Background
Pediculosis (ie, louse infestation) dates back to prehistory. The oldest known fossils of louse eggs (ie, nits) are approximately 10,000 years old. [1] Lice have been so ubiquitous that related terms and phrases such as "lousy," "nit-picking," and "going over things with a fine-tooth comb" are part of everyday vocabulary.
Louse infestation remains a major problem throughout the world, making the diagnosis and treatment of louse infestation a common task in general medical practice. [2] All socioeconomic groups can be affected. Pediculosis capitis results in significant psychological stress in children and adults and missed schooldays in children, particularly in areas with a no-nit policy. [3]
Lice are ectoparasites that live on the body. Lice feed on human blood after piercing the skin and injecting saliva, which may cause pruritus due to an allergic reaction. [4] Lice crawl; they do not have wings and cannot fly or hop. [4]
A mature female head louse lays 3-6 eggs, also called nits, per day. Nits are white and less than 1 mm long. Nymphs (immature lice) hatch from the nits after 8-9 days, reach maturity in 9-12 days, and live as adults for about 30 days. [4]
Different species of lice prefer to feed on certain locations on the body of the host. Louse species include Pediculus capitis (head lice), Pediculus corporis (body lice), and Pthirus pubis (pubic lice, sometimes called “crabs”).
See the louse images below.
 The head louse, Pediculus humanus capitis, has an elongated body and narrow anterior mouthparts. Body lice look similar but lay their eggs (nits) on clothing fibers instead of hair fibers.
The head louse, Pediculus humanus capitis, has an elongated body and narrow anterior mouthparts. Body lice look similar but lay their eggs (nits) on clothing fibers instead of hair fibers.

See When Bugs Feast: What's Causing that Itch?, a Critical Images slideshow, to help identify various skin reactions, recognize potential comorbidities, and select treatment options.
Lice move from person to person through close physical contact. Spread through contact with fomites (eg, combs, brushes, clothes, hats, scarves, coats, linens) used by an infested person is uncommon. [4] Overcrowding encourages the spread of lice. The body louse can be the vector of Rickettsia prowazeki, which causes typhus; Bartonella quintana, which causes trench fever; and Borrelia recurrentis, which causes relapsing fever.
Human lice have been used as a forensic tool. A mixed DNA profile of 2 hosts can be detectable in blood meals of body lice that have had close contact between an assailant and a victim. [5]
Pathophysiology
Louse infestation is prevalent throughout the animal kingdom. Mallophaga, or chewing lice, are common pests of birds and domestic animals, but humans only rarely are affected as accidental hosts. [6]
Human lice (P humanus and P pubis) are found in all countries and climates. They belong to the phylum Arthropoda, the class Insecta, the order Phthiraptera, and the suborder Anoplura (known as the sucking lice). [6] Mammals are the hosts for all Anoplura.
The Anoplura are wingless and have 3 pairs of legs, each with a single tarsal segment ending with a claw for grasping. The size and shape of the claws are adapted to the texture and shape of the hairs and/or clothing fibers they grasp. Their bodies are flat and covered with tough chitin.
Lice are blood-sucking insects. Human lice have small anterior mouthparts with 6 hooklets that aid their attachment to human skin during feeding. The sucking mouthparts retract into the head when the lice are not feeding. In general, lice feed approximately 5 times per day. In each species, the female louse is slightly larger than her male counterpart.
The 3 types of human lice include the head louse (Pediculus humanus capitis), the body louse (Pediculus humanus corporis), and the crab louse (Pthirus pubis). Body lice infest clothing, laying their eggs on fibers in the fabric seams. Head and pubic lice infest hair, laying their eggs at the base of hair fibers. [7, 8]
Head and body lice are similarly shaped, but the head louse is smaller. Nevertheless, the 2 species can interbreed. The pubic louse, or "crab," is morphologically distinct from the other 2.
Pediculus humanus capitis
The head louse (see the image below) is the most common of the 3 species. The average length of the head louse is 1-2 mm. Female head lice are generally larger than males. [4] The louse is wingless and white to gray and has a long, dorsoventrally flattened, segmented abdomen. It has 3 pairs of clawed legs. Its average life span is 30 days. [4]
The head louse, Pediculus humanus capitis, has an elongated body and narrow anterior mouthparts. Body lice look similar but lay their eggs (nits) on clothing fibers instead of hair fibers.
The adult female louse lays eggs, called nits, and glues them at the base of the hair shaft. Nits are placed within 1-2 mm of the scalp, where the temperature is optimal for incubation. The female head louse lays as many as 10 eggs per 24 hours, usually at night. Egg and glue extrusion onto the hair shaft takes 16 seconds. Nits typically are located at the posterior hairline and postauricular areas. [4]
Nits hatch in about 8-9 days if they are kept near body temperature and mature in another 9-12 days. [4] Nits can survive for up to 10 days away from the human host. Cooler temperatures retard both hatching and maturation. The nymph molts 3 times before reaching its adult form. The adult head louse survives only 1-2 days away from its host.
Head louse infestation is spread by close physical contact and occasionally by shared fomites (eg, combs, brushes, hats, scarves, bedding). [4] Lice can be dislodged by combs, towels, and air movement (including hair dryers in either low or high setting). [9] Hair combing and sweater removal may eject adult lice more than 1 meter from infested scalps. Head lice can travel up to 23 cm/min. [6] The head louse has difficulty attaching firmly to smooth surfaces (eg, glass, metal, plastic, synthetic leathers). [4]
Pediculus humanus corporis
The body louse is larger than the head louse. Body lice range in size from 2-4 mm. Female lice are larger than male lice. Like the head louse, the body louse is flat and white to gray with a segmented abdomen.
Unlike the head louse and the pubic louse, the body louse does not live on the human body. P humanus corporis prefers cooler temperatures; it lives in human clothing, crawling onto the body only to feed, predominantly at night. Females lay 10-15 eggs per day on the fibers of clothing, mainly close to the seams. Adult body lice can live up to 30 days but die within 1-2 days when away from the host and without blood meals. [10] On average, no more than 10 adult female lice can be found on a person with an infestation, although a thousand have been removed from the clothes on a single infested individual. [11]
Body lice are spread through contact with clothing, bedding, or towels that have been in contact with an infested individual, or through direct physical contact with a person who is infested with body lice.
Pthirus pubis
The pubic louse gets the nickname of "crab" from its short, broad body (0.8-1.2 mm) and large front claws, which give it a crab-like appearance. The pubic louse is white to gray and oval and has a smaller abdomen than both P humanus capitis and P humanus corporis. Pubic lice live for approximately 2 weeks, during which time the females lay 1-2 eggs per day. [6] Nymphs emerge from the eggs after 1 week and then mature into adults over the subsequent 2 weeks. [6]
Their large claws enable pubic lice to grasp the coarser pubic hairs in the groin, perianal, and axillary areas. Heavy infestation with P pubis can also involve the eyelashes, eyebrows, facial hair, axillary hair, and, occasionally, the periphery of the scalp.
Pubic lice are less mobile than P humanus and P corporis, mainly resting while attached to human hairs. They can crawl up to 10 cm/day. [6] They cannot survive off the human host for more than 1 day.
Nits
The average nit (ie, ovum) of the 3 types of lice is 0.8 mm long. The nit (see the images below) attaches to the base of the hair shaft (in the case of head or pubic lice) or to fibers of clothing (in the case of body lice) with a strong, highly insoluble cement; thus, nits are difficult to remove. The nit is topped with a tough but porous cap known as the operculum. This porous operculum allows for gas exchange while the nymph develops in the casing.
 Nit on a hair. Note the thin, translucent cement surrounding the hair shaft. Photo courtesy of David Shum, MD Western University, London Ontario.
Nit on a hair. Note the thin, translucent cement surrounding the hair shaft. Photo courtesy of David Shum, MD Western University, London Ontario.
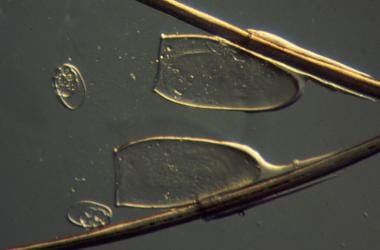 Two empty nits from Pediculus humanus capitis. Note the open shells still attached to the hairs and the porous operculi through which the lice have hatched. Photo courtesy of David G. Schaus.
Two empty nits from Pediculus humanus capitis. Note the open shells still attached to the hairs and the porous operculi through which the lice have hatched. Photo courtesy of David G. Schaus.
The ova require optimum conditions of 30°C and 70% humidity to hatch within the average time frame of 8-10 days; the incubation period is longer at lower temperatures. Ova do not hatch at temperatures lower than 22°C but can remain alive for as long as 1 month away from the body (ie, on fomites, clothing, brushes).
Etiology
Causative organisms include P humanus capitis (head louse), P humanus corporis (body louse), and P pubis (pubic louse)
P humanus capitis
Pediculosis capitis is spread by direct contact with an infested person. Head-to-head contact with an infested individual at school, at home, and while playing may result in head lice infestation; personal hygiene and environmental cleanliness are not risk factors. [4] Fomites, such as clothing, headgear, hats, combs, hairbrushes, hair barrettes, may occasionally play a role in the spread of head lice. [4] Factors that predispose to head louse infestation include young age; close, crowded living conditions; female sex; white or Asian race; and perhaps warm weather. [12] The risk for nosocomial transmission is low, unless close patient-to-patient contact (eg, playrooms, institutions) is present.
P humanus corporis
Risk factors for body lice infestation include close, crowded living situations (eg, crowded buses and trains, prison camps) [11] and infrequent washing and/or changing of clothing. P corporis can be acquired via bedding, towels, or clothing recently used by an individual infested with lice; thus, individuals who are homeless, who are impoverished, or who are living in refugee camps are at high risk for infestation. [10]
P pubis
Intimate or sexual contact with an individual who is infested with pubic lice is a common risk factor for pubic lice infestation. Risk factors for infestation of the pubic louse include sexual promiscuity and crowded living conditions. Contact with clothing, bedding, and towels used by an infested individual may occasionally be the cause of infestation. [13] It is a myth that pubic lice are spread by sitting on a toilet seat; pubic lice’s feet are not designed to walk on smooth surfaces such a toilet seats, and the lice cannot live for long away from a warm human body. [13]
Because these organisms most often are spread through close or intimate contact, P pubis infestation is classified as an STD. Condom use does not prevent transmission of P pubis. Upon diagnosis of pubic lice, concern should be raised about the possibility of concomitant STDs.
In children, infestation of pubic lice usually is contracted from a parent who is infested. Sexual transmission to children is rare. In most cases of infestations in children, transmission results from shared bed linens and close nonsexual contact.
Epidemiology
Since pediculosis is not a reportable disease, exact numbers concerning incidence are unknown. Pediculosis may be underreported because of the social stigma attached—namely, the preconceived notion that lice of any kind are related to dirt and poor personal hygiene. In fact, personal cleanliness is not a factor in head lice infestation rates. On the other hand, false-positive nit diagnosis is common. [4]
United States statistics
Pediculosis is very common; a report from 2000 estimates that 6-12 million Americans aged 3-11 years are infested each year. [14] No reliable data provide the exact number of annual cases among adults. Head louse infestation is more common in the warmer months, whereas pubic louse infestation is more common in the cooler months. [12]
Head louse infestation is most common in urban areas and may occur in all socioeconomic groups. Head louse infestations occur most commonly in school-aged children, typically in late summer and autumn. The reported prevalence ranges from 10-40% in US schools. One study estimates that 12-24 million days of school are lost because of "no-nit" school policies. [15]
Body louse infestation in the United States mainly affects homeless persons. Pubic lice generally are spread as an STD. Pubic louse infestation serves as a marker for other STDs, which may have been acquired simultaneously. [6]
COVID-19 Pandemic
COVID-19 was declared a global pandemic by the World Health Organization (WHO) in March 2020. [16] Many governments established social distancing and strict lockdowns that prevented contact between people from different households.
A study conducted in Buenos Aires, Argentina in 2020 surveyed households with school-age children (total of 1118 children) participating in strict lockdown. The study found that the prevalence of head louse infestations decreased from 69.6% pre-social distancing, to 43.9% during the COVID-19 lockdown. [17]
A study in France assessed the impact of COVID-19 lockdowns and social distancing on head lice infestations by analyzing topical head lice treatments pre-COVID-19 vs during COVID-19 lockdowns. Comparing topical head lice treatments COVID-19 lockdown periods in 2020 to pre-COVID-19 period there was a mean reduction in observed vs expected sales of 44%. [18]
Another study conducted in Israel compared pediculicide sale rates from the decade of 2010-2019 preceding the COVID-19 pandemic to 2020 during mandatory quarantines. This study reported a significant drop in pediculicide sale rates in Israel in 2020 while there were mandatory lockdowns in schools. [19]
Although the COVID-19 pandemic is ongoing and further research is needed to examine lice infestation rates during the COVID-19 pandemic, these early studies suggest that the COVID-19 pandemic has had significant effects on lice infestation rates.
International statistics
Pediculosis has a worldwide distribution and is endemic in both developing and developed countries. The prevalence of pediculosis capitis is usually higher in girls and women and varies from 0.7-59% in Turkey, 0.48-22.4% in Europe, 37.4% in England, 13% in Australia, up to 58.9% in Africa, and 3.6-61.4% in the Americas. [3]
In a study of 6,169 Belgian school children aged 2.5-12 years, the prevalence of head lice was 8.9%. [20] The prevalence in 1,569 school children in Izmir, Turkey, was 16.6%. [21] In 2005, the incidence of pediculosis doubled in the Czech Republic. [22] Live lice were detected in 14.1% and dead nits in another 9.8% of 531 children aged 6-15 years in 16 schools. [22]
A systematic review and meta-analysis including 40 studies and 200,306 individuals found the prevalence of head lice for boys, girls, and all the students in Iran, respectively, to be 1.6%, 8.8%, and 7.4%. [23]
P capitis was found in 9.6% of adolescent schoolboys in Saudi Arabia. [24] In Mali, the prevalence of head lice in children was 4.7%. [25] Among attendees of an STD clinic in south Australia, pubic lice were found in 1.7% of men and 1.1% of women. [26]
P corporis is now uncommon in developed countries except among homeless persons. [27]
Racial differences in incidence
Louse infestation affects all races and ethnic groups. All hair types can be infested by head lice. Current medical literature does not strongly indicate that race or ethnicity affect the rate of infestation. [28]
Sex- and age-related differences in incidence
Girls are at higher risk for head louse infestation than boys because of social behavior (eg, social acceptance of close physical head-to-head contact and, less commonly, sharing of hats, scarves, combs, brushes, hair ties and lying on a sofa, carpet, or stuffed toy that has recently come in contact with an infested person); hair length is not a factor. No sexual predilection exists in body or pubic louse infestation; males and females are equally likely to become infested.
Children aged 3-11 years are most likely to become infested with head lice because of close contact in classrooms and day care facilities. Head lice are much less common after puberty. Body lice are more common in adults, but can affect all ages. [29] Age is not a significant risk factor in body louse infestation; body lice are indiscriminate in regard to the age of their host. P pubis infestation is more common in people aged 14-40 years who are sexually active.
Prognosis
Prognosis is excellent when the infestation is properly managed with correct treatment.
Morbidity:
-
Frequent use of pediculicides may cause persistent itching.
-
Body lice can be vectors for diseases such as epidemic (louse-borne) typhus, trench fever, and louse-borne relapsing/recurrent fever.
-
Violation of the integrity of the skin from a bite can lead to bacterial infection with organisms such as methicillin-resistant Staphylococcus aureus (MRSA)
-
More commonly, infestation with lice produces social embarrassment and isolation rather than medical disease.
Patient Education
The social stigma associated with head lice infestation must be addressed. Poor hygiene is not a risk factor in acquiring pediculosis capitis, although it is for body lice.
Management of head lice must include examination of all individuals exposed (all household members and other close contacts) and treatment of all those who are infested. Individuals who have no evidence of infestation should not be treated unless they share a bed with an infested individual in which case they should be treated even if no lice are found. [28]
Education has been shown to reduce the number of lice infestations in schools. "No nit" policies exclude many children from the classroom, but they have not been shown to reduce the number of louse infestations. [30] Schools with “no-nit” policies should be educated to abandon these policies. The Centers for Disease Control and Prevention (CDC), American Association of Pediatrics, and National Association of School Nurses recommend discontinuation of these policies. [4]
Noncompliance is a common cause of treatment failure in all 3 types of lice infestations. Therefore, time is well-spent providing patients with detailed instructions regarding the application and timing of medications used in the treatment of lice. Fomites may harbor live lice and therefore should be treated to prevent re-infestation and infestation of other individuals.
To minimize acquiring head lice, during epidemics of head lice, children should be educated not to share combs, brushes, headbands, hats, and scarves. [6] Hats and scarves should not be piled in a common area, but rather separated for each child. [6] Shaving of hair is effective treatment of head lice, but not socially acceptable in most societies. [31]
All sexual partners from within the previous month of a person infested with pubic lice should be treated. [13] Sexual contact should be avoided until both parties have been successfully treated. Individuals infested with pubic lice are at risk for other sexually acquired diseases and should be screened for such.
In the case of body lice, infested clothing and towels need to be washed in hot water and with a hot dryer; pediculicides usually are not needed. The infested individual should be counseled on proper hygiene, changing clothing at least once a week, and proper laundering of clothing. [10]
For patient education information from the American Academy of Pediatrics. Additional information available from the CDC: head lice, body lice, pubic lice.
-
Nit on a hair. Note the thin, translucent cement surrounding the hair shaft. Photo courtesy of David Shum, MD Western University, London Ontario.
-
Two empty nits from Pediculus humanus capitis. Note the open shells still attached to the hairs and the porous operculi through which the lice have hatched. Photo courtesy of David G. Schaus.
-
Three specimens of Pediculus humanus capitis.
-
Pediculus humanus corporis.
-
Phthirus pubis. Note the crab-like appearance.
-
The head louse, Pediculus humanus capitis, has an elongated body and narrow anterior mouthparts. Body lice look similar but lay their eggs (nits) on clothing fibers instead of hair fibers.
-
The pubic louse, Pthirus pubis, is identified by its wide crablike body.








