Overview
Type 1 neurofibromatosis has a variable phenotypic expression that includes dermatologic manifestations. Some patients may have a primarily cutaneous expression, while others may have life-threatening or severely disfiguring complications.
Neurofibromatosis is an autosomal dominant disorder that affects the bone, nervous system, soft tissue, and skin. At least 8 different clinical phenotypes of neurofibromatosis have been identified, and they are linked to at least two genetic disorders. Clinical manifestations increase over time. Neurologic problems and malignancy development may supervene.
A neurocutaneous condition, neurofibromatosis can involve almost any organ system. Thus, the presenting signs and symptoms may vary widely. Two major subtypes exist: type 1 neurofibromatosis, also known as von Recklinghausen neurofibromatosis, which is the most common subtype and is referred to as peripheral neurofibromatosis, and type 2 neurofibromatosis, which is referred to as central neurofibromatosis. These descriptions are not especially accurate, because type 1 neurofibromatosis often has central features. This article will examine the dermatologic manifestations of type 1 neurofibromatosis.
Presentation
Neurofibromatosis is often diagnosed because of unusual pigmentary patterns. Café au lait macules—irregularly shaped, evenly pigmented, brown macules—are often present at birth, but they increase in number during the first few years of life. [1] Neurofibromas form in late adolescence, most commonly in the skin. Patients may report cutaneous discoloration or disfigurement or more serious physical symptoms (eg, pain caused by neurofibromas, pathologic fractures, hypertensive headaches due to pheochromocytoma).
Café au lait spots
Most individuals with neurofibromatosis have 6 or more café au lait spots that are 1.5 cm or greater in diameter. In young children, 5 or more café au lait macules greater than 0.5 cm in diameter are suggestive of neurofibromatosis, and further diagnostic workup should be pursued. Less than 1% of healthy children have 3 or more such spots, although 1 or 2 café au lait macules are commonly encountered in healthy individuals without disease. (See the images below.)
 A light-brown hyperpigmented lesion is noted on the arm and has a smooth border. Most persons affected by neurofibromatosis type 1 have such café-au-lait macules.
A light-brown hyperpigmented lesion is noted on the arm and has a smooth border. Most persons affected by neurofibromatosis type 1 have such café-au-lait macules.
 Neurofibromas are noted on the right arm and right chest in association with a café-au-lait macule on the arm. The association of these lesions is a useful clue to the diagnosis of neurofibromatosis type 1.
Neurofibromas are noted on the right arm and right chest in association with a café-au-lait macule on the arm. The association of these lesions is a useful clue to the diagnosis of neurofibromatosis type 1.
 The café au lait macules of neurofibromatosis have an even tan color and a smooth border. The presence of neurofibromas in the upper right corner of the photo as well as the lower left corner make a diagnosis of neurofibromatosis almost certain.
The café au lait macules of neurofibromatosis have an even tan color and a smooth border. The presence of neurofibromas in the upper right corner of the photo as well as the lower left corner make a diagnosis of neurofibromatosis almost certain.
Axillary freckling
Axillary freckling (as well as freckling on the perineum), known as the Crowe sign, is a helpful diagnostic feature in neurofibromatosis (see the image below). Axillary freckling and inguinal freckling often develop during puberty. The development of freckles often follows the development of café au lait macules, but it precedes the development of neurofibromas. Eighty percent of type 1 neurofibromatosis patients have freckling of the axillae. Areas of freckling and regions of hypertrichosis occasionally overlay plexiform neurofibromas.
 Axillary freckling is also known as the Crowe sign. This pigmentary change is seen in about one third of individuals affected with neurofibromatosis type 1, but it can also be seen in several other conditions.
Axillary freckling is also known as the Crowe sign. This pigmentary change is seen in about one third of individuals affected with neurofibromatosis type 1, but it can also be seen in several other conditions.
Neurofibromas
Neurofibromas are the most common benign tumor of type 1 neurofibromatosis. These tumors are composed of Schwann cells, fibroblasts, mast cells, and vascular components. They can develop at any point along a nerve. Three subtypes of neurofibroma exist: cutaneous, subcutaneous, and plexiform. Cutaneous lesions and subcutaneous lesions are circumscribed; neither is specific for type 1 neurofibromatosis. These nodules may be brown, pink, or skin colored. They may be soft or firm to the touch, and they may have the pathognomonic buttonhole invagination when pressed with a finger. (See the images below.)
 Neurofibromas increase in number and size over time. Soft pedunculated neurofibromas are shown here on the arm of a woman with neurofibromatosis type 1.
Neurofibromas increase in number and size over time. Soft pedunculated neurofibromas are shown here on the arm of a woman with neurofibromatosis type 1.
 Neurofibromas are soft on palpation, and they may exhibit a buttonhole sign, whereby they can be pushed deeper into the dermis.
Neurofibromas are soft on palpation, and they may exhibit a buttonhole sign, whereby they can be pushed deeper into the dermis.
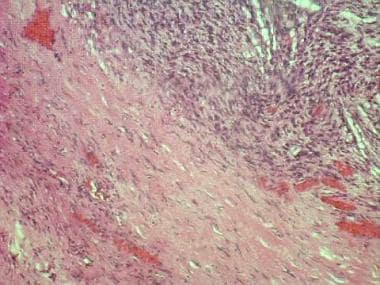
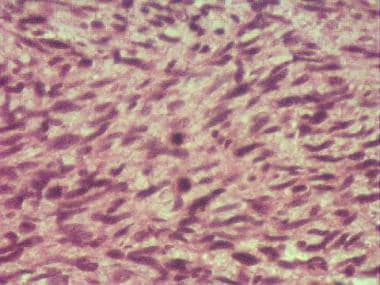
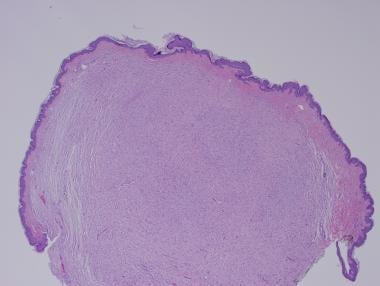 Neurofibromas are often pedunculated and are composed of spindled cells with wavy nuclei embedded in an acidophilic stroma. (Hematoxylin and Eosin stained sections; original magnification 20x).
Neurofibromas are often pedunculated and are composed of spindled cells with wavy nuclei embedded in an acidophilic stroma. (Hematoxylin and Eosin stained sections; original magnification 20x).
Plexiform neurofibromas are noncircumscribed, thick, and irregular, and they can cause disfigurement by entwining important supportive structures. The plexiform subtype is specific for type 1 neurofibromatosis. [2]
Although neurofibromas are most common tumor associated with type 1 neurofibromatosis, other neural tumors such as schwannomas, granular cell tumors, and malignant peripheral nerve sheath tumors may be encountered. [3] See the histology images below.
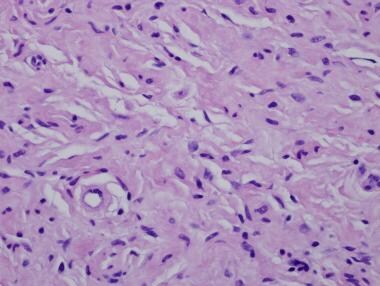 Neurofibromas are composed of delicate spindle cells in a loose stroma. (Hematoxylin and Eosin; original magnification 400x)
Neurofibromas are composed of delicate spindle cells in a loose stroma. (Hematoxylin and Eosin; original magnification 400x)
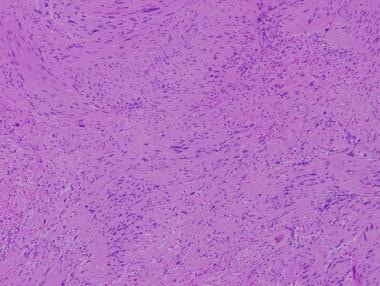 Schwannomas (neurilemmomas) are benign tumors that develop along the course of nerves. Spindle cells may cluster in "stacks" that create palisades. Two adjacenet stacks with intervening Schwann cell cytoplasm are know as Verocay bodies. (Hematoxylin and eosin stained sections; original magnification 200x).
Schwannomas (neurilemmomas) are benign tumors that develop along the course of nerves. Spindle cells may cluster in "stacks" that create palisades. Two adjacenet stacks with intervening Schwann cell cytoplasm are know as Verocay bodies. (Hematoxylin and eosin stained sections; original magnification 200x).
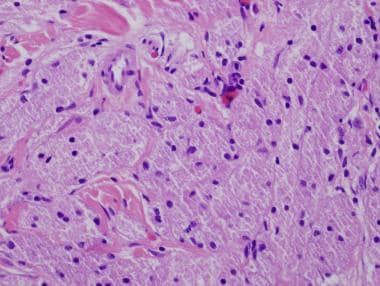
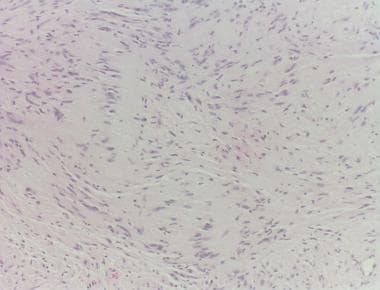 Schwannomas have areas with spindle shaped schwan cells (Antoni A areas) and intervening stroma (Antoni B areas). (Hematoxylin and eosin stain; original magnification 400x)
Schwannomas have areas with spindle shaped schwan cells (Antoni A areas) and intervening stroma (Antoni B areas). (Hematoxylin and eosin stain; original magnification 400x)
 Sheets of spindled cells are depicted in this malignant schwannoma. Malignant degeneration should be expected in a painful or rapidly enlarging tumor in any patient with neurofibromatosis.
Sheets of spindled cells are depicted in this malignant schwannoma. Malignant degeneration should be expected in a painful or rapidly enlarging tumor in any patient with neurofibromatosis.
 High-power view of a malignant schwannoma reveals sheets of hyperchromatic spindle cells with pleomorphic nuclei.
High-power view of a malignant schwannoma reveals sheets of hyperchromatic spindle cells with pleomorphic nuclei.
 Granular cell tumors are also known as granular cell schwannomas. They often involve the mouth but may occur anywhere on the skin or in the soft tissues. Tumor cells are polygonal and have unique eosinophilic granules in the cytoplasm. (hematoxylin and eosin stained sections; original magnification 400x).
Granular cell tumors are also known as granular cell schwannomas. They often involve the mouth but may occur anywhere on the skin or in the soft tissues. Tumor cells are polygonal and have unique eosinophilic granules in the cytoplasm. (hematoxylin and eosin stained sections; original magnification 400x).
Abnormalities in the neurofibromin gene in the pericentromeric region of chromosome 17 are associated with type I neurofibromatosis. Microarray analysis has identified both up- and down-regulation of multiple genes that play a role in tumorigenesis.
Extensive facial tumors may lead to hemifacial hypertrophy, which can be mitigated by facial aesthetic unit remodeling.
Exciting work is being done to look at how personalized medicine may be used to treat various aspects of neurofibromatosis type 1. [4] Next-generation sequencing has identified low-grade optic gliomas that exhibit NF1 gene inactivation and exhibit changes in PTEN and BRAF gene function. These findings suggest that subsets of patients may be identified for specific interventional therapies in the near future.
Lipomatous neurofibromas are associated with neurofibromatosis type 1. Lipomatous neurofibromas are mainly associated with larger tumors. Expression of leptin may contribute to the development of cutaneous neurofibromas. [5]
Lisch nodules
Lisch nodules are melanocytic hamartomas of the iris and are an important sign of type 1 neurofibromatosis. They may be difficult to detect on routine examination, but the dermatoscope may help detect early lesions, especially in children with multiple café au lait macules and no family history of neurofibromatosis. [6]
Treatment
Neurofibromas can be excised and laser treatment can be used to treat pigmentary abnormalities. A European patient community survey reveals that the visible stigma and unaesthetic aspect of some lesions in type I neurofibromatosis may significantly impact patients' quality of life. [7] Patients may not be entirely satisfied with the results of surgery because some lesions may regrow. It is important to set realistic expectations prior to embarking on a course of therapy.
-
The café au lait macules of neurofibromatosis have an even tan color and a smooth border. The presence of neurofibromas in the upper right corner of the photo as well as the lower left corner make a diagnosis of neurofibromatosis almost certain.
-
Neurofibromas increase in number and size over time. Soft pedunculated neurofibromas are shown here on the arm of a woman with neurofibromatosis type 1.
-
Neurofibromas are soft on palpation, and they may exhibit a buttonhole sign, whereby they can be pushed deeper into the dermis.
-
Neurofibromas are often pedunculated and are composed of spindled cells with wavy nuclei embedded in an acidophilic stroma. (Hematoxylin and Eosin stained sections; original magnification 20x).
-
Neurofibromas are composed of delicate spindle cells in a loose stroma. (Hematoxylin and Eosin; original magnification 400x)
-
Schwannomas (neurilemmomas) are benign tumors that develop along the course of nerves. Spindle cells may cluster in "stacks" that create palisades. Two adjacenet stacks with intervening Schwann cell cytoplasm are know as Verocay bodies. (Hematoxylin and eosin stained sections; original magnification 200x).
-
Schwannomas have areas with spindle shaped schwan cells (Antoni A areas) and intervening stroma (Antoni B areas). (Hematoxylin and eosin stain; original magnification 400x)
-
Sheets of spindled cells are depicted in this malignant schwannoma. Malignant degeneration should be expected in a painful or rapidly enlarging tumor in any patient with neurofibromatosis.
-
High-power view of a malignant schwannoma reveals sheets of hyperchromatic spindle cells with pleomorphic nuclei.
-
Granular cell tumors are also known as granular cell schwannomas. They often involve the mouth but may occur anywhere on the skin or in the soft tissues. Tumor cells are polygonal and have unique eosinophilic granules in the cytoplasm. (hematoxylin and eosin stained sections; original magnification 400x).
-
A light-brown hyperpigmented lesion is noted on the arm and has a smooth border. Most persons affected by neurofibromatosis type 1 have such café-au-lait macules.
-
Neurofibromas are noted on the right arm and right chest in association with a café-au-lait macule on the arm. The association of these lesions is a useful clue to the diagnosis of neurofibromatosis type 1.
-
Axillary freckling is also known as the Crowe sign. This pigmentary change is seen in about one third of individuals affected with neurofibromatosis type 1, but it can also be seen in several other conditions.








