Practice Essentials
McCune-Albright syndrome (MAS) consists of at least two of the following three features: (1) polyostotic fibrous dysplasia (PFD), (2) café-au-lait skin pigmentation (see the image below), and (3) autonomous endocrine hyperfunction (eg, gonadotropin-independent precocious puberty). Other endocrine syndromes may be present, including hyperthyroidism, acromegaly, and Cushing syndrome. Mazabraud syndrome, which can also exist in association with MAS, involves the occurrence of myxomas and usually PFD. [1, 2, 3, 4, 5, 6]
 McCune-Albright syndrome case showing café-au-lait pigmentation. Lesion does not cross midline, which is typical of pigmented lesions in this syndrome.
McCune-Albright syndrome case showing café-au-lait pigmentation. Lesion does not cross midline, which is typical of pigmented lesions in this syndrome.
Signs and symptoms of McCune-Albright syndrome
The clinical presentation of MAS is highly variable, depending on which of the various potential components of the syndrome predominate. Major manifestations include the following:
-
Precocious puberty (typically gonadotropin-independent) - This includes breast development, genital maturation (with or without pubic hair growth), increased height velocity, and macroorchidism [7]
-
Café-au-lait pigmentation - This consists of spots ranging from light brown to dark brown in color, often displaying a segmental distribution, and frequently predominating on one side of the body without crossing the midline; these spots must be differentiated from those characteristic of neurofibromatosis (NF)
-
PFD - Multiple pathologic fractures may be prominent early in the history; in many cases, bony involvement is found to predominate clinically on 1 side; potential presenting features include gait anomalies, visible bony deformities (including abnormal bone growths of the skull), bone pain, and joint stiffness with pain
-
Hyperthyroidism (rare without several other features of MAS also being present) - Findings may include tachycardia, arrhythmias (mostly supraventricular), hypertension, hyperthermia, tremor, sleeplessness, weight loss, or (in infants) failure to thrive
Other possible manifestations include the following:
-
Cushing syndrome
-
Growth hormone (GH) excess (gigantism and acromegaly)
-
Acromegaly
-
Ovarian cysts
-
Pituitary tumors
-
Thyroid tumors
-
Hypophosphatemia (hypophosphatemic rickets)
-
Hypogonadotropic hypogonadism, particularly in the setting of hyperprolactinemia
See Clinical Presentation for more detail.
Diagnosis of McCune-Albright syndrome
A complete medical history and physical examination are important in the evaluation of MAS, especially with an eye toward finding apparent endocrine hyperfunction and skeletal deformities.
Full endocrine studies should be performed. Testicular or ovarian hyperfunction is the most common abnormality. Laboratory studies that may be helpful include the following:
-
Gonadotropin (luteinizing hormone [LH], follicle-stimulating hormone [FSH]) and sex hormone levels
-
Blood and urinary chemistries
-
Thyroid testing (thyroid-stimulating hormone [TSH], thyroxine [T4], antithyroid antibodies)
-
Adrenocorticotropic hormone (ACTH) levels
-
Serum prolactin (PRL)
-
Dexamethasone suppression testing (standard or low-dose/high-dose)
-
Urine collection assayed for free cortisol (urinary free cortisol [UFC])
-
Growth hormone (GH) and insulinlike growth factor 1 (IGF-1) levels
-
Polymerase chain reaction (PCR) assay
Diagnostic imaging modalities that may be considered include the following:
-
Plain radiography (mainly skull and mandibles [craniofacial survey], pelvis, femurs; as clinically indicated)
-
Ultrasonography (neck and thyroid; ovarian and pelvic; as clinically indicated)
-
Computed tomography (CT); as clinically pertinent
-
Magnetic resonance imaging (MRI); as clinically pertinent
-
Radionuclide bone scanning
Other studies that may be considered include the following:
-
Arterial blood gas determination (for suspected acidosis)
-
Electrocardiography (ECG; (for suspected arrhythmia)
-
Gastrointestinal (GI) endoscopy can be performed to evaluate (for suspected polyposis)
-
Biopsy (bone, muscle, soft tissue, thyroid); as clinically pertinent
See Workup for more detail.
Management of McCune-Albright syndrome
There is no specific treatment for MAS per se. Pharmacologic agents that have been used to treat precocious puberty in MAS include the following:
-
Aromatase inhibitors
-
Gonadotropin-releasing hormone (GnRH) analogues (as adjuncts to aromatase inhibitors)
-
Ketoconazole [8]
-
Estrogen receptor agonists (eg, tamoxifen)
-
Spironolactone
-
Cyproterone acetate
-
Medroxyprogesterone acetate
Currently, no clinically proven medical therapies are available for PFD associated with MAS. Oral and intravenous (IV) bisphosphonates (eg, pamidronate, alendronate, zoledronate) may be beneficial to prevent disease progression, although data are conflicting. Important: bisphosphonates are very effective at relieving pain in the majority of cases.
Pharmacologic agents that have been used to treat hyperthyroidism in MAS include the following:
-
Thionamides (eg, propylthiouracil)
-
Methimazole
-
Radioiodine (for tissue ablation)
No long-term effective medical treatment for ACTH-independent Cushing syndrome is available.
Pharmacologic agents that have been used to treat GH excess in MAS include the following:
-
Octreotide
-
Dopamine agonists (eg, bromocriptine and cabergoline), typically in conjunction with octreotide
-
GH receptor antagonists (eg, pegvisomant), probably best not used as monotherapy in this setting
Pharmacologic treatment of other manifestations of MAS is as follows:
-
Hypogonadism - Appropriate hormone replacement therapy
-
Hypophosphatemia with hyperphosphaturia - Aggressive oral phosphorus replacement
-
Hypophosphatemic rickets - Appropriate calcitriol therapy with calcium and phosphate repletion
Surgical interventions that may be considered include the following:
-
Precocious puberty – Oophorectomy or ovarian cystectomy, when medical therapy fails
-
PFD – Traction or fixation for fractures; for most PFD lesions, routine removal is not warranted
-
Hyperthyroidism – Thyroidectomy (partial near-total, or total)
-
Infantile Cushing syndrome – Bilateral adrenalectomy
-
Gigantism or acromegaly – Surgical removal of the offending lesion (pituitary adenoma) is rarely curative and is considered only if the tumor is threatening vision (in consultation with an experienced base-of-skull neurosurgeon)
See Treatment and Medication for more detail.
Background
McCune-Albright syndrome (MAS) in its classic form consists of at least 2 of the following triad of features [9, 10, 11] :
-
Polyostotic fibrous dysplasia (PFD)
-
Café-au-lait skin pigmentation
-
Autonomous endocrine hyperfunction – The most common form of autonomous endocrine hyperfunction in this syndrome is precocious puberty, which is typically gonadotropin-independent [12, 13]
Other endocrine syndromes described in association with MAS include the following [14, 15] :
-
Acromegaly or gigantism (due to GH-producing pituitary adenoma)
-
Gonadotropinomas
-
Hyperprolactinemia
Some severely affected patients may present with associated hepatic, cardiac, and gastrointestinal (GI) dysfunction (ie, elevated hepatic transaminases, GI polyposis, and cardiomyopathy). [16]
MAS has been shown to be due to a postzygotic activating mutation of the GNAS gene, coding for the G protein subunit Gs alpha in the affected tissues (see Pathophysiology and Etiology). For semantic reasons, it is important to differentiate MAS from Albright hereditary osteodystrophy (AHO). AHO, which also is caused by a GNAS1 gene defect, [17] results in pseudohypoparathyroidism or pseudopseudohypoparathyroidism. [18]
The clinical presentation of MAS is highly variable, depending on which of the various potential components of the syndrome predominate (see Presentation). Diagnosis of MAS depends on finding at least 2 of the phenotypic features associated with activating GNAS1 mutations.
Early recognition is vital. In typical cases, the diagnosis of MAS is not in doubt. However, in atypical cases, the combination of cutaneous pigmentation, bony lesions, and soft-tissue masses may suggest other conditions (eg, systemic mastocytosis and neurofibromatosis [NF]) (see DDx).
Full endocrine studies should be performed under the care of an endocrinologist. Testicular or ovarian hyperfunction is the most common abnormality. Diagnostic imaging modalities that may be considered include plain radiography, ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and radionuclide bone scanning (as clinically indicated) (see Workup).
Because MAS is a multisystemic condition with a host of variable presentations, management often is challenging and requires a multidisciplinary approach. For most physicians who are not endocrinologists, the crucial points in management are recognition of MAS and referral of the patient to an endocrinologist who is experienced in its management. The endocrinologist, in turn, offers other referrals as indicated (eg, neurosurgeon) (see Treatment).
Pathophysiology
Most of the clinical features of McCune-Albright syndrome (MAS) are caused by a noninherited postzygotic activating mutation of the GNAS1 gene that results in overproduction of a variety of protein products in a fashion independent from normal feedback control mechanisms (see Etiology). [10]
Precocious puberty, the most common endocrine feature of MAS, is a result of gonadotropin-independent autonomous ovarian or testicular function. [7] Precocious puberty caused by this condition is far more common in girls than in boys. In girls, it is the result of estrogen excess from ovarian follicular cysts. [19] Because the sexual precocity associated with MAS is gonadotropin-independent, it is more accurately described as pseudoprecocious puberty.
The café-au-lait spots in MAS are large melanotic macules, sometimes referred to as café-au-lait macules (CALMs). Except for hyperpigmentation of the basal layer, no abnormal pathology is seen.
Fewer than 10 cases of MAS associated with Cushing syndrome have been well documented. This syndrome is distinct, unlike all other endocrinopathies of MAS, which are slowly progressive and persistent without treatment. Several cases of Cushing syndrome in the context of MAS have regressed within the first few years following onset.
Cushing syndrome associated with MAS is predominantly due to adrenocortical hyperfunction. Most of these cases have been described in infants or children. The adrenal glands are bilaterally enlarged and contain multiple small nodules in the cortex. In some cases, Cushing syndrome is transitory. Pituitary-based (ACTH-dependent) Cushing disease in the setting of MAS is far less common.
Hyperthyroidism typically occurs later in childhood, though it can occur within the first year of life. Like Cushing syndrome and precocious puberty, hyperthyroidism associated with MAS is a result of 1 or more autonomous hyperfunctioning thyroid nodules.
Growth hormone (GH) excess from somatotroph adenomas in the pituitary can occur at any age, resulting in gigantism or acromegaly. The GH excess among patients with MAS has been noted to be as high as 21%. The basis of GH hypersecretion in MAS remains incompletely understood, but it appears to have a different basis from that of acromegaly or gigantism in non-MAS patients. [20] A study by Yao et al suggested that growth hormone excess in MAS occurs more frequently in males than in females; the investigators determined that of 52 patients with MAS, 13 (25.0%) had growth hormone excess, including 10 males (76.9%). The study also found an association between growth hormone excess in MAS and greater severity of skeletal lesions, with more craniofacial bone involvement. [21]
Fibrous dysplasia (FD) in MAS can involve any bone but most commonly affects the long bones, ribs, and skull. It may range from small asymptomatic areas detectable only by bone scan to markedly disfiguring lesions that can result in frequent pathologic fractures and impingement on vital nerves.
Approximately 30 cases of FD associated with single or multiple intramuscular or juxtamuscular myxomas (Mazabraud syndrome) have been documented. [2, 3] This syndrome has been associated with precocious puberty and café-au-lait spots and occurs in association with MAS. The myxomas associated with this condition can occur in virtually any location in the muscular system. The exact etiopathogenesis of the syndrome is unclear, because no activating mutations of the GNAS1 gene have been demonstrated in this clinical variant.
Simple myxomas typically are benign and solitary, with peak incidence in the sixth and seventh decades. The age of peak incidence for this syndrome is young adulthood, and the tumors commonly are multiple. The main sites of involvement are the large muscles of the thighs, buttocks, and shoulders. They often are located close to FD lesions but typically remain separate from them. They commonly recur, even after attempts at surgical resection.
Hypophosphatemic rickets is a potential complication that may worsen the bone disease associated with PFD. It is due to a tubulopathy and characterized by hyperphosphaturia. In patients with MAS, hyperphosphaturia may be due to a phosphatonin similar to that seen in patients with tumor-induced osteomalacia, which appears to be fibroblast growth factor 23 (FGF-23). While MAS patients with hypophosphatemic rickets are typically managed with calcitriol and phosphorus supplements, they must be monitored closely for hypercalcemia, excessive hypercalciuria, nephrocalcinosis, and progressive loss of renal function, as well as the development of secondary hyperparathyroidism.
Hepatic abnormalities range from mild elevation of hepatic transaminases to severe neonatal jaundice and chronic cholestasis. Although some liver biopsies appear normal, others reveal mild biliary abnormalities or fatty liver. One case report described fatty liver in an infant with Cushing syndrome, suggesting that the fatty liver may have been secondary to glucocorticoid excess. Elevated transaminases in this infant, however, persisted long after the glucocorticoid excess had been corrected with adrenalectomy.
A study by Wood et al indicated that a wide range of gastrointestinal (GI) tract and pancreatic abnormalities occur in patients with MAS, with the investigators pointing out that GNAS mutations are not only responsible for MAS but are also found in association with several GI and pancreatic neoplasms. GI abnormalities in the study’s seven patients included gastric heterotopia/metaplasia, gastric hyperplastic polyps, fundic gland polyps, and a hamartomatous polyp, with endoscopic ultrasonographic findings in the pancreas suggesting the presence of intraductal papillary mucinous neoplasms (IPMNs). [22]
In a cross-sectional study of 54 patients with MAS, Robinson et al found radiographic GI abnormalities in 30 (56%) of them. IPMNs occurred in 25 (46%) patients, with 14 individuals having IPMNs alone and 11 also having abnormal hepatobiliary imaging. In addition, the investigators reported that, compared with the rest of the cohort, more fibrous dysplasia (as evaluated using skeletal burden scores), as well as a greater prevalence of acute pancreatitis and diabetes mellitus, was present in the patients with MAS-associated GI pathology. [23]
Many case reports describe sudden deaths, mostly occurring in patients with multiple endocrine and nonendocrine manifestations of MAS. Persistent tachycardia has been observed in addition to mild-to-moderate cardiomegaly, even in the absence of hyperthyroidism. Although the cause of death in these patients is unclear, it is presumed to be secondary to cardiac arrhythmia.
Only a few cases of malignant transformation of skeletal lesions have been described in the setting of MAS, most frequently in the setting of therapeutic irradiation. This occurs in probably less than 1% of MAS cases. The tendency for malignant transformation to occur may be greater in patients who have concomitant GH excess or those with Mazabraud syndrome. Observed malignancies include the following:
-
Osteosarcomas (most common)
A study by Hagelstein-Rotman et al, using the Dutch Pathology Registry and the Netherlands Cancer Registry, as well as the investigators’ patient cohort, suggested that the risk for osteosarcoma, melanoma, and cervical, thyroid, and prostate cancer is greater in individuals with FD/MAS. The standardized morbidity ratios for these patients were as follows [24] :
-
Osteosarcoma (19.7)
-
Cervical cancer (4.93)
-
Thyroid cancer (3.71)
-
Prostate cancer (3.08)
-
Melanoma (2.01)
Females appear to be at greater risk for breast cancer, probably as a consequence of prolonged exposure to elevated estrogen and/or GH levels. The underlying GNAS1 mutation also may play a role. For the same reasons, these patients also appear to be at increased risk for thyroid malignancies and testicular cancer (a novel finding by the National Institutes of Health [NIH]).
Etiology
McCune-Albright syndrome (MAS) is caused by a sporadic, early postzygotic somatic mutation in the GNAS1 gene at locus 20q13.1-13.2, coding for the G protein subunit Gs alpha. [25] This genetic finding has been noted and confirmed in various tissue specimens from patients with MAS. [26] Researchers have isolated activating mutations of GNAS1 in pituitary adenomas, thyroid adenomas, ovarian cysts, monostotic bone dysplasia, and the adrenal glands. [27] GNAS1 gene abnormality in pseudohypoparathyroidism I-a has also been noted. [28]
G proteins couple cell surface receptors to intracellular proteins to activate or inactivate signaling cascades. The stimulatory G protein is normally activated when a hormone or other ligand binds to the cell surface receptor (see the image below). The activated Gs alpha disassociates from the receptor, binds to adenylyl cyclase, and stimulates an increase in intracellular cyclic adenosine monophosphate (cAMP) levels. Gs alpha then is inactivated, reassociates with the receptor, and is again available for hormone-mediated reactivation.
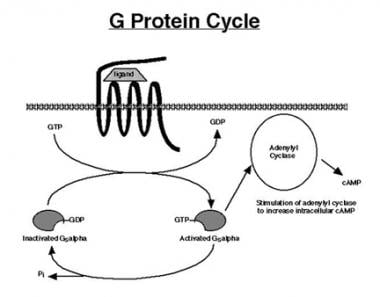 The G protein cycle begins with ligand binding to a 7-transmembrane domain G protein-coupled receptor (GPCR). Binding of the cognate ligand forms a ligand-receptor complex, which then stimulates an exchange of guanosine triphosphate (GTP) for guanosine diphosphate (GDP) on the alpha subunit of the stimulatory G protein (Gs alpha). This activates the alpha subunit, which subsequently stimulates adenylyl cyclase (AC) to increase production of cyclic adenosine monophosphate (cAMP). The alpha subunit contains intrinsic guanosine triphosphatase (GTPase) activity, which cleaves a phosphate group from GTP, converting it to GDP, and thus inactivates the alpha subunit. The inactivated alpha subunit is now ready to be reactivated by ligand-receptor binding, so that the next cycle of signal transduction can occur.
The G protein cycle begins with ligand binding to a 7-transmembrane domain G protein-coupled receptor (GPCR). Binding of the cognate ligand forms a ligand-receptor complex, which then stimulates an exchange of guanosine triphosphate (GTP) for guanosine diphosphate (GDP) on the alpha subunit of the stimulatory G protein (Gs alpha). This activates the alpha subunit, which subsequently stimulates adenylyl cyclase (AC) to increase production of cyclic adenosine monophosphate (cAMP). The alpha subunit contains intrinsic guanosine triphosphatase (GTPase) activity, which cleaves a phosphate group from GTP, converting it to GDP, and thus inactivates the alpha subunit. The inactivated alpha subunit is now ready to be reactivated by ligand-receptor binding, so that the next cycle of signal transduction can occur.
The mutations that cause MAS occur at a site in the protein that mediates inactivation of Gs alpha (see the image below). Once activated, the mutated Gs alpha subunit remains activated for a prolonged period despite the absence of hormone (GPCR ligand) stimulation. This results in constitutive activation of Gs alpha, constant stimulation of adenylyl cyclase, and persistently high levels of intracellular cAMP. Increased cAMP levels can mediate mitogenesis and increased cell function. The specific phenotype depends on the cell type containing the mutation.
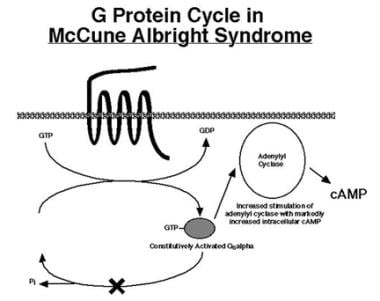 Mutations in McCune-Albright syndrome inactivate intrinsic guanosine triphosphatase (GTPase) activity, thus preventing inactivation of the "turned-on" Gs alpha subunit. Once activated, the mutated Gs alpha subunit is able to continuously stimulate adenylyl cyclase, even in absence of ligand binding to its cognate GPCR receptor. The result is elevation of intracellular cyclic adenosine monophosphate (cAMP) and continual stimulation of downstream cAMP signaling cascades.
Mutations in McCune-Albright syndrome inactivate intrinsic guanosine triphosphatase (GTPase) activity, thus preventing inactivation of the "turned-on" Gs alpha subunit. Once activated, the mutated Gs alpha subunit is able to continuously stimulate adenylyl cyclase, even in absence of ligand binding to its cognate GPCR receptor. The result is elevation of intracellular cyclic adenosine monophosphate (cAMP) and continual stimulation of downstream cAMP signaling cascades.
The classic triad of features in MAS-PFD, autonomous endocrine hyperfunction, and café-au-lait skin pigmentation—can all be explained by activation of the Gs alpha subunit and increased intracellular cAMP levels.
Eumelanogenesis (formation of brown/black pigment) is normally stimulated by melanocyte-stimulating hormone (MSH) binding to the MSH receptor, a classic G protein receptor coupled to Gs alpha. Constitutive activation of the Gs alpha subunit in melanocytes results in the increase in brown pigmentation characteristic of the café-au-lait spots seen in the syndrome. Likewise, both the luteinizing hormone (LH) and the follicle-stimulating hormone (FSH) receptors are Gs alpha−coupled receptors.
Constitutive activation of the postreceptor cAMP signaling cascade in ovarian follicular cells results in cyst formation, estrogen production, and gonadotropin-independent precocious puberty. Similar mechanisms of increased intracellular cAMP likely explain essentially all of the other endocrine and nonendocrine features of MAS.
Because MAS results from a postzygotic somatic mutation, all the daughter cells of the embryonic cell in which the initial mutation occurred also contain the mutation. The earlier the mutation occurs in embryogenesis, the more widespread the tissue involvement.
Mutations late in embryogenesis are more focused and account for those mild cases in which only 2 or 3 of the classic phenotypic features of the syndrome are present. If the mutation occurs very late in tissue development after differentiation into a specific cell line, then a single adenoma may result. Gs alpha−activating mutations have been reported in isolated hyperfunctioning thyroid nodules and in somatotroph adenomas.
Although GNAS1 mutations could occur in germ cells (either oocytes or spermatocytes), the resulting zygote and all daughter cells then would contain the mutation. Activating GNAS1 mutations are likely lethal if they occur very early in embryogenesis. This accounts for the lack of autosomal dominant transmission of this syndrome.
Epidemiology
United States and international statistics
The exact incidence of McCune-Albright syndrome (MAS) in the United States and internationally is unknown, but its prevalence is probably between 1 case in 100,000 population and 1 case in 1 million population, rendering it a very rare, sporadically occurring disorder. [10] In a review of radiographs from 82,000 patients, only 23 cases of PFD were found. Polyostotic variants of FD are uncommon, and MAS is even less common. The relative incidence of monostotic FD (MFD) is 70%, whereas that of PFD is 30% and that of MAS is less than 3%.
Age-, sex-, and race-related demographics
Severe cases of MAS involving multiple endocrine tissues may be recognized shortly after birth. Cases of infantile Cushing syndrome and hyperthyroidism have also been reported in the neonatal period. Additionally, FD, café-au-lait pigmentation, liver disease, and hypophosphatemia can initially be seen in infancy.
Less severe findings of MAS can occur at almost any time during childhood. Most commonly, the onset of MAS occurs in early childhood (mean age, 4.9 years; range, 0.3-9 years), typically earlier in girls than in boys. Precocious puberty in girls can be seen in infants as young as 4 months, though it more frequently occurs in girls older than 1 year. Café-au-lait pigmentation is more likely to become apparent later in the progression of the syndrome.
GH-producing pituitary tumors and functional-thyroid adenomas secondary to activating GNAS1 mutations can occur in individuals at any age. Disease with a later onset (ie, in the early to late teenage years) tends to be associated with clinically attenuated phenotypes.
Both sexes are affected by MAS, but the syndrome has been reported to be about twice as common in females as in males. That girls develop precocious puberty far more frequently than boys (9:1 female-to-male ratio) probably explains why this autosomal mutation is recognized more frequently in girls than in boys. Other manifestations of MAS probably occur with approximately equal frequency in females and males.
MAS has no ethnic predilection.
Prognosis
Apart from the small subgroup of patients with increased perioperative mortality and those patients who develop malignancies, McCune-Albright syndrome (MAS) is not associated with a significantly increased mortality. In general, patients achieve a normal life span. Mortality and morbidity related to MAS result from the fractures, malignancies, endocrine disorders, and other conditions associated with this syndrome. The symptom and disability burden of MAS can be quite high, owing to the associated chronic pain and deformities, as well as the sequelae of chronic multihormonal endocrinopathies. Thus, the prognosis varies according to the manifestations of MAS.
With precocious puberty, the prognosis depends on the duration of premature estrogen exposure. Early puberty is not a life-threatening condition and does not seem to lead to problems after true, centrally mediated puberty begins at an appropriate age. Early breast development and vaginal bleeding can be accompanied by loss of adult height potential. Reduction of height potential depends on the degree of bone age advancement that occurs during the periods of early estrogen exposure.
A study of 16 girls and 10 boys with MAS found (1) that MAS occurs slightly more frequently in girls than in boys, (2) that peripheral precocious puberty (PPP) in MAS occurs significantly more frequently and at a younger age in girls than in boys, (3) that PPP in boys with MAS correlates with bilateral testicular enlargement, (4) that unilateral macroorchidism can occur, and (5) that testicular microlithiasis might function as another marker for MAS in males. [29]
Moreover, a literature review by Aversa et al indicated that at presentation, macroorchidism is the most common testicular abnormality related to MAS. In addition, the study found that in MAS, an association does not always exist between macroorchidism and clinical and biochemical evidence of peripheral precocious puberty. [30]
FD may have severe effects, including pathologic fractures, facial disfigurement, and vision and hearing problems. It is difficult to treat effectively. Current therapies focus on treating complications of FD, rather than on preventing it from developing. Current studies using bisphosphonates are promising, though it is unclear whether bisphosphonates significantly reduce the morbidity associated with these lesions.
Hyperthyroidism can cause severe failure to thrive in infants and young children, decreased attention span, and osteoporosis. Tachycardia resulting from severe hyperthyroidism may complicate or trigger a cardiac event. Radioiodine (131 I) ablation or thyroidectomy treats hyperthyroidism effectively. The long-term prognosis is excellent with adequate thyroid hormone replacement.
Infantile Cushing syndrome can cause severe growth failure, poor muscle tone, and hypertension. Permanent effect on growth potential is also possible. Comorbid heart and liver disease are poor prognostic markers and may indicate the need for prompt adrenalectomy. [31]
The long-term prognosis for infantile Cushing syndrome depends on adequate replacement of both mineralocorticoids and glucocorticoids. Individuals remain at risk for significant morbidity or mortality due to adrenal insufficiency during times of severe stress and should receive stress doses of hydrocortisone on an emergency basis.
Hypophosphatemia causes rickets and short stature; the pathophysiology of hypophosphatemic rickets, as well as the need for long-term therapy with calcitriol and phosphorus supplementation in these cases, increases the risk of nephrocalcinosis and loss of renal function over time.
Gigantism or acromegaly can occur, carrying a risk of glucose intolerance, hypertriglyceridemia, hypertension, and mild myopathy. GH secretion in MAS is difficult to treat effectively. Octreotide acetate or pegvisomant has proved effective in many cases, but not all. Furthermore, radiation treatment of the adenoma increases the risk of malignant change in areas of FD in the radiation field. The long-term prognosis in refractory cases of acromegaly is poor.
Although 2 long-term follow-up studies have shown no increased risk of premature death, several authors have noted unexplained sudden death in patients with a severe phenotype. Patients may have multiple endocrine, cardiac, GI, central nervous system (CNS), hematopoietic, and hepatic manifestations, all of which can contribute to significant morbidity. Although no arrhythmias have been detected in individuals with MAS, this is the presumed mechanism of sudden death.
Patient Education
Educational requirements depend on the phenotypic expression of McCune-Albright syndrome (MAS). Individuals with FD in critical weight-bearing areas should be instructed to avoid activities (eg, contact sports) that put the skeleton at risk for pathologic fracture.
Patients who have undergone bilateral adrenalectomy for Cushing syndrome should be given clear instructions on changing steroid dosing for febrile illnesses. Furthermore, these individuals need to wear medic alert identification bracelets or necklaces so that if severe illness or trauma occurs, medical personnel will be aware of the requirement for stress doses of hydrocortisone.
Patients should also be informed MAS is not hereditary and that offspring of affected patients are not at increased risk for the syndrome.
For patient education resources, see the Thyroid and Metabolism Center, as well as Thyroid Problems.
-
Base of the skull computed tomography scan showing extensive fibrous dysplasia in McCune-Albright syndrome. Note the asymmetrical affectation, with near-total obliteration of various neural foramina at the base of the skull. This degree of fibrous dysplasia can result in multiple cranial nerve compression neuropathies, of which blindness and deafness (from involvement of cranial nerves II and VIII) are among the most disabling.
-
Café au lait spot. This is a fairly large, irregular-edged ("coast-of-Maine" variety) lesion. It presents as a brownish, otherwise-asymptomatic macule/patch. The degree of pigmentation is fairly uniform.
-
Fibrous dysplasia of a long bone characterized by focal bony expansion, patchy areas of sclerosis, and bony cyst formation in McCune-Albright syndrome.
-
Plain skull radiograph in a typical McCune-Albright syndrome case shows marked macrocrania, frontal bossing, and markedly thickened bony table in patchy areas, particularly at base of skull and occiput. Skull also shows hair-on-end appearance, which needs to be differentiated from similar radiologic appearances in Paget disease or poorly controlled hemoglobinopathy (eg, beta-thalassemia, sickle cell disease).
-
Large café-au-lait patches around shoulder in child with McCune-Albright syndrome.
-
Lucency characteristic of polyostotic fibrous dysplasia in patient with McCune-Albright syndrome.
-
McCune-Albright syndrome case showing café-au-lait pigmentation. Lesion does not cross midline, which is typical of pigmented lesions in this syndrome.
-
Adrenal hyperplasia with nodular elements in adrenal gland isolated from infant with infantile Cushing syndrome in the context of McCune-Albright syndrome. DNA isolated from nodular tissue was determined to have activating Gs alpha mutation (GNAS1), whereas DNA isolated from surrounding tissue did not contain this mutation.
-
The G protein cycle begins with ligand binding to a 7-transmembrane domain G protein-coupled receptor (GPCR). Binding of the cognate ligand forms a ligand-receptor complex, which then stimulates an exchange of guanosine triphosphate (GTP) for guanosine diphosphate (GDP) on the alpha subunit of the stimulatory G protein (Gs alpha). This activates the alpha subunit, which subsequently stimulates adenylyl cyclase (AC) to increase production of cyclic adenosine monophosphate (cAMP). The alpha subunit contains intrinsic guanosine triphosphatase (GTPase) activity, which cleaves a phosphate group from GTP, converting it to GDP, and thus inactivates the alpha subunit. The inactivated alpha subunit is now ready to be reactivated by ligand-receptor binding, so that the next cycle of signal transduction can occur.
-
Mutations in McCune-Albright syndrome inactivate intrinsic guanosine triphosphatase (GTPase) activity, thus preventing inactivation of the "turned-on" Gs alpha subunit. Once activated, the mutated Gs alpha subunit is able to continuously stimulate adenylyl cyclase, even in absence of ligand binding to its cognate GPCR receptor. The result is elevation of intracellular cyclic adenosine monophosphate (cAMP) and continual stimulation of downstream cAMP signaling cascades.





