Practice Essentials
Nodular localized cutaneous amyloidosis (NLCA) is a rare condition characterized by the deposition of amyloid or amyloid-like proteins in the dermis. The cause of NLCA is not known, although the amyloid protein is derived from a localized infiltrate of plasma cells. Skin biopsy provides the definitive diagnosis; special stains and immunohistochemistry are helpful (see the image below). Laser therapy, excision, and curettage and electrodessication have been used to treat NCLA lesions. [1]
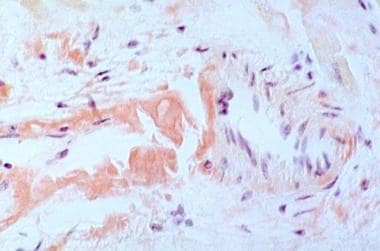 The bright pink homogeneous-appearing material seen is amyloid stained with Congo red. A distinguishing feature of amyloid in the skin is an affinity to take up Congo red stain.
The bright pink homogeneous-appearing material seen is amyloid stained with Congo red. A distinguishing feature of amyloid in the skin is an affinity to take up Congo red stain.
Signs and symptoms
NLCA lesions usually are asymptomatic. The firm, pink to brown or red nodules vary from a few millimeters to a few centimeters and may coalesce to form larger plaques. The nodules can present at any cutaneous site including the face, scalp, extremities, trunk, and genitalia; however, acral areas are preferentially involved.
See Presentation for more detail.
Diagnosis
Laboratory studies
Normal serum protein electrophoresis and urine protein electrophoresis studies help to exclude multiple myeloma. Positive antinuclear, anti-Ro, and anti-La antibody tests suggest Sjögren syndrome. Urinalysis or 24-hour urine testing can be performed to check for protein.
Imaging and other studies
The following imaging studies may be included in the workup:
-
Chest radiography
-
Electrocardiography
-
Abdominal ultrasonography
-
Scintigraphy with radioiodinated serum amyloid P component (SAP scanning)
The definitive diagnostic test is skin biopsy. Bone marrow biopsy with gene rearrangement studies may be considered to exclude multiple myeloma.
See Workup for more detail.
Management
Methods that have been used to treat NLCA lesions include the following:
-
Topical and intralesional corticosteroids
-
Intralesional methotrexate
-
Cryotherapy
-
Dermabrasion
-
Shaving
-
Curettage and electrodesiccation
-
Carbon dioxide laser
-
Pulsed dye laser
See Treatment for more detail.
Background
Localized cutaneous amyloidosis (LCA) refers to a condition characterized by the deposition of amyloid or amyloid-like proteins in the dermis. Localized cutaneous amyloidosis encompasses several conditions characterized by amyloid deposition, including macular amyloidosis, lichen amyloidosis, and biphasic amyloidosis (both forms are present). Nodular localized cutaneous amyloidosis (NLCA) is the rarest type of localized cutaneous amyloidosis and is distinct from the other forms. By definition, nodular localized cutaneous amyloidosis describes a primary disease of the skin, although lesions occasionally appear similar to the skin manifestations of systemic amyloidosis.
Pathophysiology
As a term, "amyloid" was used historically to define proteins that shared similar microscopic characteristics and affinity for certain stains. Research has revealed that "amyloid" proteins are heterogeneous. The various diseases characterized by deposition of "amyloid" proteins are similarly heterogeneous but have in common the deposits of fibrillar proteins characterized as "amyloid" in the dermis. In nodular localized cutaneous amyloidosis, the amyloid is believed to derive from local plasma cells, in contrast to lichenoid or macular amyloidosis, which have keratinocyte-derived amyloid.
In nodular localized cutaneous amyloidosis, plasma cells produce immunoglobulin γ light chains as well as β2-microglobulin, which are precursors to the amyloid fibril protein(s) termed amyloid L. Reports differ regarding the clonality of this population of plasma cells. In some instances, plasma cells have been monoclonal, suggesting that nodular localized cutaneous amyloidosis is a neoplastic disorder. [2] On the other hand, cutaneous plasma cell clonality has been observed in the absence of a monoclonal plasma cell population in the bone marrow. [2, 3] In other cases, plasma cells demonstrated polyclonality, which usually is a feature of a more reactive process.
Epidemiology
United States data
The incidence and prevalence of localized cutaneous amyloidosis in the United States are not known; however, the scarcity of reported patients with localized cutaneous amyloidosis indicates that the condition may be rare.
International data
Despite a paucity of reported patients, localized cutaneous amyloidosis, although rare, is represented in the American, Asian, and European literature.
Morbidity/mortality
Nodular localized cutaneous amyloidosis typically is benign and limited to the skin. However, lesions are more often persistent. Reported rates of progression to systemic disease are derived from case series with small numbers of patients; these rates vary from 7% to nearly 50%. [4, 5] Progression to fatal systemic amyloidosis has been reported, although this is a rare occurrence. [6] As many as 25% of reported cases have been associated with Sjögren syndrome. Some speculate that these 2 disorders may have a shared pathogenesis. [7, 8, 9, 10, 11]
Case reports have also correlated nodular localized cutaneous amyloidosis with other autoimmune disorders such as CREST syndrome (calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia syndrome), primary biliary cirrhosis, rheumatoid arthritis, and systemic lupus erythematosus. [12] Other rare associations described in the case report literature include alcoholic cirrhosis [13] and severe atopic dermatitis. [14]
Race-, sex-, and age-related demographics
Epidemiologic data can be difficult to establish when so few patients are reported. No specific racial, ethnic, or geographic group appears more prone than another to developing nodular localized cutaneous amyloidosis.
Of the first 13 patients described in the Japanese literature, 12 were women; however, this disproportionate ratio has not been seen consistently. In a subsequent series of 12 patients, the male-to-female ratio was equal. Other series have reported equal or nearly equal male-to-female ratios.
Patients reportedly range in age from 33-86 years. The mean age of onset has been reported to be 55 years. Although numbers are small, reports indicate that nodular localized cutaneous amyloidosis is likely to occur during adulthood.
-
The bright pink homogeneous-appearing material seen is amyloid stained with Congo red. A distinguishing feature of amyloid in the skin is an affinity to take up Congo red stain.
-
Amyloid shows apple green when examined with polarized light.
-
This transmission electron micrograph of amyloid deposited in the tissue shows loosely interwoven straight filaments.






