Practice Essentials
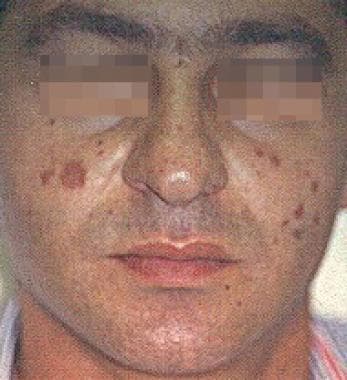
Granuloma faciale (GF) is an uncommon benign chronic skin disease of unknown origin characterized by single or multiple cutaneous nodules, usually occurring over the face. See the images below.


Occasionally, extrafacial involvement is noted, [1, 2, 3, 4] most often on sun-exposed areas. Lever and Leeper first recognized granuloma faciale as a distinct entity in 1950. Pinkus' group suggested the name granuloma faciale that same year. The disease mimics many other dermatoses and can be confused with conditions, such as sarcoidosis, discoid lupus erythematosus, mycosis fungoides, and fixed drug eruption. See Sarcoidosis, Discoid Lupus Erythematosus, Mycosis Fungoides, and Fixed Drug Eruptions for more information on these topics.
Signs and symptoms
Granuloma faciale is usually asymptomatic. It rarely may be tender or cause itching or stinging. Lesions may darken upon sun exposure.
Solitary or, more commonly, multiple, soft, elevated, and well-circumscribed papules, plaques, or nodules are observed. See the images below.


Lesions are most commonly located over the face. Reported extrafacial locations include the scalp, [5, 6] the trunk, and the upper and lower extremities.
The size of the lesions varies from a few millimeters to several centimeters in diameter.
The color varies from shades of dull red to brown, blue, and purple.
Lesions have a smooth surface with prominent follicular orifices (peau d'orange) and may be covered by telangiectases. [7]
Granuloma faciale may clinically resemble rhinophyma clinically. [8]
Diagnostics
No laboratory abnormalities are associated with granuloma faciale. Obtain an adequate skin biopsy of a representative lesion.
The histologic findings of granuloma faciale are diagnostic. The name granuloma faciale is a misnomer, as granulomas are never present histologically. The epidermis is unaffected. A grenz zone of uninvolved dermis is located beneath the epidermis. Below the grenz zone is a dense, polymorphous inflammatory infiltrate located most often in the papillary and mid dermis. The infiltrate consists of neutrophils, lymphocytes, eosinophils, monocytes, and, occasionally, mast cells. Vasculitic changes, including perivascular inflammation with nuclear dust and vessel wall damage, are often observed. This chronic localized fibrosing leukocytoclastic vasculitis is a vasculitic reaction pattern seen in granuloma faciale and erythema elevatum diutinum. [9] Extravasated RBCs and hemosiderin deposition are found, which may contribute to the color of the lesions. Later, lesions may show considerable fibrosis around venules. See the images below.
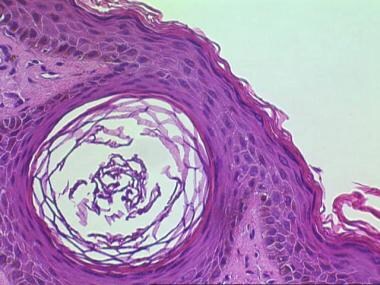
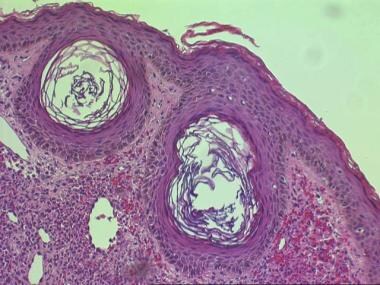
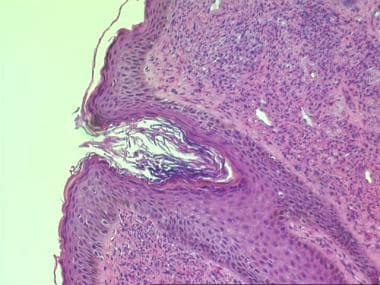 Histologic findings in granuloma faciale include a normal epidermis; a grenz zone of uninvolved dermis just beneath the epidermis; and a dense, polymorphous inflammatory infiltrate located in the papillary and mid dermis. The infiltrate consists of neutrophils, lymphocytes, eosinophils, monocytes, and, occasionally, mast cells. Perivascular inflammation is also observed.
Histologic findings in granuloma faciale include a normal epidermis; a grenz zone of uninvolved dermis just beneath the epidermis; and a dense, polymorphous inflammatory infiltrate located in the papillary and mid dermis. The infiltrate consists of neutrophils, lymphocytes, eosinophils, monocytes, and, occasionally, mast cells. Perivascular inflammation is also observed.
Immunophenotyping in one study documented a higher intensity of T lymphocytes than B lymphocytes, with a predominance of T CD8 lymphocytes in almost two thirds of cases, whereas other studies have tended to show the major component as T CD4 lymphocytes. [10] IgG4 was demonstrated in most, but in less than 25% of stained cells.
Direct immunofluorescence reveals immunoglobulin G (IgG), fibrin, and, occasionally, immunoglobulin M deposition at the basement membrane zone and perivascularly. Granuloma faciale in one study did not demonstrate the immunohistochemical diagnostic criteria for IgG4-related disease. [11]
Electron microscopy reveals more perivascular eosinophils than suggested by light microscopy. Charcot-Leyden crystals, the eosinophil granules, are evident within eosinophils as well as histiocytes, providing evidence of degranulation.
Management
Granuloma faciale is notoriously resistant to treatment; therefore, many different medical options available, with topical steroids and tacrolimus favored choices, sometimes enhanced with topical dapsone. [12, 13] Pulsed-dye laser [4, 14, 15] often produces resolution without scarring and should generally be tried before the patient is started on long-term medication. Other therapeutic options that have been tried and are reported to be effective include topical corticosteroid therapy, intralesional corticosteroid injections (without or in combination with 5-fluorouracil, [16] , intralesional gold injections, oral bismuth, antimalarials, isoniazid, oral potassium arsenite, p-aminobenzoic acid (PABA), calciferol, topical psoralen UV-A (PUVA), [17] intralesional rituximab, [18, 19] and radiation therapy. More recently, topical tacrolimus has been reported of benefit. [20, 21, 22] Granuloma faciale can also be treated with another topical calcineurin inhibitor, pimecrolimus cream. [23] Dapsone is the oral medication most frequently reported to be of some benefit. [24, 25, 26, 27] Rituximab is a monoclonal antibody against CD-20 approved by the US Food and Drug Administration for treatment of some autoimmune and tumoral diseases.
A variety of surgical procedures may be used in the management of granuloma faciale. Scarring may occur with many of these, so the pulsed dye laser is preferred if it is available. Note the following:
-
Surgical excision
-
Dermabrasion [28]
-
Argon laser [29]
-
Carbon dioxide laser [30]
-
Electrosurgery
-
The 585-nm pulsed dye laser [34]
Scarring may result from ablative treatment modalities. Close postsurgery follow-up care is required as well as regular monitoring of patients on medications, such as dapsone.
Pathophysiology
The skin is the primary organ system that is affected. Reports of granuloma faciale–like lesions of the oral mucosa are rare. [35] Eosinophilic angiocentric fibrosis may be viewed as its mucosal counterpart. [36] Innate and adaptive immunity seem to be factors in the pathogenesis of granuloma faciale. [37]
Etiology
Some cases are idiopathic.
Production of interleukin 5 by the clonal T-cell population may cause the attraction of eosinophils to the lesions. [38]
A gamma interferon–mediated process has been suggested. [39]
Sun exposure may play a role. Sunlight-exposed areas are more commonly affected than non–sun-exposed areas. Lesions may darken with sunlight exposure.
Epidemiology
Cases of granuloma faciale are rare. Granuloma faciale is found most commonly in Whites; however, it has been reported rarely in Japanese and Black people. Men are affected more frequently than women. Granuloma faciale is primarily a disease of middle age (median age, 45 y).
Prognosis
No systemic involvement has been reported with granuloma faciale. The disease is benign except for its appearance. Granuloma faciale may persist indefinitely if untreated; spontaneous resolution rarely occurs. Granuloma faciale has a tendency to relapse after treatment.
Patient Education
Inform the patient about scarring and the recurrence of the condition if an ablative procedure is performed. Inform the patient about the adverse effects of medications and the need for follow-up care while taking these medications for this recalcitrant disorder.
-
Solitary, well-demarcated, brown-red plaque associated with granuloma faciale.
-
Solitary, well-demarcated, brown-red plaque associated with granuloma faciale.
-
Solitary, well-demarcated, brown-red plaque associated with granuloma faciale.
-
Granuloma faciale.
-
Histologic findings in granuloma faciale.
-
Histologic findings in granuloma faciale.
-
Histologic findings in granuloma faciale.
-
Histologic findings in granuloma faciale.
-
Histologic findings in granuloma faciale.
-
Histologic findings in granuloma faciale include a normal epidermis; a grenz zone of uninvolved dermis just beneath the epidermis; and a dense, polymorphous inflammatory infiltrate located in the papillary and mid dermis. The infiltrate consists of neutrophils, lymphocytes, eosinophils, monocytes, and, occasionally, mast cells. Perivascular inflammation is also observed.
-
Histologic findings in granuloma faciale.
-
Multiple brown-red plaques on the face associated with granuloma faciale.
-
Multiple brown-red plaques on the nose associated with granuloma faciale.
-
Multiple brown-red plaques on the forehead associated with granuloma faciale.
-
Close-up view of multiple brown-red plaques on the forehead associated with granuloma faciale.
-
Close-up view of multiple brown-red plaques on the nose associated with granuloma faciale.






