Practice Essentials
Gardner syndrome, a variant of familial adenomatous polyposis (FAP), [1] is an autosomal dominant disease characterized by GI polyps, multiple osteomas, and skin and soft tissue tumors. Cutaneous findings [2] of Gardner syndrome include epidermoid cysts, desmoid tumors, and other benign tumors. Polyps have a 100% risk of undergoing malignant transformation (see the figure below); consequently, early identification of Gardner syndrome is critical. [3, 4]
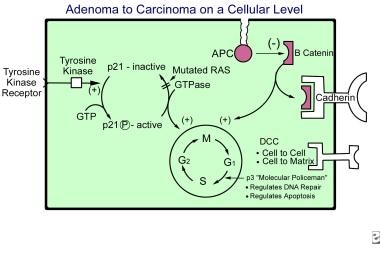 Adenoma-to-carcinoma sequence on a cellular level.
Adenoma-to-carcinoma sequence on a cellular level.
Signs and symptoms
Many skin findings of Gardner syndrome are evident on full body examination; however, the patient's history of the age at onset and whether lesions are present in family members is important.
Cysts in Gardner syndrome patients are usually asymptomatic, but they may be pruritic and/or inflamed.
More than half the patients with Gardner syndrome have dental anomalies. [5] Previously undiagnosed Gardner syndrome may be detected when the patient is evaluated for multiple impacted and unerupted teeth. Dentists may play a pivotal role in detecting craniomaxillofacial osteomas, a major criterion for Gardner syndrome. [6]
See Presentation for a full discussion.
Diagnostics
Thyroid screening by physical examination and ultrasonography is recommended in Gardner syndrome. Chromosome studies from peripheral blood lymphocytes and allele-specific expression assay can be performed. Screen all first-degree relatives of patients with Gardner syndrome or FAP.
Most parents believed it was their responsibility to inform young family members about genetic testing results, an often emotionally challenging matter encouraging preventive screening and possible lifestyle adaptions. [7]
Imaging studies
Imaging studies are essential for screening patients and family members who are affected. Panoramic radiography of the mandible can demonstrate subtle opacities at an early age. Long bone radiographs may demonstrate osteomas or hyperostosis. Ultrasonography is performed to screen for thyroid tumors. Van Epps et al reported seeing epidermal inclusion cysts on a CT scan from a patient with Gardner syndrome. [8]
Procedures
Perform an ophthalmologic examination at an early age to detect pigmented lesions of the fundus.
Fecal occult blood, sigmoidoscopy/colonoscopy, and upper GI endoscopy are required at least every 1-2 years until the patient reaches age 50 years.
Histologic findings
Pathologic findings of the epidermoid cysts of Gardner syndrome are similar to findings in non–Gardner syndrome cysts; however, many have pilomatricomalike changes. [9] In 1 study, 63% of cysts examined from 7 patients with Gardner syndrome demonstrated 1 or more matricoma features, such as columns of shadow cells, calcification, and basophilic matrixlike cells in the cyst lining.
The Gardner fibroma, a soft tissue tumor of children and young adults, displays a bland hypocellular proliferation of haphazardly arranged coarse collagen fibers with a bland hypocellular proliferation of inconspicuous spindle cells, small blood vessels, and a sparse mast cell infiltrate. Immunohistochemically, many show nuclear reactivity for beta-catenin and most, if not all, have nuclear reactivity for both cyclin-D1 and C-myc. These fibromas may serve as an indicator for familial Gardner syndrome or similar disorder. [10, 11]
Treatment of the cutaneous manifestations of Gardner syndrome depends on the symptomatic or cosmetic nature and the location of the cysts. Treatment is similar to that used for ordinary cysts and involves excision [12] or use of intralesional steroids if the cysts are inflamed. Conservative management with chemotherapy or tyrosine kinase inhibitors is now being favored. [13]
Antiestrogens and anthracycline-containing regimens may have a favorable radiological response rate against desmoid tumors and may be a viable option in some patients. [14]
Surgical care
Colectomy [15] is recommended for Gardner syndrome patients if 30 or more polyps are detected on colonoscopy or if biopsy results reveal dysplasia or malignant degeneration. Preserving the rectum results in a 25-59% chance of rectal carcinoma occurring in Gardner syndrome patients; therefore, rectal mucosal resection is recommended. Total gastroduodenectomy with pancreatic preservation may be desirable in some settings. [16]
Generally, cutaneous findings do not require treatment. Osteomas may require excision if they are severely deforming or if they interfere with function.
Also see the General Surgery article Gardner Syndrome.
Pathophysiology
Gardner syndrome is genetically linked to band 5q21, the adenomatous polyposis coli locus. [17] FAP and Gardner syndrome are believed to be variants of the same condition. The wider spectrum of abnormalities found in Gardner syndrome may represent variable penetrance of a common genetic mutation. Novel pathogenic alterations have been described. [18] A novel large germline fragment deletion of the adenomatous polyposis coli (APC) gene was identified in a Chinese family with this syndrome. [19] The osteomas represent genetically-driven neoplasms, with mutations in the APC gene resulting in aberrant Wnt/β-catenin signaling. [20]
Etiology
The cause of Gardner syndrome is genetic, with autosomal dominant inheritance.
Epidemiology
Frequency
In the United States, 1 person per million population is diagnosed with Gardner syndrome. The incidence of FAP is 1 case per 8000 people. The most common cutaneous finding in patients with Gardner syndrome is epidermoid cysts (50-65%).
Age
Although colonic polyps begin to form in puberty, the average age at Gardner syndrome diagnosis is 22 years. Osteoma formation precedes polyposis. Usually, progression to malignancy is observed in patients aged 30-50 years. The average age by which malignancy is diagnosed is 39.2 years.
Prognosis
With adequate screening, long-term control of colorectal tumors is possible, with desmoid tumors determining the survival and quality of life for many patients. [21] Unless surgical transection is performed, GI polyps may progress to malignancy in almost 100% of Gardner syndrome patients (rates vary from 58-100% in studies). A genetic variant with an aggressive early childhood phenotype has been described. [22]
-
Adenoma-to-carcinoma sequence on a cellular level.




