be sufficient care. Topical steroids can be effective but their application can be cumbersome, especially when the eruption is extensive, as it is in most cases of guttate psoriasis.
A guideline summary from the American Academy of Dermatology, Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics, may be helpful. [53]
Corticosteroids
Topical corticosteroids are a critical addition to the successful treatment of many guttate psoriasis patients. The mechanisms believed to provide benefit include anti-inflammatory, antiproliferative, immunosuppressive, and vasoconstrictive effects.
Seven potency classes of corticosteroids exist, and the agent prescribed should be selected from a class appropriate to the location of disease. Lower-potency corticosteroids should be used for face and intertriginous areas, areas of thinned skin, and on infants. Higher-potency corticosteroids are generally acceptable in adults with lesions elsewhere on the body. Thick plaques may require therapy with the most potent corticosteroids. [54]
Antimicrobials
Because of the clear association with streptococcal infection seen in most cases of guttate psoriasis, laboratory testing in patients with a known history or symptoms suggestive of streptococcal infections and antibiotic therapy have been proposed. [55]
However, the efficacy of antibiotics in the management of psoriasis has been questioned and data are limited. [50] Dogan et al and Owen et al found no statistically significant improvement in streptococcal guttate psoriasis after treatment with penicillin or erythromycin or with no treatment. [56, 57] Nevertheless, some experts have used empiric antimicrobial therapy in streptococcal-related guttate psoriasis, with the following agents [58] :
-
Cephalexin (Keflex)
-
Amoxicillin
-
Penicillin VK
-
Erythromycin
-
Rifampin
Azithromycin, which is commonly prescribed for community-acquired pneumonia, is likewise an option.
Phototherapy
The clearance of guttate lesions can be accelerated by judicious exposure to sunlight or by a short course of either broadband ultraviolet B (UV-B) or narrow-band UV-B phototherapy. [59, 60, 61] Koek et al reported that UV-B phototherapy administered to psoriasis patients in home-based setting was as effective as that administered as an outpatient treatment, with significantly lower patient burden. [62]
More resistant cases may benefit from oral psoralen plus exposure to ultraviolet A radiation (PUVA). The suit PUVA technique has been used in this setting. [59]
Aside from the usual mechanisms by which UV light is believed to exert its beneficial effects in psoriasis, a specific fibrosing response to PUVA via increased mast cell activation has been observed in guttate psoriasis and might underlie the mechanism of action behind UV-induced resolution of the lesions.
However, considering the developments in photomedicine over the last several years, particularly regarding the clinical efficacy of narrowband UV-B phototherapy, versus the risk of cutaneous malignancies with PUVA, treatment with narrowband UV-B is favored over treatment with PUVA.
Guidelines on the management and treatment of psoriasis with phototherapy were released in September 2019 by the American Academy of Dermatology and the National Psoriasis Foundation. [63]
Narrowband ultraviolet B phototherapy
Phototherapy using narrowband ultraviolet B (NB-UVB) is recommended as monotherapy for adults with plaque psoriasis.
For adults with generalized plaque psoriasis, the recommended NB-UVB phototherapy starting dose should be based on the minimal erythema dose or it should be determined based on a fixed-dose or skin-phototype protocol.
For adults with generalized plaque psoriasis, a treatment phase of thrice-weekly dosing of NB-UVB phototherapy is recommended.
For adults with psoriasis, treatment with short-term psoralen plus ultraviolet A (PUVA) monotherapy is more effective than NB-UVB.
Owing to its increased safety, higher convenience, and lower cost, NB-UVB is preferred over PUVA monotherapy for psoriasis in adults, even though it is less effective.
In adults with generalized plaque psoriasis, NB-UVB is recommended over broadband ultraviolet B (BB-UVB) monotherapy.
Treatment with NB-UVB monotherapy is recommended for guttate psoriasis patients, regardless of their age.
For appropriate patients with generalized plaque psoriasis, home-based NB-UVB phototherapy is recommended as an alternative to in-office NB-UVB phototherapy.
Treatment with NB-UVB phototherapy is recommended for pregnant patients who have guttate psoriasis or generalized plaque psoriasis.
As a measure to possibly improve efficacy, NB-UVB phototherapy can be safely augmented with concomitant topical therapy using retinoids, vitamin D analogues, and corticosteroids.
Oral retinoids can be combined with NB-UVB phototherapy in appropriate patients with generalized plaque psoriasis if they have not responded adequately to monotherapy.
Owing to an increased risk of developing skin cancer, long-term combination therapy with NB-UVB and cyclosporine is not recommended for adults with generalized plaque psoriasis.
Apremilast combined with NB-UVB phototherapy can be considered for adult patients with generalized plaque psoriasis if they have not responded adequately to monotherapy.
To reduce the risk of genital skin cancer, all patients receiving NB-UVB phototherapy should be provided genital shielding.
To reduce the risk of ocular toxicity, all patients receiving NB-UVB phototherapy should be provided eye protection with goggles.
Owing to the risk of photocarcinogenesis, use caution when administering NB-UVB phototherapy to patients with a history of melanoma or multiple nonmelanoma skin cancers, arsenic intake, or prior exposure to ionizing radiation.
Folate supplementation is recommended for females of childbearing age who are receiving NB-UVB phototherapy.
To maintain the clinical response from NB-UVB phototherapy, maintenance therapy can be considered.
BB-UVB phototherapy
In adults with generalized plaque psoriasis, BB-UVB phototherapy is recommended as monotherapy if NB-UVB is not available.
In adults with generalized plaque psoriasis, BB-UVB monotherapy is considered less efficacious than NB-UVB or oral PUVA monotherapy.
Monotherapy with BB-UVB may be considered for adults with guttate psoriasis.
To reduce the risk of genital skin cancer, all patients being offered BB-UVB phototherapy should be provided with genital shielding.
To reduce the risk of ocular toxicity, all patients receiving BB-UVB phototherapy should be provided eye protection with goggles.
Owing to the risk of photocarcinogenesis, use caution when administering BB-UVB phototherapy to patients with a history of melanoma or multiple nonmelanoma skin cancers, arsenic intake, or prior exposure to ionizing radiation.
Combination therapy with acitretin and BB-UVB can be considered in adults with generalized plaque psoriasis.
Targeted UVB phototherapy
The recommended targeted UVB phototherapy for adults with localized plaque psoriasis (< 10% body surface area), for individual plaque psoriasis lesions, or for patients with more extensive disease includes excimer 308-nm laser, excimer 308-nm light, and targeted NB-UVB 311- to 313-nm light.
For maximal efficacy, the recommended treatment frequency for targeted UVB phototherapy in adults with localized plaque psoriasis is 2-3 times per week, rather than once every 1-2 weeks.
In adults with localized plaque psoriasis, the initial dose of targeted UVB phototherapy is based on the minimal erythema dose or by a fixed-dose or skin-phototype protocol.
For treating localized plaque psoriasis in adults, the most effective targeted UVB phototherapy is excimer 308-nm laser, followed by excimer 308-nm light, followed by localized NB-UVB 311- to 312-nm light.
For adults with plaque psoriasis (including palmoplantar psoriasis), a recommended targeted UVB phototherapy includes excimer 308-nm laser and excimer 308-nm light.
Treatment of plaque psoriasis in adults with excimer 308-nm laser may be combined with topical steroid therapy.
A recommended targeted UVB phototherapy treatment for adults with scalp psoriasis is excimer 308-nm laser.
PUVA therapy
In the treatment of localized plaque psoriasis in adults, particularly those with palmoplantar psoriasis or palmoplantar pustular psoriasis, topical phototherapy with PUVA is deemed superior to NB-UVB 311- to 313-nm light.
A recommended treatment for psoriasis in adults is oral PUVA.
A recommended treatment for moderate-to-severe psoriasis in adults is bath PUVA.
Photodynamic therapy
Photodynamic therapy with either aminolevulinic acid or methyl aminolevulinate is not recommended for adults with localized psoriasis, including the palmoplantar variety or nail psoriasis.
Grenz ray, climatotherapy, visible light, Goeckerman, and pulsed-dye laser therapies
Evidence is insufficient to recommend grenz ray therapy (long-wavelength ionizing radiation) for the treatment of psoriasis.
Sufficient evidence exists to recommend climatotherapy (temporary or permanent relocation geographically) for the treatment of psoriasis.
Evidence is insufficient to recommend the use of visible light (blue or red) as a more effective treatment for psoriasis, except in nail psoriasis.
Sufficient evidence exists to recommend Goeckerman therapy (coal tar in combination with UVB phototherapy) for the treatment of psoriasis.
Pulsed-dye laser can be considered for nail psoriasis.
Additional Therapies
Vitamin D analogues are also used for psoriasis. Randomized, placebo-controlled and double-blind studies have shown a marked improvement in disease as compared with response to other treatments. [54] Other therapies that have been reported in the literature include fish oil–derived n -3 fatty acid infusion, topical retinoids, and tar. [52, 54]
Should guttate psoriasis prove resistant to the above therapies, it may develop into a chronic plaque psoriasis, which may require systemic treatment with medications such as cyclosporine, acitretin, methotrexate, or a biologic agent.
Surgical Care
Although unproven by large controlled clinical trials, tonsillectomy for patients with recurrent or chronic guttate psoriasis associated with poststreptococcal tonsillitis may be considered. [64, 65, 66]
Complications
Physicians should watch for possible hypersensitivity reactions to the above-mentioned antimicrobials, especially to penicillin. If hypersensitivity is suspected, the drug should be immediately discontinued. Patients who are hypersensitive to penicillin generally do well on erythromycin. Cephalosporins can also cover streptococci, but some cross-sensitivity with penicillins has been documented.
Areas of the skin that have been treated with high-potency topical steroids for long periods may show some atrophy, telangiectases, and hypopigmentation. Shifting to a preparation with a lower potency or to another treatment modality should be considered.
Patients on PUVA may experience a number of adverse effects, such as nausea and vomiting. These effects are sometimes remedied by taking psoralen pills after a meal. The psoralen-induced photosensitivity persists up to 24 hours after administration of the drug. Patients should be adequately informed about the need to wear protective lenses and to avoid sun exposure during this period.
Patient Education
Patients should be advised to minimize all forms of skin trauma, such as scratching or vigorous rubbing, which may lead to new psoriatic lesions on previously unaffected areas (Koebner phenomenon).
Patients should be advised to seek medical attention promptly for sore throat and other possible streptococcal infections. Early detection and treatment of such infections may prevent an acute flare of the skin disease.
For patient education information, see Guttate Psoriasis, What Is Psoriasis?, Types of Psoriasis, Understanding Psoriasis Medications, and Nail Psoriasis.
Prognosis in Guttate Psoriasis
Guttate psoriasis is a nonfatal eruption that either can run a limited course over several weeks to a few months, may recur, or can develop into the chronic plaque-type of psoriasis. Scarring is not a problem. Previously affected areas may show postinflammatory hypopigmentation or postinflammatory hyperpigmentation.
Data available on the prognosis of guttate psoriasis are sparse. Although guttate psoriasis often has a short-lived course, it may also represent the initial stage of chronic plaque-type psoriasis. Progression rates to chronic plaque psoriasis, reported in small studies, have ranged from one third to approximately two thirds (68%) of patients with gutatte psoriasis. [67, 68]
In a study of 15 patients, the probability of an individual developing chronic psoriasis within 10 years of a single episode of acute guttate psoriasis was suggested to be about 1 in 3, although further studies with larger numbers of patients are needed to more accurately determine the risk. [67]
Like other forms of psoriasis, guttate psoriasis tends to improve during the summer and worsen during the winter. Once an episode of acute guttate psoriasis has cleared, many patients will have limited or no evidence of psoriasis for prolonged periods.
Questions & Answers
Overview
What is the pathophysiology of guttate psoriasis?
What is the prevalence of guttate psoriasis in the US?
What are the demographic predilections in the prevalence of guttate psoriasis?
What are the signs and symptoms of guttate psoriasis?
Which organisms are associated with guttate psoriasis?
What are medical causes of guttate psoriasis?
Which physical findings are characteristic of guttate psoriasis?
What causes guttate psoriasis?
What is the role of genetics in the etiology of guttate psoriasis?
What is the role of streptococcal infection in the etiology of guttate psoriasis?
What is the role of T lymphocytes in the pathophysiology of guttate psoriasis?
What is the role of autoantibodies in the pathophysiology of guttate psoriasis?
What are implications of immunologic changes in the etiology of guttate psoriasis?
What is the role of vaccines in the etiology of guttate psoriasis?
What is the role of tumor necrosis factor blockers in the etiology of guttate psoriasis?
How is guttate psoriasis diagnosed?
What is included in the differential diagnoses of guttate psoriasis?
What is the role of serology in the evaluation of guttate psoriasis?
What is the role of culture in the diagnosis of guttate psoriasis?
What is the role of urinalysis in the evaluation of guttate psoriasis?
What are histologic features of guttate psoriasis?
What are the treatment options for guttate psoriasis?
What is the role of corticosteroids in the management of guttate psoriasis?
What is the role of lab testing in the management of guttate psoriasis?
What is the role of empiric antimicrobial therapy in the treatment of guttate psoriasis?
What is the role of phototherapy in the management of guttate psoriasis?
What is the role of vitamin D in the management of guttate psoriasis?
When are systemic medications indicated for the treatment of guttate psoriasis?
What is the role of surgery in the treatment of guttate psoriasis?
What are complications associated with guttate psoriasis?
What is included in patient education about guttate psoriasis?
What is the prognosis of guttate psoriasis?
-
Guttate psoriasis. The distinctive, acute clinical presentation of guttate psoriasis characterized by small, droplike, 1-10 mm in diameter, salmon-pink papules, usually with a fine scale. Courtesy of Hon Pak, MD.
-
Guttate psoriasis. Courtesy of Hon Pak, MD.
-
Guttate psoriasis. Note characteristic lesions consisting of multiple, discrete, droplike papules with a salmon-pink hue. A fine scale, which is usually absent in early-stage lesions, may be appreciated on the more established ones. Courtesy of Hon Pak, MD.
-
Guttate psoriasis. Superficial perivascular, predominantly lymphocytic infiltrate with minimal dermal edema. The overlying epidermis has psoriasiform hyperplasia. Notice how the stratum granulosum (on right) disappears underneath the mound of parakeratosis in the stratum corneum (in center) (hematoxylin and eosin, 100X). Courtesy of Cary Chisholm, MD.
-
Guttate psoriasis. A Munro microabscess is present in the stratum corneum, underneath parakeratosis (in center). Neutrophils can be seen migrating through the psoriasiform epidermis, towards the microabscess (the so-called squirting papillae) (hematoxylin and eosin, 200X). Courtesy of Cary Chisholm, MD.
Tables

What would you like to print?
- Overview of Guttate Psoriasis
- Pathophysiology of Guttate Psoriasis
- Epidemiology of Guttate Psoriasis
- Clinical Presentation of Guttate Psoriasis
- Etiology of Guttate Psoriasis
- Diagnosis of Guttate Psoriasis
- Serology
- Cultures
- Urinalysis
- Histologic Findings
- Overview of Treatment
- Corticosteroids
- Antimicrobials
- Phototherapy
- Additional Therapies
- Surgical Care
- Complications
- Patient Education
- Prognosis in Guttate Psoriasis
- Questions & Answers
- Show All
- Media Gallery
- References