Environmental Distribution
Endemic syphilis is a disease that is common to dry, hot climates and to rural areas of poor economic status, education, and personal hygiene. [1, 2] Transmission occurs when skin or mucous membranes come in contact with infected skin lesions.
Features of endemic syphilis have been noted in Africa as far back as the start of recorded history.
Endemic syphilis is also known as sibbens (Scotland), radseyege (Scandinavia), siti (Gambia), therlijevo (Croatia), njovera (Zimbabwe), frenjak (Balkans), and nonvenereal endemic syphilis (Bejel).
Endemic syphilis in the United States
Rare cases of endemic syphilis have been reported in the United States. When reported, the cases are typically seen in immigrants and people coming from endemic areas. Owing to its mode of transmission, endemic syphilis is easily transmitted to new areas. Hygiene; living conditions; and environmental factors, such as weather, have made the disease fastidiously endemic in the United States.
International distribution of endemic syphilis
Parts of Africa (eg, Sahel countries [Sudan, Zimbabwe, South Africa]), parts of the Middle East (eg, Nomadic/Bedouin tribes of Saudi Arabia, Iraq, and Syria), and parts of Asia (eg, Turkey, Southeast Asia, the Western Pacific) are affected. In these areas, seropositivity in children reaches as high as 40%, and early lesions reportedly affect 2-20% of children. [3]
Transmission
Species of the spirochete Treponema cause diverse infections in humans. T pallidum causes venereal syphilis. T carateum and T pertenue cause pinta and yaws, respectively. Endemic syphilis is caused by T pallidum subsp endemicum. [4]
Endemic syphilis is transmitted through direct or indirect skin-to-skin or mouth-to-mouth contact with the infected lesion. It occurs predominantly in children aged 2-15 years. Because children are the active transmitters of the disease, infection of all members of a household is very common.
Wearing gloves at all times is imperative for the physician who is examining lesions caused by endemic syphilis.
Congenital syphilis is rarely encountered, because the disease can be treated during pregnancy.
The common housefly, Musca domestica, has not been established as a potential vector.
Morbidity in Endemic Syphilis
Because the disease rarely manifests clinically significant cardiovascular and neurologic symptoms, mortality is uncommon unless the disease state is highly exaggerated, through either a large inoculum or a devastating immune reaction.
Race, Sex, and Age Predilections
Endemic syphilis can affect anyone. Because it is endemic in certain areas of the world, the disease mostly affects ethnic groups found in those regions.
Both sexes are equally affected, especially in the pediatric population. This varies with the geographic region. In adults, however, women are slightly more susceptible, probably because they are the primary interactants with children, either as caregivers or during breastfeeding.
Children aged 2-15 years are the most commonly affected by endemic syphilis, with 25% of cases occurring before age 6 years and 55% of cases occurring before age 16 years. The remaining 20% of cases occur in adults who are in close contact with children who are infected. [5]
The incidence of endemic syphilis has increased among HIV-infected men in same-sex relationships. A study at a hospital in Malaga, Spain, showed an increase from 1.2% in 2007 to 7.8% in 2012. [6]
Symptoms and Stages
Endemic syphilis has a pathology and histology similar to those of venereal syphilis. However, the effects on organ systems are different.
Primary stage
The incubation period for endemic syphilis is 10-90 days.
Primary lesions usually manifest in the oropharynx.
Skin lesions in the primary stage resemble the chancres of venereal syphilis. A small, eroded or ulcerated papule is usually asymptomatic. Observing a lesion on the nipple of a mother with a suckling child who is infected is not uncommon.
Primary lesions heal in 1-6 weeks and often go undiagnosed. Generalized lymphadenopathy is uncommon, since the inoculum is small.
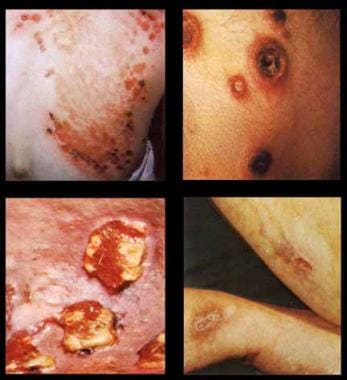
See the image below.

Yaws can present with chronic skin ulcers, especially in tropical and subtropical climates. [7, 8, 9, 10, 11, 12]
Secondary stage
This stage usually consists of macerated, eroded patches on the lips, the tongue, and the tonsils. Hypertrophic condyloma lata can appear in the anogenital area.
Nontender, generalized lymphadenopathy is common, painful osteoperiostitis in the long bones (eg, tibia) can occur, and angular stomatitis resembling that caused by vitamin B deficiency can be seen.
The secondary stage can persist for 6-9 months.
See the image below.

Tertiary and late stages
The development of tertiary and late-stage disease usually occurs 6 months to years after inoculation.
Destruction of the bone and the cartilage in the formation of gummatous lesions (commonly in the nose) may take place. The gummas can ulcerate and develop chronic serpiginous tracts. Healing results in depigmented scars with a hyperpigmented border.
Saddle nose deformity and palate perforation can occur.
Rare, atypical involvement of the cardiovascular and nervous systems can occur.
See the image below.
Mimics of Endemic Syphilis
Because of the overlap between treponematoses, endemic syphilis has to be correctly differentiated from venereal syphilis, yaws, and pinta. The differential diagnoses of the diseases are very similar, and some features, such as nasopharyngeal lesions, can be difficult to differentiate.
During the early stages, features in endemic syphilis resemble a number of dermatoses, mainly eczema, mycoses, psoriasis, leprosy, herpes simplex, perlèche, and condylomata acuminata.
In the late stages, the features overlap those of malignant tumors, including carcinoma; mycosis fungoides; lupus vulgaris; and lupus erythematosus. [13]
The mutilating nasopharyngeal lesions can be mistaken for tertiary venereal syphilis tuberculosis, leprosy, rhinoscleroma, and mucocutaneous leishmaniasis.
Diagnosis of Endemic Syphilis
The best and most reliable method to diagnose endemic syphilis is to gather a thorough clinical history and to conduct a complete physical examination. Geographic data, including travel information, is invaluable in establishing the diagnosis.
Laboratory tests confirm the clinically based diagnosis. These laboratory tests are the same as those used for the diagnosis of venereal syphilis. [14]
Serologic, morphologic, and biochemical tests are not useful in distinguishing between the types of treponemal infections.
Serologic tests
Results of treponemal tests, such as the fluorescence treponemal antibody absorption (FTA-ABS) test, are positive in all stages of the disease. [15, 16, 17]
Nontreponemal tests, such as the Venereal Disease Research Laboratory (VDRL) test and the rapid plasma reagent (RPR) test, are reactive 2-3 weeks after the onset of the primary lesion. These tests have a sensitivity of 80% in patients with a 2- to 3-month history of symptomatic primary syphilis. In the secondary stage, these tests have a sensitivity of near 100%.
Dark-field microscopy
This is the best method to confirm a treponemal disease. Although it does not specify the correct species because of similarities in morphology, the test promptly confirms that the infection is caused by a treponeme.
Serum is obtained by squeezing the base of the lesion.
Treatment of Endemic Syphilis
Endemic syphilis responds well to penicillin and other treponemicidal drugs. Patients become noninfectious within 24 hours.
After successful treatment, the titer of nontreponemal tests shows a gradual decline and eventually becomes negative.
No vaccines for endemic syphilis are available.
Patient Information
Early detection and treatment campaigns aimed at endemic syphilis by health officials are extremely important. Improvement of social and medical conditions and continuing health education help to halt the spread of the disease and facilitate its eradication.
For patient education information, see the Sexual Health Center, as well as Syphilis.
Questions & Answers
Overview
What is the US prevalence of endemic syphilis?
What is the global prevalence of endemic syphilis?
How is endemic syphilis transmitted?
What is the morbidity and mortality associated with endemic syphilis?
Which patient groups have the highest incidence of endemic syphilis?
How do the effects of endemic syphilis differ from venereal syphilis?
What are the signs and symptoms of primary-stage endemic syphilis?
What are the signs and symptoms of secondary-stage endemic syphilis?
What are the signs and symptoms of late-stage endemic syphilis?
How is endemic syphilis differentiated form venereal syphilis, yaws, and pinta?
How is endemic syphilis diagnosed?
What is the role of serologic testing in the diagnosis of endemic syphilis?
What is the role of dark-field microscopy in the diagnosis of endemic syphilis?
How is endemic syphilis treated?
How is endemic syphilis eradicated?
-
Primary stage lesions.
-
Second-stage condylomata lata lesions.
-
Third-stage gummatous lesions.








