Overview
Kawasaki disease is a dynamic vasculitic disorder that presents with various mucocutaneous findings, which are most pronounced at different times. (See the chart below.) The most characteristic features of Kawasaki disease are usually present at the time of presentation, or appear shortly thereafter. [1, 2, 3, 4, 5, 6, 7, 8]
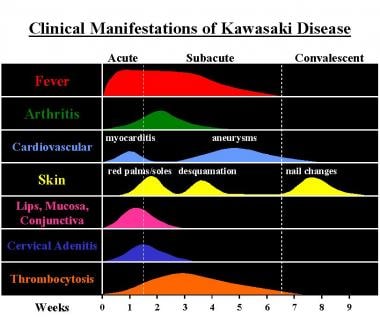 Clinical manifestations and time course of Kawasaki disease. Courtesy of Paul R. Ogershok, MD.
Clinical manifestations and time course of Kawasaki disease. Courtesy of Paul R. Ogershok, MD.
The five major clinical findings in Kawasaki disease are as follows [4, 7, 9] :
-
Change in the extremities, typically painful erythema and edema
-
Polymorphous exanthem
-
Changes in the lips and oropharyngeal mucosa
-
Bilateral, nonexudative, bulbar conjunctival injection
-
Unilateral, nonsuppurative cervical lymphadenopathy
See Kawasaki Disease: Do You Know the Signs?, a Critical Images slideshow, to help identify the specific criteria for diagnosis.
Treatment summary
The goal of treatment is to reduce inflammation in walls of the coronary arteries in order to decrease the risk of coronary thrombosis and other cardiac complications. Although the standard of care of Kawasaki disease is intervenous immunoglobulin (IVIG) [10] and high-dose aspirin, approximately 15-20% of children are nonresponders (having persistent or recurrent fever after therapy); these patients have higher risk for coronary artery damage and require additional therapy. [11] In Japan, the Egami score (based on age, duration of illness, platelet count, and C-reactive protein) is a sensitive and specific tool used at diagnosis to determine IVIG treatment resistance. [12] Several large randomized trials have been performed, which have shown reduced coronary abnormalities when intravenous methylprednisolone-pulse (IVMP) was added to traditional IVIG in patients with severe or refractory Kawasaki disease. [6, 13, 14, 15, 16]
However, it is important to keep in mind that Kawasaki disease is not a homogeneous disease, even in Japan, and the Egami score has not been well studied for non-Japanese populations. So at this juncture, IVMP plus IVIG therapy appears safe and effective for Kawasaki disease patients who are deemed to have refractory Kawasaki disease based on Egami score, at least in the Japanese population.
Other treatments that have been used for IVIG-resistant patients include additional does of IVIG; Ulinastatin (human trypsin inhibitor), which is primarily used in Japan; plasma exchange; immunosuppressants; and, recently, tumor necrosis factor-α inhibitor (infliximab). [13]
Go to Kawasaki Disease and Ophthalmologic Manifestations of Kawasaki Disease for complete information on these topics.
Dermatologic Presentation
More than 90% of patients present with a polymorphic exanthema within 3-5 days of the onset of fever. Initially, the patient may present with nonspecific erythema of the palms, soles, and perineal regions, which gradually and diffusely involves the trunk and extremities. The eruption is usually pruritic and can be macular, papular, morbilliform (as in the first image below), scarlatiniform, urticarial, erythrodermatous, targetoid (erythema multiforme‒like, [7, 8] or composed of fine micropustules and rarely vesicles. [4, 7] Purpura, petechiae, or gangrene can occasionally occur as a result of cutaneous vasculitis. [17]
Within a few days after the onset of the eruption, a fine desquamation of the perineal region occurs. (See the second image below.)
 Morbilliform eruption in Kawasaki disease. Courtesy of Noah S. Scheinfeld, MD, JD.
Morbilliform eruption in Kawasaki disease. Courtesy of Noah S. Scheinfeld, MD, JD.
 Desquamation in a patient with mucocutaneous lymph node syndrome (Kawasaki disease). Courtesy of Chemene Y. Quinn, MD.
Desquamation in a patient with mucocutaneous lymph node syndrome (Kawasaki disease). Courtesy of Chemene Y. Quinn, MD.
The extremities show distinctive changes in 94% of patients. After the initial acral erythema, the palms and soles gradually become indurated and painful, which may limit mobility. Then, during the subacute phase of the illness, approximately 14 days after the onset of fever, desquamation occurs in a glovelike fashion, first involving the periungual region of the fingers and followed a week later by a similar desquamation of the toes. (See the image below.)
 Acral desquamation during the subacute phase of the illness. Courtesy of Noah S. Scheinfeld, MD, JD.
Acral desquamation during the subacute phase of the illness. Courtesy of Noah S. Scheinfeld, MD, JD.
A 2012 study showed a positive correlation between decreased capillary blood cell velocity in the nail fold area with increased coronary artery diameter. These results suggest that dynamic capillaroscopy using laser Doppler flowmetry can show early abnormalities in the microcirculation and can serve as a noninvasive indirect tool to evaluate coronary artery status. [18]
Other Manifestations
More than 95% of Kawasaki disease patients present with protracted fever, which has a remittent pattern of several temperature spikes each day. The patient is ill and often extremely irritable.
Mucous membrane and oropharyngeal alterations begin within the first few days after the onset of fever. Changes in the lips are seen in 75-90% of patients and include erythema, dryness, cracking, and bleeding. From 50-77% of patients have an extremely erythematous tongue, with protuberance of the fungiform papillae, which has been referred to as strawberry tongue. This feature, while clinically impressive, is indistinguishable from that seen in patients with scarlet fever, a streptococcal infection. (See the image below.)
 Oral manifestations of Kawasaki disease: red lips and strawberry tongue. Courtesy of Paul R. Ogershok, MD.
Oral manifestations of Kawasaki disease: red lips and strawberry tongue. Courtesy of Paul R. Ogershok, MD.
Bilateral, nonexudative, bulbar conjunctival injection with relative sparing around the limbus occurs within a few days after the onset of fever and lasts 1-3 weeks in approximately 88% of patients. (See the image below.) Mild iridocyclitis or anterior uveitis may be seen during a slit-lamp examination but is rarely associated with eye pain or photophobia.
 Bulbar conjunctiva congestion in a patient with mucocutaneous lymph node syndrome (Kawasaki disease). Courtesy of Chemene Y. Quinn, MD.
Bulbar conjunctiva congestion in a patient with mucocutaneous lymph node syndrome (Kawasaki disease). Courtesy of Chemene Y. Quinn, MD.
Go to Ophthalmologic Manifestations of Kawasaki Disease for complete information on this topic.
The least common of the five major diagnostic criteria for Kawasaki disease is a unilateral, nontender, nonsuppurative, anterior cervical lymphadenopathy. This typically involves a single node larger than 1.5 cm in diameter. This finding is only seen in 70% of cases in Japan and in 50-86% of cases in the United States. Although uncommon, Kawasaki disease patients who present with only fever and cervical lymphadenopathy at admission typically have a greater risk of developing coronary artery abnormalities and are at risk of being nonresponders to intravenous immunoglobulin treatment. [19]
The last feature seen during the acute febrile stage is cardiovascular alterations. Cardiac auscultation may reveal various findings, such as a hyperdynamic precordium, tachycardia, a gallop rhythm, or an innocent flow murmur. These findings are nonspecific and may be initially attributed to mild anemia and/or fever.
-
Clinical manifestations and time course of Kawasaki disease. Courtesy of Paul R. Ogershok, MD.
-
Morbilliform eruption in Kawasaki disease. Courtesy of Noah S. Scheinfeld, MD, JD.
-
Desquamation in a patient with mucocutaneous lymph node syndrome (Kawasaki disease). Courtesy of Chemene Y. Quinn, MD.
-
Acral desquamation during the subacute phase of the illness. Courtesy of Noah S. Scheinfeld, MD, JD.
-
Oral manifestations of Kawasaki disease: red lips and strawberry tongue. Courtesy of Paul R. Ogershok, MD.
-
Bulbar conjunctiva congestion in a patient with mucocutaneous lymph node syndrome (Kawasaki disease). Courtesy of Chemene Y. Quinn, MD.







