Practice Essentials
Tarsal coalition is the abnormal union of 2 or more bones in the hindfoot and midfoot. This union may be either complete or incomplete, and the condition may be congenital or acquired secondary to trauma, infection, surgery, or articular disorders. Coalitions can be bony (synostosis), cartilaginous (synchondrosis), or fibrous (syndesmosis). [1, 2, 3, 4, 5, 6, 7, 8, 9]
The classification of tarsal coalitions is based on the bones affected. The 2 most common types are calcaneonavicular and talocalcaneal, which constitute more than 90% of cases. Although calcaneocuboid, talonavicular, and cubonavicular tarsal fusions also occur, they are less common. [10] Calcaneonavicular coalition may be visible on standard radiographs, whereas talocalcaneal coalition is best visualized by computed tomography or magnetic resonance imaging. [1, 2]
Although tarsal coalition can exist at birth, synostosis usually occurs later in the patient’s growth period. Coalition gradually becomes symptomatic as the coalition ossifies. In most cases of calcaneonavicular coalition, ossification occurs from 8 to 12 years of age, whereas patients with talocalcaneal coalition develop symptoms around 12 to 16 years of age. [11]
(See the images below.)
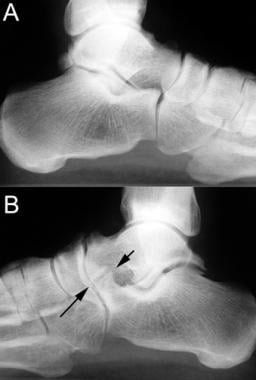
 Medial oblique radiographs of both feet in a patient with unilateral calcaneonavicular coalition. A, Unaffected side. B, Fibrous calcaneonavicular coalition (arrows). Note the decrease in the space between the calcaneus and navicular with the formation of pseudoarthrosis.
Medial oblique radiographs of both feet in a patient with unilateral calcaneonavicular coalition. A, Unaffected side. B, Fibrous calcaneonavicular coalition (arrows). Note the decrease in the space between the calcaneus and navicular with the formation of pseudoarthrosis.
 Lateral radiographs of both feet in a patient with unilateral calcaneonavicular coalition (same patient as in previous image). A, Unaffected side. B, Fibrous calcaneonavicular coalition. Note the elongated tubular extension of the anterior calcaneus seen on the lateral film (arrows) compared to the unaffected side.
Lateral radiographs of both feet in a patient with unilateral calcaneonavicular coalition (same patient as in previous image). A, Unaffected side. B, Fibrous calcaneonavicular coalition. Note the elongated tubular extension of the anterior calcaneus seen on the lateral film (arrows) compared to the unaffected side.
 Talocalcaneal coalition. Lateral radiograph of the foot reveals a classic C sign (arrows), which is a C-shaped line formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali. The C sign is a reliable indicator of subtalar coalition on lateral radiographs.
Talocalcaneal coalition. Lateral radiograph of the foot reveals a classic C sign (arrows), which is a C-shaped line formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali. The C sign is a reliable indicator of subtalar coalition on lateral radiographs.
Preferred examination
Initial evaluation of a patient suspected of having tarsal coalition begins with conventional radiography and the acquisition of 3 images: oblique, anteroposterior (AP), and lateral weight-bearing views of the feet. [12, 13, 14] Virtually all calcaneonavicular coalitions can be evaluated by using plain radiographs, although talocalcaneal coalitions generally require cross-sectional imaging, because their assessment can be difficult on conventional radiographs. Standing anteroposterior and lateral and Harris views are helpful in making the diagnosis. Radiographs of the ankle joint may demonstrate an apparent ball-and-socket ankle. On lateral views, the talar beak sign is seen at the distal dorsal aspect of the talar head near the talonavicular joint, which is caused by abnormal biomechanical stresses at the talonavicular joint. The C sign is seen on lateral radiographs, which is caused by the bony continuity of the inferomedial border of the talus and the posteroinferior aspect of the sustentaculum tali. On a true lateral radiograph, there is an absent middle facet sign. [1, 2, 15, 3, 16]
Cross-sectional imaging with CT or MRI is advantageous for evaluation of complicated cases of tarsal coalition for preoperative surgical planning. [17] Imaging with CT or MRI allows a more precise determination of articular involvement, and these examinations may be necessary for diagnosis. MRI is especially essential in the detection of nonosseous fibrous and cartilaginous coalitions. [16, 18, 19, 20, 21, 22, 23, 24, 25]
Radiography
Radiographs are important in screening for tarsal coalitions, especially with calcaneonavicular tarsal coalitions; however, findings may not be sufficient for thorough evaluation of a complex subtarsal coalition. AP, lateral, and oblique views of the feet are the standard projections obtained. [26] False-negative findings can occur with talocalcaneal coalitions because they are more difficult to detect with radiography than with other techniques. [16, 23]
Standing anteroposterior and lateral and Harris views are helpful in making the diagnosis. Radiographs of the ankle joint may demonstrate an apparent ball-and-socket ankle. On lateral views, the talar beak sign is seen at the distal dorsal aspect of the talar head near the talonavicular joint, which is caused by abnormal biomechanical stresses at the talonavicular joint. The C sign is seen on lateral radiographs, which is caused by the bony continuity of the inferomedial border of the talus and the posteroinferior aspect of the sustentaculum tali. On a true lateral radiograph, there is an absent middle facet sign. [1, 2, 3, 15]
(See the radiographic images below.)
Medial oblique radiographs of both feet in a patient with unilateral calcaneonavicular coalition. A, Unaffected side. B, Fibrous calcaneonavicular coalition (arrows). Note the decrease in the space between the calcaneus and navicular with the formation of pseudoarthrosis.
Lateral radiographs of both feet in a patient with unilateral calcaneonavicular coalition (same patient as in previous image). A, Unaffected side. B, Fibrous calcaneonavicular coalition. Note the elongated tubular extension of the anterior calcaneus seen on the lateral film (arrows) compared to the unaffected side.
Talocalcaneal coalition. Lateral radiograph of the foot reveals a classic C sign (arrows), which is a C-shaped line formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali. The C sign is a reliable indicator of subtalar coalition on lateral radiographs.
Calcaneonavicular coalition findings are as follows:
-
Calcaneonavicular coalition is viewed best on a 45° internal oblique radiograph.
-
Calcaneonavicular coalition is not depicted well on AP and lateral projections.
-
A coalition bridge extends from the anterolateral process of the calcaneus and fuses with the dorsolateral margin of the navicular bone.
-
A solid bony bar forms a bridge if an osseous coalition is present.
-
Occasionally, a fracture can appear through the coalition.
-
In patients with fibrous and cartilaginous coalitions, irregularity and narrowing of bone interfaces may occur in addition to sclerosis and eburnation.
-
A secondary radiographic sign of hypoplasia of the talar head is observed in some patients.
-
On lateral projections, the anteater nose sign may appear as a result of an anterosuperior calcaneal protrusion. [27]
Talocalcaneal coalition findings are as follows:
-
Talocalcaneal coalition often involves the middle facet at the talar-sustentaculum tali junction. The anterior and posterior facets are involved less frequently.
-
Talocalcaneal coalitions are difficult to visualize using the 3 standard radiographic projections.
-
Harris-Beath (axial) views of the hindfoot are useful for visualizing the posterior and middle facets. With the ankle slightly dorsiflexed at 10°, the beam is directed through the hindfoot at a 45° angle. The angle is adjusted if the facets are still not well demonstrated. Obliteration or irregularity of the facets is indicative of a coalition.
Numerous secondary radiographic signs are associated with talocalcaneal coalitions, such as the following:
-
The talar beak occurs because of limitations of the subtalar joint motion. This rigidity causes the navicular bone to sublux dorsally. [15]
-
At the insertion of the talonavicular ligament, a periosteal reaction occurs, and continued osseous repair leads to the formation of a beak at the dorsal aspect of the talar head.
-
Although it is less common, a similar type of formation can occur at the navicular dorsal surface.
-
A beak is not present in all patients with talocalcaneal coalition. Furthermore, these findings are not necessarily pathognomonic for a coalition. The beak may be seen in other conditions that can limit motion, such as diffuse idiopathic skeletal hyperostosis and rheumatoid arthritis.
-
Typically, the sustentaculum tali slopes upward. In patients with talocalcaneal coalition, an abnormal horizontally positioned sustentaculum tali may be present. This causes an attenuation in the x-ray beam as it crosses the sustentaculum over an increased distance. Unfortunately, false-positive C signs can occur with severe pes valgus deformity and improper positioning.
-
In addition, the C sign may be incomplete or missing. This may be seen with variations in sustentaculum tali size and orientation, radiolucent fibrous or cartilaginous talocalcaneal coalitions, and mild cases of coalition with lack of involvement at the posterior subtalar joint.
-
Concavity of the undersurface of the talar neck is seen occasionally.
-
The ball-and-socket ankle joint refers to an adaptive change caused by subtalar limitations in motion. Biomechanical stressors resulting from restrictions with inversion and eversion cause the proximal talar surface to become convex and cause a concavity to form at the distal tibial surface. The ball-and-socket joint is not pathognomonic for talocalcaneal coalition; this appearance can occur in midfoot disorders, genu valgum deformity, shortened extremities, or hypoplasia or aplasia of the fibula.
-
Flattening and rounding of the lateral talus can occasionally be seen. This finding is most apparent when compared with radiographs of the opposing unaffected foot.
-
Narrowing at the posterior talocalcaneal joint space is noted in approximately 50% of patients. This finding may be the result of calcaneal eversion or degenerative arthritic change.
Computed Tomography
With CT scans, the feet are assessed simultaneously after proper uniform positioning in the CT gantry. Proper assessment of tarsal coalitions requires both axial and coronal views of the ankle and foot. Section thickness of 3 mm or less are optimal for evaluation. Coalitions and degenerative changes are usually easier to diagnose with CT scans than with standard radiographs. This form of imaging is extremely useful for preoperative planning. [18, 19, 20, 23, 31, 16, 25]
CT data are usually unequivocal for osseous involvement. However, CT has limitations, and MRI is superior in differentiating osseous from fibrous coalitions. False-positive findings can occur with CT because of its limitations in the detection of nonosseous coalitions.
(See the CT scan images below.)
 CT scan in a patient with unilateral calcaneonavicular coalition. Note pseudoarthrosis between the calcaneus and navicular bones (arrow).
CT scan in a patient with unilateral calcaneonavicular coalition. Note pseudoarthrosis between the calcaneus and navicular bones (arrow).
 Talocalcaneal coalition. CT scan. Note the fusion of the sustentacular articulation with solid bone obliterating the joint.
Talocalcaneal coalition. CT scan. Note the fusion of the sustentacular articulation with solid bone obliterating the joint.
Calcaneonavicular coalition findings are as follows:
-
Joint-space narrowing and reactive sclerosis can be seen in calcaneonavicular coalitions.
-
On axial views, 2 abnormalities are noted: Medial broadening of the anterior and dorsal aspects of the calcaneus can occur at the navicular interface.
-
On coronal views, lateral bridging with protrusion of an abnormal bony mass and rounding of the talus may be present.
Talocalcaneal findings are as follows:
-
Coronal CT images are the most useful in the assessment of talocalcaneal coalitions. As mentioned previously, the middle facet of the talocalcaneal articulation is most frequently involved.
-
Occasionally, osseous bridging can be seen at the posterior and anterior facets; often, these findings are associated with more progressive cases.
-
Evaluating the sustentaculum tali carefully is important. The sustentaculum often extends in an upward medial direction. It may slant downward or laterally in talocalcaneal coalitions.
-
Hypoplasia of the sustentaculum is noted occasionally; however, broadening of this structure is relatively common.
As expected, findings in nonosseous coalitions usually are subtler. Articular narrowing and reactive bony changes, such as subchondral sclerosis and cystic changes, are sometimes minimal.
Magnetic Resonance Imaging
Protocols differ from institution to institution. Three views of the feet and ankle are ideal: axial, coronal, and sagittal. Bone marrow, soft-tissue edema, and inflammatory changes are best evaluated by using fat-suppressed sequences such as short-tau inversion recovery (STIR) or fat-suppressed T2-weighted sequences. Osseous structures, ligaments, and tendons are evaluated with T1-weighted, T2-weighted, and fast spin-echo proton density–weighted images. [18, 20, 23, 24, 31, 32, 16]
(See the magnetic resonance images below.)
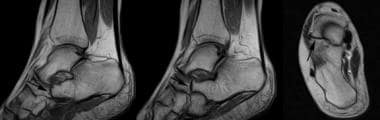 MRI in a patient with calcaneonavicular coalition. Note pseudoarthrosis between the calcaneus and navicular bones (arrows).
MRI in a patient with calcaneonavicular coalition. Note pseudoarthrosis between the calcaneus and navicular bones (arrows).
 Talocalcaneal coalition. MRI shows the fusion of the sustentacular articulation with solid bone obliterating the joint (arrow).
Talocalcaneal coalition. MRI shows the fusion of the sustentacular articulation with solid bone obliterating the joint (arrow).
Sagittal and axial images are most useful in the evaluation of calcaneonavicular coalitions. Sagittal views are particularly advantageous because of the oblique alignment of a calcaneonavicular bridge. Coronal views are valuable for assessing talocalcaneal coalitions. A continuous bone marrow bridge is visible at the junction of an osseous coalition. Marginal reactive changes can be noted.
STIR, fat-saturated T2-weighted, or proton density–weighted imaging may show edema at the articulation. In nonosseous coalitions, findings such as articular narrowing and irregularity of joint space signal intensities may be present. With fibrous and cartilaginous coalitions, a more precise interpretation is obtained with MRI than with other imaging modalities.
Nuclear Imaging
Scintigrams demonstrate abnormally increased uptake at the region of the coalition. Although CT and MRI still provide the most graphic views of the coalition site, scintigraphy may be useful as a screening procedure if plain radiographic results are equivocal. In addition, scintigraphy can provide important localizing information in complicated cases. [33]
In the workup of a limping patient, SPECT/CT can be helpful in the assessment of fusions (bony, cartilaginous, or fibrous coalition) and the grade of scintigraphic activity. [34]
-
Medial oblique radiographs of both feet in a patient with unilateral calcaneonavicular coalition. A, Unaffected side. B, Fibrous calcaneonavicular coalition (arrows). Note the decrease in the space between the calcaneus and navicular with the formation of pseudoarthrosis.
-
Lateral radiographs of both feet in a patient with unilateral calcaneonavicular coalition (same patient as in previous image). A, Unaffected side. B, Fibrous calcaneonavicular coalition. Note the elongated tubular extension of the anterior calcaneus seen on the lateral film (arrows) compared to the unaffected side.
-
CT scan in a patient with unilateral calcaneonavicular coalition. Note pseudoarthrosis between the calcaneus and navicular bones (arrow).
-
MRI in a patient with calcaneonavicular coalition. Note pseudoarthrosis between the calcaneus and navicular bones (arrows).
-
Talocalcaneal coalition. Lateral radiograph of the foot reveals a classic C sign (arrows), which is a C-shaped line formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali. The C sign is a reliable indicator of subtalar coalition on lateral radiographs.
-
Talocalcaneal coalition. CT scan. Note the fusion of the sustentacular articulation with solid bone obliterating the joint.
-
Talocalcaneal coalition. MRI shows the fusion of the sustentacular articulation with solid bone obliterating the joint (arrow).




